Multiple Sclerosis (MS) is a neurological disease caused by demyelination or breakdown of the myelin coating around the nerve cells (1). This is referred to as a neurodegeneration where the physical structure of the nerve is compromised, much like the coating around an electrical wire being chipped or stripped away. Common symptoms of MS are sensory symptoms in the extremities or face, unilateral visual loss, acute or subacute motor weakness of the muslces, diplopia (double vision), gait disturbance and balance problems, Lhermitte sign (electric shock-like sensations that run down the back and/or limbs upon flexion of the neck), vertigo, bladder problems, loss of control of a limb, and pain.
Initially, and for many years, the degeneration seen in multiple sclerosis (MS) was thought to occur because of an acute inflammatory attack on the cells by dis-regulated immune cells crossing the blood brain barrier. However, treatments focused on modulating the inflammatory attack seem to have no effect on the degeneration and demyelination. Thus, the actual definitive cause of this demyelination and neuro-degeneration has eluded us since 1868, when Jean-Martin Charcot first described it.
Recent studies point to evidence that this demyelation may be due to degeneration or breakdown of the nerve cell’s ability to use glucose as a primary fuel (2, 3). It is now theorized that MS may be due to a combination of degeneration and localized inflammation related to poor glucose uptake causing the demyelination which is seen in a number of MS cases (4, 5, 6).
A. Normal nerve cell with intact myelin sheath around the axon. B. Demyelinated axion nerve losing its ionic charge due to escape of potassium. C. Radio-labled tracer allowing visualization of demyelination on PET Scan
With this dual concept in mind, ketogenic diets have demonstrated some promising results when used with neurological diseases including MS. Ketogenic diets have been used in the treatment of epilepsy since 500 B.C. and in the treatment of obesity since 1860. It is now becoming apparent that ketogenic diets may play a very significant role in the treatment of neurological disease because of two-fold effects that arise when ketones become the primary fuel for the body.
First, when a person becomes keto-adapted and ketones are used as the primary fuel, instead of glucose, the body up-regulates mitochondria to use the ketones for fuel. As the ketone level rises, the need for glucose diminishes. This provides the nerve cell an alternative fuel source if glucose metabolism is impaired. It also decreases the need and production of insulin, a known hormone heavily involved in stimulating inflammation and inflammatory responses.
The second effect of a ketogenic diet is this favorable effect on inflammation. It has been demonstrated that a ketogenic diet decreases reactive oxygen species, increased production of superoxide dismutase and catalayse, all of which notably decrease the inflammatory effects of oxidative stress (9,10, 11). A ketogenic diet also is well known to raise glutithione levels, another anti-oxidant that decreases inflammation and oxidative stress (12-16). This same anti-inflammatory and keto-adaptation effect can be obtained from intermittent fasting.
To date, studies in patients with neurologic diseases like MS, Alzheimer’s disease using ketogenic diets have had positive results in memory, cognition and diminished inflammation with evidence of halting or reversing the chronic demyelination (17,18, 19). Still somewhat theoretical, the evidence points to effective dietary treatment and prevention for multiple sclerosis and other degenerative neurological diseases like Alzheimer’s Disease.
References:
J. M. Pearce, “Historical descriptions of multiple sclerosis,” European Neurology, vol. 1, no. 1, pp. 49–53, 2005.
C.-A. Castellano, S. Nugent, N. Paquet et al., “Lower brain 18F-fluorodeoxyglucose uptake but normal 11C-acetoacetate metabolism in mild Alzheimer’s disease dementia,” Journal of Alzheimer’s Disease, vol. 43, no. 4, pp. 1343–1353, 2014.
S. Nugent, S. Tremblay, K. W. Chen et al., “Brain glucose and acetoacetate metabolism: a comparison of young and older adults,” Neurobiology of Aging, vol. 35, no. 6, pp. 1386–1395, 2014.
H. Lassmann, W. Brück, and C. F. Lucchinetti, “The immunopathology of multiple sclerosis: an overview,” Brain Pathology, vol. 17, no. 2, pp. 210–218, 2007.
C. Confavreux and S. Vukusic, “Natural history of multiple sclerosis: a unifying concept,” Brain, vol. 129, no. 3, pp. 606–616, 2006.
P. K. Stys, G. W. Zamponi, J. van Minnen, and J. J. G. Geurts, “Will the real multiple sclerosis please stand up?” Nature Reviews Neuroscience, vol. 13, no. 7, pp. 507–514, 2012.
P. G. Nijland, I. Michailidou, M. E. Witte et al., “Cellular distribution of glucose and monocarboxylate transporters in human brain white matter and multiple sclerosis lesions,” Glia, vol. 62, no. 7, pp. 1125–1141, 2014.
L. C. Costantini, L. J. Barr, J. L. Vogel, and S. T. Henderson, “Hypometabolism as a therapeutic target in Alzheimer’s disease,” BMC Neuroscience, vol. 9, supplement 2, article S16, 2008.
P. G. Sullivan, J. E. Springer, E. D. Hall, and S. W. Scheff, “Mitochondrial uncoupling as a therapeutic target following neuronal injury,” Journal of Bioenergetics and Biomembranes, vol. 36, no. 4, pp. 353–356, 2004.
P. G. Sullivan, N. A. Rippy, K. Dorenbos, R. C. Concepcion, A. K. Agarwal, and J. M. Rho, “The ketogenic diet increases mitochondrial uncoupling protein levels and activity,” Annals of Neurology, vol. 55, no. 4, pp. 576–580, 2004.
T. Shimazu, M. D. Hirschey, J. Newman et al., “Suppression of oxidative stress by β-hydroxybutyrate, an endogenous histone deacetylase inhibitor,” Science, vol. 339, no. 6116, pp. 211–214, 2013.
S. G. Jarrett, J. B. Milder, L.-P. Liang, and M. Patel, “The ketogenic diet increases mitochondrial glutathione levels,” Journal of Neurochemistry, vol. 106, no. 3, pp. 1044–1051, 2008.
J. B. Milder, L.-P. Liang, and M. Patel, “Acute oxidative stress and systemic Nrf2 activation by the ketogenic diet,” Neurobiology of Disease, vol. 40, no. 1, pp. 238–244, 2010.
N. Dupuis, N. Curatolo, J. F. Benoist, and S. Auvin, “Ketogenic diet exhibits anti-inflammatory properties,” Epilepsia, vol. 56, no. 7, pp. e95–e98, 2015.
D. Y. Kim, J. Hao, R. Liu, G. Turner, F.-D. Shi, and J. M. Rho, “Inflammation-mediated memory dysfunction and effects of a ketogenic diet in a murine model of multiple sclerosis,” PLoS ONE, vol. 7, no. 5, Article ID e35476, 2012.
Y.-H. Youm, K. Y. Nguyen, R. W. Grant et al., “The ketone metabolite β-hydroxybutyrate blocks NLRP3 inflammasome—mediated inflammatory disease,” Nature Medicine, vol. 21, no. 3, pp. 263–269, 2015.
A. Ramm-Pettersen, K. O. Nakken, I. M. Skogseid et al., “Good outcome in patients with early dietary treatment of GLUT-1 deficiency syndrome: results from a retrospective Norwegian study,”Developmental Medicine and Child Neurology, vol. 55, no. 5, pp. 440–447, 2013.
Y. Ito, H. Oguni, S. Ito, M. Oguni, and M. Osawa, “A modified Atkins diet is promising as a treatment for glucose transporter type 1 deficiency syndrome,” Developmental Medicine and Child Neurology, vol. 53, no. 7, pp. 658–663, 2011.
M. Storoni and GT Plant, “The Therapeutic Potential of the Ketogenic Diet in Treating Progressive Multiple Sclerosis,” Multiple Sclerosis International, vol. 2015, Article ID 681289, 9 pages, 2015.
The image above has nine dots within a square. Your task, using only four lines is to connect ALL nine dots WITHOUT ever raising your pen, pencil or finger (Please don’t use a sharpie on your computer screen . . . it doesn’t come off).
You may have seen this puzzle previously . . . it’s made its rounds in corporate training circles. But the underlying principle remains true. The solution requires you to expand your thinking or to “think outside the box.”
Whenever you find yourself on the side of the majority, it is time to pause and reflect. (Mark Twain)
Why should we limit ourselves to thinking outside the box. Can’t we just get rid of the box?
True discovery consists in seeing what everyone has seen . . . then, thinking what no one has thought.
The answer can be found when those four lines are used beyond the box our mind creates:
What good has the box done us? People were burned at the stake because they refused to believe the Earth was not the center of the universe. People were beheaded because they had a sneaking suspicion that the world was not flat.
Why is it so very hard to accept that our weight gain and diabetes are driven by a hormonal signal, and not by gluttony or caloric intake of fat? The definition of insanity is doing the same thing repetitively and expecting a different outcome. How long have you been restricting calories and fat with only minimal or no improvement in your weight, blood sugar, cholesterol or general feeling of health?
The main problem with the current thought model, or dogma, on the obesity’s cause is that it does not account for metabolic syndrome. Metabolic syndrome is insulin resistance. It is an over production of insulin in the presence of ANY form of carbohydrate (sugar or starch).
In the practice of medicine over the last 15 years, I noticed that a very interesting pattern emerged. There was always a spike in fasting and postprandial insulin levels 5-10 years prior to the first abnormal fasting and postprandial blood sugars. These patients were exercising regularly and eating a diet low in fat. But they saw continued weight gain and progressed down the path of metabolic syndrome. 10-15 years later, they fall into the classification of type II diabetes. What I now lovingly refer to as stage IV insulin resistance.
The only thing that seems to halt this progressive process with any degree of success is carbohydrate restriction. Fasting insulin levels return to normal, weight falls off, and the diseases of civilizations seem to disappear as insidiously as they arose.
So you tell me, is the world flat? Is the Earth the center of the universe?
What is a low carbohydrate or ketogenic diet? 15 years of practical in the trenches experience have helped me develop a very simple program to help you lose and maintain your weight. Access to this program, video help and access to blog articles at your fingertips are offered through my online membership site.
You can also hear me each week a I discuss low carbohydrate, paleolithic and ketogenic diets with the Legendary Jimmy Moore on KetoTalk.com
Good morning from Arizona. I’ve had a few people ask about how gut health relates to a ketogenic diet. This is a great question and one that I think can be answered best by taking a closer look at my natural koi pond and learning a little about pond scum.
So, sit back and look at the similaries between your gut and how nature balances a pond system: Katch.me
Or you can watch the video below:
The four tenets of health that we touch on above that are essential to understand before you can understand gut health:
The body is a unit and works as such with all parts enhancing the whole
The body is capable of self-regulation, self-healing, and health-maintenance
Structure & function are reciprocally interrelated
Rational treatment of the body must be based upon understanding the principles above and assisting or augmenting those principles
Keys to gut health and pond balancing that we touch on:
Remove the toxins from entering the system like:
Antibiotic overuse
Caffeine
Artificial Fat
Artificial Sweeteners
Repair the system and it’s ability to balance the system
Takes time
Provide structure for the bacteria to which it can bind
Provide essential vitamins and minerals like KetoEnhance & Omega-3 fatty acids
Periodic Fasting
Restore the bacteria or flora of the system
Prebiotics (fermented foods like sauerkraut, kimchi, Japanese natto, etc.)
Probiotics like Dietary KetoBalance (can be purchased in the office)
Replace the salts and pH balance where necessary
Replace electrolytes
Limit things that shift the pH balance
Hope this gives you a starting point for your New Year!!
It’s Here! KetoTalk with Jimmy Moore and the Doc premiers today. You can link to it here: http://ketotalk.com/2015/12/0-keto-talk-with-jimmy-moore-the-doc-debuts/ or click on the menu bar above to take you to KetoTalk.com.
The show has been picked up by iTunes, but it takes anywhere from 3-7 days to appear in their search menus, so be patient and while iTunes assimilates it, you can always hear it or download it from KetoTalk.com.
We want to hear your feed back so please tell us what you think and rate us on iTunes when it is available.
KetoTalk with Jimmy & the Doc (the legendary podcaster Jimmy Moore from Livin’ La Vita Low Carb and his newest co-host, your’s truly, Dr. Adam Nally) makes its debut this Thursday, December 31st, 2015 on iTunes. You can see the show notes at KetoTalk.com (will be up and live on January 1st, 2016).
Throughout the exciting month of January, we will be airing a brand new episode of this 20-minute show each Thursday and a special bonus episode available on Sundays just to wet your ketogenic appetite and to kick off the podcast in its first month. Then, in February we’ll settle in to our regular Thursday time slot each week.
New podcasts can take a few days to assimilate into #iTunes, so don’t get discouraged if you don’t immediately see it up on iTunes. However, you can always find them at KetoTalk.com. Jimmy and I look forward to being your go-to, Ketogenic Lifestyle source for the latest and greatest in treating the diseases of civilization!
Get a sneak peek of our new show on tomorrow’s (Wednesday, December 30th) episode of “The Livin’ La Vida Low-Carb Show” where you can hear my interview with Jimmy as a preview what is sure to be a big hit in the #keto community. Thanks in advance for supporting our new podcast!
Today’s Periscope was an exciting one. Do you really need a pre- or post-workout shake or meal? How much protein do you need? What’s the difference between ketosis and ketoacidosis? Is Dr. Nally a ketogenic cheerleader? Get your answers to these and many more questions asked by some wonderful viewers this evening on today’s PeriScope.
Be sure to check out Dr. Nally’s new podcast called “KetoTalk with Jimmy and the Doc” with the veteran podcaster Jimmy Moore on KetoTalk.com. The first podcast will be available on December 31, 2015. KetoTalk with Jimmy and the Doc will be available for download for free on iTunes.
What are the three things you need to successfully weather the holidays with your ketosis lifestyle? What does a raindeer on a motorcycle look like? How does insulin resistance effect kidney stones and gout? How do you get back on track if you fall off the ketosis wagon? These and many more questions are answered by Dr. Adam Nally on tonight’s PeriScope.
You can see the video stream including the comment roll here at katch.me/docmuscles. Or you can watch the video below:
How do you know if you're insulin resistant? What questions need to be asked? What should your numbers be? And, many other great ketosis questions. Also, why does Dr. Nally look like he has dirt on his chin? See it here . . .
“I’ve tried your low-carb diet, Dr. Nally, and it didn’t work.”
“Hmm . . . really?” If you’re mumbling this to yourself, or you’ve said it to me in my office, then lets have a little talk. You’ve probably been subjected to the common ketosis killers.
I’ve heard this statement before. It’s not a new statement, but it’s a statement that tells me we need to address a number of items. If you’ve failed a low carbohydrate diet, I’d suspect you are pretty severely insulin resistant or hyperinsulinemic. You probably never really reached true ketosis. I’d want to have you checked out by your doctor to rule out underlying disease like hypothyroidism, diabetes, other hormone imbalance, etc.
Nutritional Ketosis is Most Effective as a Lifestyle Change
Next, switching to a low-carbohydrate lifestyle is literally a “lifestyle change.” It requires that you understand a few basic ketosis principles. And, it takes the average person 3-6 months to really wrap their head around what this lifestyle means . . . and, some people, up to a year before they are really comfortable with how to eat and function in any situation.
I assume, if you are reading this article, that you’ve already read about ketosis and understand the science behind it. If not, please start your reading with my article The Principle Based Ketogenic Lifestyle – Part I and Ketogenic Principles – Part II. If this is the case, then please proceed forward, “full steam ahead!”
There are usually a few areas that are inadvertently inhibiting your body transformation, so let’s get a little personal.
Nutritional Ketosis is a Very Low Carbohydrate Diet
First, this is a low carbohydrate diet. For weight loss, I usually ask people to lower their carbohydrate intake to less than 2o grams per day. How do you do that? (A copy of my diet is accessible through my membership site HERE.) You’ve got to begin by restricting all carbohydrates to less than 20 grams per day. Any more than 20 to 30 grams per day will cause an insulin release from the pancreas and stimulate fat storage of both carbohydrate and fat for the next 10-12 hours, commonly killing ketosis. Keep a dietary journal to record your progress, your cravings, your successes and failures. I’m going to want to see it and review it with you if you see me.
No, I don’t believe in “Net Carbs.” Net Carbs are a sales gimmick to get you to buy “artificial food” that keeps you coming back for “artificial food” and halts your weight loss (you’ll see why shortly). You’re going to lose the most weight and feel your best when you eat real food. I do allow for the subtraction of real fiber, specifically non-cooked, non-blended, non-juiced leafy greens (If you cook, blend or juice a leafy green, it activates more carbohydrate availability). Leafy greens are real fiber. You can subtract them. In fact, I recommend eating 1-3 cups of leafy greens per day to help bowel function & provide necessary folic acid, but, everything else is “carbage.” Avoid it.
Yes, cottage cheese and yogurt contain carbohydrates. Be very cautious with them.
Alcohol also halts your weight loss. It’s not the sugar in the alcohol I’m worried about, the distilling process changes the sugar to alcohol, however, alcohol stimulates an insulin response after the alcohol is metabolized in the liver with a SIMILAR RESPONSE to regular sugar.
To Effectively Maintain Nutritional Ketosis, You MUST get adequate Protein
Second, this is a low carbohydrate, moderate protein, high fat lifestyle. N0 . . . it is NOT a high protein diet! However, so many of my patients don’t eat enough protein that they feel like it is a “high protein diet.”
Protein is essential for the building and maintaining of muscle, connective tissue and a number of other enzymatic reactions in your body. However, in patients who are morbidly obese [people with a body mass index (BMI) over 50], excess protein intake can cause fat to be stored by producing an excessive insulin response. In these patients we initially moderate protein. Excess sugars and a number of proteins, in the presence of a high insulin response, are converted to triglyceride (the soft squishy stuff inside the fat cells that make them plump) and stocked away inside your adipose tissue. Excessive protein, especially the amino acids argenine, leucine and tryptophan are common ketosis killers, not because they are converted to sugar, but because they stimulate and insulin response all by themselves.
If you don’t fall into the morbidly obese category (BMI over 50). Then, I encourage you to use the protein levels below.
Initially, I ask my patients to focus on lowering their carbohydrate intake and I don’t really worry about protein. (It is often hard enough to figure out what the difference between a carbohydrate and a protein in the first month or two if you’ve never had any nutrition background.) Most people begin losing weight just by lowering carbohydrates over the first few months. Once you figure out how to lower your carbohydrates, if your weight loss is not moving and your pants are not getting looser, then you’re probably eating too much protein.
How much protein do you need? It’s pretty easy to calculate and is based on your height and gender. Your basic protein needs to maintain muscle, skin and hair growth are as follows:
70 grams or higher for women per day
120 grams or higher for men per day.
However, these levels are WAY TOO LOW for weight loss and maintaining good health. Because we now know that protein acts as a hormone in a number of ways, in my office I recommend women get 80-90 grams of protein per day, and men should get > 150 grams of protein per day.
This also goes for protein powders and protein shakes. Many of these have 25-40 grams of protein in them per serving, so be careful with their use.
Nutritional Ketosis is a High Fat Diet
Third, this is a high fat lifestyle. Yes, I want you to INCREASE your fat intake. I’m going to repeat that, again, just for clarity, . . . . INCREASE your fat intake. Increase it to around 50% of your total calories, . . . 70% of your total calories if you can do it. Not enough fat is a common ketosis killer.
“What?! Won’t that cause heart disease and stroke and make my cholesterol worse?!!!”
I know, take a big deep breath . . . (you may even need to breath into a paper bag for a minute if you begin hyperventilating).
No, it will not raise your cholesterol, cause heart disease, or cause a stroke. If you have lowered your carbohydrate intake to less than 20 grams per day, then there is NO hormonal signal for you to make more bad cholesterol, worsen heart disease, or cause a stroke. In fact, there is great data showing that increasing your fat and lowering your carbohydrates reverses the blockage in the arteries. I see this reversal every single day in my clinic through the application of ketogenic diets.
If we remove carbohydrate as your primary fuel, you must replace it with something else.That something else should be fat. Protein must be moderated, as it will also be stored as fat if you eat too much. So, if the carbohydrates are kept low, fat intake can be increased and the body will pick the fat it wants and essentially throw the rest out without raising cholesterol, causing weight gain or causing heart disease. This is why we want you to use good natural animal fats like butter, hard cheese, olive oil, coconut oil, avocado, etc. Look for fats highest in omega-3 fatty acids as these decrease inflammation and improved weight loss. Look for meats highest in fat like red meat (55% fat) and pork (45% fat). Take the food pyramid and flip it over.
Check Your Sweeteners At the Door
The fourth common ketosis killer and culprit in halting your weight loss is artificial sweeteners. There are quite a few of them. Most of them WILL cause an insulin response (exactly what we don’t want for weight loss) with minimal to no rise in blood sugar. Raising blood sugar doesn’t matter, if the insulin is being stimulated . . . “you’re gonna gain weight for the next 10-12 hours.” I wrote an article for you to print off and hang on your fridge, upload it to your iPhone or carry it with you in your purse to the grocery store. (If you’re a man and you’re carrying a purse, please don’t tell me about it.) You can find the article here: The Skinny About Sweeteners. The short list of those sweeteners that are OK to use and cook with, and do not increase insulin response, can be found here in my Amazon Store.
Don’t Even Start with Coffee Creamers
Fifth on my list is coffee creamer. Coffee creamer contains corn syrup solids (another very special name for . . . SUGAR!!) and/or maltodextrin (SUGAR’s married name!). If you must put something in your coffee, then use real heavy cream (pure tasty fat) or real butter. It will taste much better (I’m told – I don’t drink coffee personally) and you won’t get an insulin spike 2-3 hours later and begin craving more coffee and donuts.
Yes, “Half & Half” is half fat and half sugar. . . avoid it too!!
Ketosis Killing Medications
The sixth culprit in halting weight loss is medications. Please talk to your doctor before making ANY changes in your medications as suddently stopping them can be hazardous to your health. Those highest on my list for stopping your weight loss are Glyburide (glipizide), insulin, & steroids like prednisone. A more complete list of medications that will halt your weight loss can be found on my on my ketogenic diet plan. If you are on any prescription medications, please talk to your doctor or to a physician board certified in obesity medicine treatment about how to adjust or wean these medications in a way that is safe and appropriate for your individual needs.
Estrogen
The seventh common culprit in halting weight loss is a lack of estrogen in menopausal or post-menopausal women. About 20% of women that I see in my practice who are over 55 years old, need some degree of estrogen replacement before they are able to lose weight. Estrogen plays a very large role in regulation of the metabolism and when deficient, causes weight retention or weight gain. Talk to your doctor about the risks and benefits of estrogen for you individually in this situation.
For many years, we’ve thought that caffeine was great for weight loss. However, we are finding, clinically, that too much caffeine can also cause a stress response by raising cortisol, releasing glycogen, thereby stimulating an insulin response and bringing your weight loss to a screeching halt. How much caffeine? . . . The jury is still out . . . and remains to be determined. But, I am currently under going an n=1 experiment on myself (as many of you know, I loved Diet Dr. Pepper. But I had to give it up). I’ll keep you posted . . .
Look closely at these eight issues. Correcting them usually solves most plateaus with weight loss and improves blood pressure, blood sugar and cholesterol control dramatically.
Adrenal Fatigue? Adrenal Insufficiency? Cortisol? PseudoCushing’s Syndrome? What do these terms mean and why are they all over the internet these days? And, what do they have to do with your weight loss?
This was our topic this evening on PeriScope. Katch Dr. Nally speak about this topic with rolling comments at Katch.me/docmuscles. Or you can watch the video below:
If you’re not sure about what this is, you’re not alone. I think I’ve heard the term “Adrenal Fatigue” at lease four times a day for the last three months. If you ask your doctor, they’ll probably scratch their heads too. The funny thing is that “Adrenal Fatigue” isn’t a real diagnosis, but it is all over the internet and it shows up in the titles of magazines in the grocery store every day. There’s even and “Adrenal Fatigue For Dummies” so it must be real, right?!
No. It isn’t a real diagnosis. It is a conglomeration of symptoms including fatigue, difficulty getting out of bed in the morning, and “brain fog” that have been lumped together to sell an “adrenal supplement.” (Sorry, but that’s really what it is all about.) Do a Google search and the first five or six sites describing adrenal fatigue claim the solution is taking their “special adrenal supplement.”
I know what you’re thinking, “Your just a main stream, Western Medicine doctor, Dr. Nally, you wouldn’t understand.” Actually, I do understand.
Adrenal fatigue has risen in popularity as a “lay diagnosis” because many patients show up at their doctors office with significant symptoms that actually interfere with their ability to function, and after all the testing comes back negative for any significant illness, they are told that they are normal. But the patient still has the symptoms and no answer or treatment has been offered. It’s discouraging. . . very discouraging.
That’s because the symptoms are actually the body’s response to chronic long term stress. Many of my patients, myself included, have found themselves “stuck” in their weight loss progression, feeling fatigued, struggling to face the day, with a number of symptoms including cold intolerance, memory decline, difficulty concentrating, depression, anxiety, dry skin, hair loss, and even infertility in some cases. Is it poor functioning adrenal glands? No, your feeling this way because the adrenal glands are actually doing their job!!
If the adrenal glands weren’t working you’d experience darkening of the skin, weight loss, gastric distress, significant weakness, anorexia, low blood pressure, and low blood sugar. The symptoms are actually called Addison’s disease and it is actually fairly rare (1 in 100,000 chance to be exact). So what is causing the symptoms you ask?
There are a number of reasons, but one that I am seeing more and more frequently is “Pseudo-Cushings’s Syndrome.” Pseudo-Cushing’s Syndrome is a physiologic hypercortisolism (over production of cortisol) that can be caused by five common issues:
Chronic Physical Stress
Severe Bacterial or Fungal Infections that Go Untreated
Malnutrition or Intense Chronic Exercise
Psychological Stress – including untreated or under-treated depression, anxiety, post-traumatic stress, or dysthymia (chronic melancholy)
Alcoholism
The psychiatric literature suggest that up to 80% of people with depressive disorders have increased cortisol secretion (1,2,3). People with significant stressors in their life have been show to have an increased corsiol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing a daily, cyclic over production of cortisol and then normalization of cortisol after resolution of the stressor. This cortisol response is not high enough to lead to a true Cushing’s Syndrome, but has the effect of the symptoms listed above and begins with limiting ones ability to loose weight.
I’m convinced that this is becoming more and more prevalent due to the high paced, high-stress, always on, plugged in, 24 hour information overload lives we live.
What is cortisol? It is a steroid hormone made naturally in the body by the adrenal cortex (outer portion of the adrenal gland). Cortisol is normally stimulated by a number of daily activities including fasting, awakening from sleep, exercise, and normal stresses upon the body. Cortisol release into the blood stream is highest in the morning, helping to wake us up, and tapers into the afternoon. Cortisol plays a very important role in helping our bodies to regulate the correct type (carbohydrate, fat, or protein) and amount of fuel to meet the bodies physiologic demands that are placed upon it at a given time (4,5,6).
Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids or proteins into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues (by stimulating insulin production) and turns on the maturation process of adipocytes (it makes your fat cells age – nothing like having old fat cells, right?!) In the process, cortisol suppresses the immune system through an inhibitory effect designed to decrease inflammation during times of stress (7,8,9). If this was only occurring once in a while, this cascade of hormones acts as an important process. However, when cortisol production is chronically turned up, it leads to abnormal deposition of fat (weight gain), increased risk of infection, impotence, abnormal blood sugars, brain fog, head
aches, hypertension, depression, anxiety, hair loss, dry skin and ankle edema, to name a few.
The chronic elevation in cortisol directly stimulates increased insulin formation by increasing the production of glucose in the body, and cortisol actually blunts or block-aids the thyroid function axis. Both of these actions halt the ability to loose weight, and drive weight gain.
Cortisol also increases appetite (10). That’s why many people get significant food cravings when they are under stress (“stress eaters”). Cortisol also indirectly affects the other neuro-hormones of the brain including CRH (corticotrophin releasing hormone), leptin, and neuropeptide Y (NPY). High levels of NPY and CRH and reduced levels of leptin have also been shown to stimulate appetite and cause weight gain (10-11).
How do you test for Pseudo-Cushing’s Syndrome?
Testing can be done by your doctor with a simple morning blood test for cortisol. If your cortisol is found to be elevated, it needs to be repeated with an additional 24 hour urine cortisol measurement to confirm the diagnosis. If Cushing’s Syndrome is suspected, some additional blood testing and diagnostic imaging will be necessary. Pseudo-Cushing syndrome will demonstrate a slightly elevated morning cortisol that doesn’t meet the criteria for true Cushing’s type syndrome or disease.
How do you treat it?
First, the stressor must be identified and removed. Are you getting enough sleep? Is there an underlying infection? Is there untreated anxiety or depression present? Are you over-exercising? These things must be addressed.
Second, underlying depression or anxiety can be treated with counseling, a variety of weight neutral anti-depressant medications or a combination of both. Many of my patients find that meditation, prayer, and journaling are tremendous helps to overcoming much of the anxiety and depression they experience.
Third, adequate sleep is essential. Remove the television, computer, cell phone, iPad or other electronic distraction from the bedroom. Go to bed at the same time and get up at the same time each day. Give yourself time each day away from being plugged in, logged in or on-line.
Fourth, mild intensity (40% of your maximal exertion level) exercise 2-3 days a week was found to lower cortisol; however, moderate intensity (60% of your maximal exertion level) to high intensity (80% of your maximal exertion level) exercise was found to raise it (12). A simple 20 minute walk, 2-3 times per week is very effective. Find a hobby that you enjoy and participate in it once or twice a week. Preferably, a hobby that requires some physical activity. The activity will actually help the sleep wake cycles to improve.
Fifth, follow a low carbohydrate or ketogenic diet. Ketogenic diets decrease insulin and reverse the effect of long term cortisol production. Ketogenic diets a have also been shown to decrease or mitigate inflammation by reducing hyperinsulinemia commonly present in these patients (13).
So, the take home message is . . . take your adrenal glands off of overdrive.
References:
Pfohl B, Sherman B, Schlechte J, Winokur G. Differences in plasma ACTH and cortisol between depressed patients and normal controls. Biol Psychiatry 1985; 20:1055.
Pfohl B, Sherman B, Schlechte J, Stone R. Pituitary-adrenal axis rhythm disturbances in psychiatric depression. Arch Gen Psychiatry 1985; 42:897.
Gold PW, Loriaux DL, Roy A, et al. Responses to corticotropin-releasing hormone in the hypercortisolism of depression and Cushing’s disease. Pathophysiologic and diagnostic implications. N Engl J Med 1986; 314:1329.
Ely, D.L. Organization of cardiovascular and neurohumoral responses to stress: implications for health and disease. Annals of the New York Academy of Sciences (Reprinted from Stress) 771:594-608, 1995.
McEwen, B.S. The brain as a target of endocrine hormones. In Neuroendocrinology. Krieger and Hughs, Eds.: 33-42. Sinauer Association, Inc., Massachusetts, 1980.
Vicennati, V., L. Ceroni, L. Gagliardi, et al. Response of the hypothalamic- pituitary-adrenocortical axis to high-protein/fat and high carbohydrate meals in women with different obesity phenotypes. The Journal of Clinical Endocrinology and Metabolism 87(8) 3984-3988, 2002.
Wallerius, S., R. Rosmond, T. Ljung, et al. Rise in morning saliva cortisol is associated with abdominal obesity in men: a preliminary report. Journal of Endocrinology Investigation 26: 616-619, 2003.
Epel, E.S., B. McEwen, T. Seeman, et al. Stress and body shape: stress-induced cortisol secretion is consistently greater among women with central fat.
Psychosomatic Medicine 62:623-632, 2000.
Tomlinson, J.W. & P.M. Stewart. The functional consequences of 11_- hydroxysteroid dehydrogenase expression in adipose tissue. Hormone and Metabolism Research 34: 746-751, 2002.
Epel, E., R. Lapidus, B. McEwen, et al. Stress may add bite to appetite in women: a laboratory study of stress-induced cortisol and eating behavior.Psychoneuroendocrinology 26: 37-49, 2001.
Cavagnini, F., M. Croci, P. Putignano, et al. Glucocorticoids and neuroendocrine function. International Journal of Obesity 24: S77-S79, 2000.
Hill EE, Zack E, Battaglini C, Viru M, Vuru A, Hackney AC. Exercise and circulating cortisol levels: the intensity threshold effect. J Endocrinol Invest. 2008. Jul;31(7):587-91.
Fishel MA et al., Hyperinsulinemia Provokes Synchronous Increases in Central Inflammation and β-Amyloid in Normal Adults. Arch Neurol. 2005;62(10):1539-1544. doi:10.1001/archneur.62.10.noc50112.
What laboratory testing is necessary when you start your weight loss journey on a Ketogenic, Low-Carbohydrate, Paleolithic or any other dietary changes? Why do you need them and what are you looking for? We discuss these questions and others on today’s PeriScope. Lots of questions from around the world to day . . . this one lasted a bit longer than normal . . . 45 minutes to be specific. But it’s a good one because of all of your fantastic questions! You really don’t want to miss this one.
You can see the video below or watch the video combined with the rolling comments here on Katch.me/docmuscles.
A list of the labs that we discussed are listed below:
Fasting insulin with 100 gram 2 or 3 hour glucose tolerance test with insulin assay every hour
CMP
CBC
HbA1c
Leptin
Adiponectin
C-Peptid
NMR Liprofile or Cardio IQ test
Lipid Panel
Urinalysis
Microalbumin
Apo B
C-reactive protein
TSH
Thyroid panel
Thyroid antibodies
AM Cortisol
This list will at least get one started, provide the screening necessary to identify insulin resistance (Diabetes In-Situ), Impaired fasting glucose, diabetes and allow for screening for a number of the less common causes of obesity.
I would highly recommend that you get these through your physician’s office so that appropriate follow up can be completed. These labs will need to be interpreted by your physician, someone who understands and is familiar with various causes of obesity.
I just completed my reading of Dr. Joseph Kraft’s Diabetes Epidemic & You. This text originally printed in 2008 and was re-published in 2011. I am not really sure why I have never seen this book until now, but I could not put it down. I know, I am a real life medical geek. But seriously, you should only read this book if you are concerned about your health in the future. Otherwise, don’t read it.
For the first time in 15 years, someone has published and validated what I have been seeing clinically in my office throughout my career. Dr. Kraft is a pathologist that began measuring both glucose and insulin levels through a three hour glucose tolerance blood test at the University of Illinois, St. Joseph Hospital in Chicago. This test consists of checking blood sugar and insulin in a fasted state, and then drinking a 100 gram glucose load followed by checking blood sugar and insulin at the 30, 60, 120 and 180 minute marks (a total of three hours).
Dr. Kraft completed and recorded this test over a period of almost 30 years on 14,384 patients between 1972 and 1998. His findings are landmark and both confirm and clarify the results that I have seen and suspected for years.
I am convinced that our problem with treating obesity, diabetes and the diseases of civilization has been that we defined diabetes as a “disease” based on a lab value and a threshold instead of identifying the underlying disease process. We have been treating the symptoms of the late stage of a disease that started 15 to 20 years before it is ever actually diagnosed. Diabetes is defined as two fasting BS >126, any random blood sugar >200, or a HbA1c >6.5%. (Interestingly this “disease” has been a moving target. When I graduated from medical school it was two fasting blood sugars >140 and the test called hemoglobin A1c (HbA1c) that we use today for diagnosis didn’t even exist). The semantics associated with this problem is that many of us recognize that the disease is not actually diabetes. The disease is (as far as we understand it today) insulin resistance or hyperinsulinemia. This is where Dr. Kraft’s data is so useful. Diabetes, as it is defined above, is really the fourth stage of insulin resistance progression over a 15-20 year period and Dr. Kraft’s data presents enormous and very clear evidence to that effect.
When I first entered private practice 15 years ago, I noticed a correlation and a very scary trend that patients would present with symptoms including elevated triglycerides, elevated fasting blood sugar, neuropathy, microalbuminuria, gout, kidney stones, polycystic ovarian disease, coronary artery disease and hypertension that were frequently associated with diabetes 5-15 years before I ever made the diagnosis of diabetes mellitus. I began doing 2 hour glucose tolerance tests with insulin levels and was shocked to find that 80-85% of those people were actually diabetic or very near diabetic in their numbers. The problem with a 2 hour glucose tolerance test, is that if you are diabetic or pre-diabetic, you feel miserable due to the very profound insulin spike that occurs. A few patients actually got quite upset with me for ordering the test, both because of how they felt after the test, and the fact that I was the only physician in town ordering it. So, in an attempt to find an easier way, I found that the use of fasting insulin > 5 nU/dl, triglycerides > 100 mg/dl and small dense LDL particle number > 500 correlated quite closely clinically with those patients that had positive glucose tolerance tests in my office. There is absolutely no data in the literature about the use of this triangulation, but I found it to be consistent clinically.
I was ecstatic to see that Dr. Kraft plowed through 30 years and over 14,000 patients with an unpleasant glucose tolerance test and provided the data that many of us have had to clinically triangulate. (I’m a conservative straight white male, but if Dr. Kraft would have been sitting next to me when I finished the book this afternoon, I was so excited that I probably would have kissed him.)
Insulin resistance or hyperinsulinemia (the over production of insulin between 2-10 times the normal amount after eating carbohydrates) is defined as a “syndrome” not a disease. What Dr. Kraft points out so clearly is that huge spikes in insulin occur at 1-2 hours after ingestion of carbohydrates 15-20 years prior to blood sugar levels falling into the “diabetic range.” He also demonstrates, consistently, the pattern that occurs in the normal non-insulin resistant patient and in each stage of insulin resistance progression.
The information extrapolated from Dr. Kraft’s research give the following stages:
Stages of insulin resistance by 3 hr OGTT extrapolated from “Diabetes Epidemic & You”
From the table above, you can see that the current definition of diabetes is actually the fourth and most prolifically damaging stage of diabetes. From the data gathered in Dr. Kraft’s population, it is apparent that hyperinsulinemia (insulin resistance) is really the underlying disease and that diabetes mellitus type II should be based upon an insulin assay instead of an arbitrary blood sugar number. This would allow us to catch and treat diabetes 10-15 years prior to it’s becoming a problem. In looking at the percentages of these 14,384 patient, Dr. Kraft’s data also implies that 50-85% of people in the US are hyperinsuliemic, or have diabetes mellitus “in-situ” (1). This means that up to 85% of the population in the U.S. is in the early stages of diabetes and is the reason 2050 projections state that 1 in 3 Americans will be diabetic by 2050 (2).
Insulin resistance is a genetically inherited syndrome, and as demonstrated by the data above has a pattern to its progression. It is my professional opinion that this “syndrome” was, and actually is, the protective genetic mechanism that protected groups of people and kept them alive during famine or harsh winter when no other method of food preservation was available. It is most likely what kept the Pima Indians of Arizona, and other similar groups, alive while living for hundreds of years in the arid desert. This syndrome didn’t become an issue among these populations until we introduced them to Bisquick and Beer.
The very fascinating and notably exciting aspect of this whole issue is that insulin resistance is made worse by diet and it is completely treatable with diet. This is where the low carbohydrate diet, and even more effective ketogenic diet or lifestyle becomes the powerful tool available. Simple carbohydrate restriction reverses the insulin spiking and response. In fact, I witness clinical improvement in the insulin resistance in patients in my office over 18-24 months every day. You can get a copy of my Ketogenic Diet here in addition to video based low carbohydrate dietary instruction.
Until we are all on the same page and acknowledge that diabetes is really the fourth stage of progression on the insulin resistance slippery slope, confusion and arguments about treatment approaches will continue to be ineffective in reducing the diseases of civilization.
This evening on PeriScope, we talked about the 10 things you can do to stay motivated on your low-carb lifestyle. A number of great questions were asked including:
How much carbohydrate should be restricted?
What labs should you be monitoring regularly?
What’s a normal blood sugar?
Why is Dr. Nally freezing in Denver?
Is fermented food good for you?
Why should you eat pickles and kimchi even when you’re not pregnant?
And, much much more . . . It’s like a college ketogenic course on overdrive . . . for FREE!!!
You can see the PeriScope with the comments rolling in real-time here: katch.me/docmuscles
Join me as we chew the phat of ketogenic lifestyles PeriScope style and answer many questions like, “Why do I get ‘hangry’?” What causes hypoglycemia? How many times a day should I eat? and many more . . .
We talk briefly about why 60% of people with insulin resistance may need methylated folic acid to help with B vitamin absorption/use and where it can be found. (See me recent article about this called The Power of a Good Vitamin.)
You can see the whole PeriScope conversation on Katch.me/docmuscles with the comments scrolling or you can see the video stream below:
A patient just sent this picture to me this evening. I got a good laugh out of it.
It brought up a couple of principles. So, Seriously, take just a moment and admire this pile of bacon. . .
First, it’s important that we take a moment and think about what is important in life. What really makes you tick? To those of us following a ketogenic lifestyle (low carb, moderate protein & high fat living), this represents food, fuel, taste and a great conversation tool. This pile of bacon forces one to think about what is really important in ones life.
This pile of bacon represents 2-3 weeks of breakfasts.
It represents wonderful flavor for a salad.
It becomes something wonderful to dip in guacamole.
Second, how much of this bacon can one following a ketogenic lifestyle have at a meal? That depends upon your need of protein. We base our basic protein need on a persons calculated ideal body weight. (No, your ideal body weight is not the weight you’re supposed to reach! It is a calculation based on height that gives us a starting point fro protein needs).
Many people have asked me how to calculate ideal body weight this week. I’ve provided the calculation below:
Ideal Body Weight (IBW) – Estimated in (kg) Males: IBW = 50 kg + 2.3 kg for each inch over 5 feet.
Females: IBW = 45.5 kg + 2.3 kg for each inch over 5 feet.
The average female needs 1.0 g of protein per kg of ideal body weight per day.
The average male needs 1.2 g protein per kg of ideal body weight per day.
If you are exercising more than 60 minutes 5 days per week then those values increase to 1.4 grams per kg for females and 1.6 grams per kg for males.
Example:
A 6 foot male’s IBW would be 50 kg + (2.3kg x 12 inches) = 77.6 kg
A 5 foot 4 inch females IBW would be 45.5 kg + (2.3kg x 4 inches) = 54.7 kg.
If you eat three times per day, then simply divide your IBW by 3 to get the maximum protein you need per meal.
What are the four most common mistakes I see in the office when it comes to weight loss? Watch Dr. Nally on today’s PeriScope as he answers that question and many others. You can see it here with the live stream comments on: https://www.katch.me/docmuscles/v/392e5d3e-bb28-3176-a03a-83433878a5ce
Yes, your fruit makes you fat just like your beer gives you a beer belly. . .
It is fascinating how similarly fructose (the sugar in fruit) and alcohol are processed through the liver. Both of them increase insulin and both increase triglyceride production as a byproduct of their metabolism. This is clearly pointed out in Robert Lustig’s paper published in the Journal of the American Dietetic Association in 2010.
The metabolic pathways are very clearly outlined below:
You can Katch my PeriScope conversation about this below or with the comments and hearts included at Katch.me/docmuscles.
Diseases seem to arrive in three’s each day in my office. Today I had three different patients with cholesterol concerns who were notably confused about what actually makes the cholesterol worse, and what causes weight gain. Each of them, like many patients that I see, were stuck in a state of confusion between low fat and low carbohydrate lifestyle change. My hope is to give my patients and anyone reading this blog a little more clarity regarding what cholesterol is, how it is influenced and how it affect our individual health.
First, the standard cholesterol profile does not give us a true picture of what is occurring at a cellular level. The standard cholesterol panel includes: total cholesterol (all the forms of cholesterol), HDL (the good stuff), LDL-C (the “bad” stuff) and triglycerides. It is important to recognize that the “-C” in these measurements stands for “a calculation” usually completed by the lab, and not an actual measurement. Total cholesterol, HDL-C and triglycerides are usually measured and LDL-C is calculated using the Friedewald equation [LDL = total cholesterol – HDL – (triglycerides/5)]. (No, there won’t be a quiz on this at the end . . . so relax.)
However, an ever increasing body evidence reveals that the concentration and size of the LDL particles correlates much more powerfully to the degree of atherosclerosis progression (arterial blockage) than the calculated LDL concentration or weight (1, 2, 3).
There are three sub-types of LDL that we each need to be aware of: Large “fluffy” LDL particles (type I), medium LDL particles (type II & III), and small dense LDL particles (type IV).
Weight & Size of VLDL, LDL & HDL
Why LDL-C is misleading: Identical LDL-C of 130 mg/dL can have a low risk (Pattern A) with a few “big fluffy LDL particles or high risk (Pattern B) with many small dense LDL particles.
Second, it is important to realize that HDL and LDL types are actually transport molecules for triglyceride – they are essentially buses for the triglycerides (the passengers). HDL can be simplistically thought of as taking triglycerides to the fat cells and LDL can be thought of as taking triglycerides from the fat cells to the muscles and other organs for use as fuel.
Third, it is the small dense LDL particles that are more easily oxidized and because of their size, are more likely to cause damage to the lining of the blood vessel leading to damage and blockage. The large boyant LDL (“big fluffy LDL particles”) contain more Vitamin E and are much less susceptible to oxidation and vascular wall damage.
Eating more fat or cholesterol DOES NOT raise small dense LDL particle number. Eating eggs, bacon and cheese does not raise your cholesterol! What increases small dense LDL particles then? It is the presence of higher levels of insulin. Insulin is increased because of carbohydrate (sugars, starches or fruits) ingestion. It is the bread or the oatmeal you eat with the bacon that is the culprit. The bread or starch stimulates and insulin response. Insulin stimulates the production of triglycerides and “calls out more small buses” to transport the increased triglyceride to the fat cells (4, 5, 6, 7).
Fourth, following a very low carbohydrate diet or ketogenic diet has been demonstrated to decreased small dense LDL particle number and correlates with a regression in vascular blockage (8, 9). So, what does this really mean to you and me? It means that the low-fat diet dogma that that has been touted from the rooftops and plastered across the cover of every magazine and health journal for the last 50 years is wrong. . . absolutely wrong.
I talk about this and answers questions on today’s Periscope. You can see the recording on Katch.me with the comments in real time here:
Superko HR, Gadesam RR. Is it LDL particle size or number that correlates with risk for cardiovascular disease? Curr Atheroscler Rep. 2008 Oct;10(5):377-85. PMID: 18706278
Rizzo M, Berneis K. Low-density lipoprotein size and cardiovascular risk assessment. QJM. 2006 Jan;99(1):1-14. PMID: 16371404
Rizzo M, Berneis K, Corrado E, Novo S. The significance of low-density-lipoproteins size in vascular diseases. Int Angiol. 2006 Mar;25(1):4-9. PMID:16520717
Howard BV, Wylie-Rosett J. Sugar and cardiovascular disease: A statement for healthcare professionals from the Committee on Nutrition of the Council on Nutrition, Physical Activity, and Metabolism of the American Heart Association. Circulation. 2002 Jul 23;106(4):523-7. PMID: 12135957
Elkeles RS. Blood glucose and coronary heart disease. European Heart Journal (2000) 21, 1735–1737 doi:10.1053/euhj.2000.2331
Stanhope KL, Bremer AA, Medici V, et al. Consumption of Fructose and High Fructose Corn Syrup Increase Postprandial Triglycerides, LDL-Cholesterol, and Apolipoprotein-B in Young Men and Women. The Journal of Clinical Endocrinology and Metabolism. 2011;96(10):E1596-E1605.
Shai I et al. Cirulation. 2010; 121:1200-1208
Krauss RM, et al. Prevalence of LDL subclass pattern B as a function of dietary carbohydrate content for each experimental diet before and after weight loss and stabilization with the diets. American Journal of Clinical Nutrition. 2006; 83:1025-1031
Gentile M, Panico S, et al., Clinica Chimica Acta, 2013, Association between small dense LDL and early atherosclerosis in a sample of menopausal women, Department of Clinical Medicine and Surgery, University “Federico II” Medical School, Naples, Italy Division of Cardiology, Moscati Hospital, Aversa, Italy A. Cardarelli Hospital, Naples, Italy
In light of the fact that exercise DOES NOT cause weight loss, exercise has a fascinating ability to enhance ketosis. No, seriously, I don’t care what your trainer told you, you won’t loose weight with exercise, no mater how hard you try. However, exercise does help you body attain a ketogenic state.
When you exercise, the muscles take up glucose and oxygen to burn as their primary fuel. Exercise has actually been shown to enhance this process and reduce the “insulin resistance” effect that the the SAD diet (Standard American Diet) has on 2/3rds of the population (whether they realize it or not). Mild to moderate exercise like a walk or even a mild jog, and resistance training like weight lifting, yoga or Pilates increased the drive of the glucose into the cells and improves the ability of the cells to use the glucose.
In a person following a carbohydrate restricted diet (Ketogenic, Low-Carb, and even Paleolithic to some degree), the body maintains a stable level of blood sugar by releasing glycogen from the liver and gluconeogenisis as needed to support the 100 grams necessary per day required by the brain (the liver makes about 240 grams per day no mater what you do). In the absence of extra glucose as fuel, the body will then use triglyceride and/or ketones as fuel. Exercise improves the sensitivity to the small amount of glucose and actually ramps up the presence of ketones placing the person into a more ketogenic state.
This enhanced ketogensis is often experienced as “second wind” or “being in the zone” or even as an ability to “hyperfocus” during exercise. But the exercise levels must be in the mild to moderate range for this to be accomplished.
But, there’s a fine balance, if the muscles are pushed too hard to fast, lactic acid builds up because of a shift to an anaerobic state and the acid creates a stress response, triggering cortisol and increased glucose formulation, causing one to shift out of ketosis.
How do you know if you exercising too hard? You should be exercising hard enough to break a sweat, but not so hard that you can’t carry on a conversation with your partner at the same time. Over time, as the body becomes more effective at using ketones, you’ll find your exercise intensity can and will improve.
See Dr. Nally try to explain all this while riding his horse Bailey in the White Tank Mountains:
Or you can Katch it here: https://katch.me/docmuscles/v/ce43292a-296f-3de4-bf6f-d19cd688fc62
I have been using PeriScope as a fun method of staying in touch with each of you, my fantastic patients, and people all over the world. If you’re interested in seeing me live, you can down-load the PeriScope app onto your iPhone, iPad or Android phone through the App Store.
You can see this mornings PeriScope (with the rolling comments and hearts on the screen) with Dr Nally here on Katch.me/docmuscles. Katch is a great site that holds a record of all my recent PeriScopes.
Or you can watch the video stream (without comment stream) below:
If you have a question you’d like me to address on PeriScope, please let me know.
This week I had the pleasure of seeing a really nice 46 year old Hispanic male who is fairly new to the office. He came back in to see me in follow up on his diabetes. To give you a bit of background history, the patient came to see me about 6 months ago, just not feeling very well. Based on his symptoms of fatigue, history of elevated blood sugar and family history, lab work was completed.He saw us initially with a Hemoglobin A1c of 12.3% in June (normal should be 4.9%-5.6%). This means he had an average blood sugar over the previous three months of about 310 mg/dL (normal should be < 110 mg/dL).
Past Medical History include: Diabetes Mellitus – type II (not on any medications when initially seen), Hypertension (high blood pressure), Dyslipidemia (elevated cholesterol) and a non-specific heart arrhythmia.
Medications: None
Surgeries: Knee & shoulder arthroscopies
Family History: Father Diabetes, Stroke, Heart Disease, Hypertension, Elevated Cholesterol
After getting his labs back, we had a very long conversation about the need to either fix his diet dramatically, or he may be looking at using 3-4 oral medications or even insulin to control his blood sugar.
When I see average blood sugars (HbA1c) stay over 6.5% (or greater than 140 mg/dL), the risk for retinal, kidney and nerve damage is significant and often irreversible after 4-5 years. Most physican’s are affraid to lower the HbA1c to less than 7.0% with medications due to low blood sugar events, and so the diabetes community has “settled” with 7.0% as being effective. However, it still isn’t low enough. I saw this happen with my father and with other members of me family. I’ve seen it happen over and over with my patients over the last 15 years when they have not lowered their blood sugar and reduced the high insulin loads that occur in response to those high blood sugar levels. It has been my experience that HbA1c can be very safely lowered to the normal range, as low as 5.2-5.6% without symptomatic low blood sugars, with the correct diet and careful use of medications.
As you can see, a dramatic change in his blood sugar has occurred in a three month interval. Not only that, we see a significant change in his cholesterol profile.
Previously, we looked at LDL-C for heart disease risk, however, I have multiple patients that have had heart disease with normal LDL-C ( <100 mg/dL). LDL-C is just a summation of all the particles. The LDL particle is actually made up of three sub-types and it is specifically the small dense particle that causes the vascular risk. You can see a dramatic normalization of the small dense particle LDL with no change in LDL-C and minimal change in Total Cholesterol in the patient’s labs when he reduces his carbohydrate intake. This is a pattern I see every single day. When serial carotid ultrasound studies are completed, I see reduction in blockage and reduction in the vascular wall thickening. I will be very interested to see the vascular studies on this patient and I will await his results as he tightens up his diet even further.
All in all, he has dramatically brought his diabetes under control with carbohydrate restriction and if he continues this lifestyle, he has reduced his risk for retinal damage, reduced his risk for kidney damage, reduced his risk for nerve damage and essentially added 20 years to his life.
(Disclosures: Dr. Nally has no vested interest, monitary or otherwise, in Novo Nordisc or it’s products including liraglutide.)
Dr. Nally chats via PeriScope with the four corners of the US . . . Did we see you there?
Join me for Q&A about general #low-carb #ketosis and #ketogenic questions (protein amounts, Vitamin D, fatty liver disease, ketosis and sleep, osteoporosis/osteopenia, and much more) on a Friday evening between charts.
There are three constants in life: change, choice & principles. Change, ironically acting as a constant, is the variable that we have limited control over. Accepting that change is going to happen, that change is constant, and making choices to prepare for those changes is the key to success. My last post introduced the 10 Principles of the Ketogenic Lifestyle. This post will discuss choice as a foundation for those principles outlined in the ketogenic lifestyle. Choices are directly influenced by the balance between the mind, the body and the spirit of man.
LIFESTYLE PRINCIPLE 1 – WHEREVER YOU GO, THERE YOU ARE
People seem to get sidetracked off a ketogenic lifestyle for a number of reasons, but the most common I hear is that they were traveling, had company visit or they were on vacation. Successfully living a lifestyle requires that you first know who you are and where you are before you can consistently make good, solid, principle based choices. So I ask, who are you? Are you defined by your job, by your finances, by your travels, by your friends or by your vacations? Each of these experiences is unique. Our experiences place both good and bad before us. I have come to learn over time and countless interactions with people that nothing is coincidental. Everything, good and bad, happen for a reason.
Today’s society teaches the Pleasure Principle. This is the human instinct to seek pleasure and avoid pain, including avoiding painful recollections. We often define ourselves by those things that bring us pleasure. We each go through personal tests, failures and triumphs. Some of us harness all of those experiences for good, others find worsening mental paralysis due to fear of them. We often hide from the painful experiences and attempt to bury or forget them. Food is often involved with many of the experiences of life, and for a significant number of people, the endorphin release from eating a meal, sometimes just the act of chewing, may be the only pleasure one experience in a day, in a week or a in a year. Many people hide from painful recollections behind the simple pleasure produced by the eating of “comfort foods.” Food, and our opportunities to experience pleasure from it’s various flavors, textures and physical stimulus, begin to define us. However, hiding from life’s painful memories with momentary pleasures usually prolongs or makes the problem worse. The ingestion of simple foods containing glucose and fructose, their effect on the liver, and the hedonistic hormonal response is the basis of addiction, and simple carbohydrates provide the perfect fix.
Fascinatingly, when fructose is metabolized in the liver, in the presence of glucose (the basic structure of sugar – one fructose molecule bound to a glucose molecule), the byproduct has a hedonic (pleasure experiencing) effect on the exact same pleasure receptors in the brain that bind to morphine. Yes, that’s why the M&M’s make you forget your troubles and why the Jolly Rancher is so jolly. And, its the same reason you crave another do-nut two hours after you ate the entire baker’s dozen.
Although obesity has been recognized as a disease, our use of foods to celebrate with people or events in life is still a form of pleasure seeking. Excuses to deviate from healthy behavior under the guise of family, vacation, or social requirements, acknowledges our willingness to hide from pain with hedonic drugs like chocolate chip cookies and cotton candy. In fact, it’s usually a welcomed and and expected acceptable excuse.
“Dr. Nally, I can cheat eat and bad, (meals loaded with starch) because I’m on vacation” . . . from my problems. It’s so acceptable, we’ve based movie themes around it.
Healing can only occur when one is willing to confront and talk about the reasons, the real reasons you’d rather experience the endorphins from the do-nuts with your family instead of acknowledge your weakness, stresses, and fears. Many of us are so afraid of where we might be, we avoid acknowledging where and who we are. It takes courage not to take the easy path. And I will be the first to admit, pizza is the easy path and it’s scenic views are decorated with french fry palms and sunset clouds of apple fritters.
“There appears to be a conscience in mankind which severely punishes the man who does not somehow and at some time, at whatever cost to his pride, cease to defend and assert himself, and instead confess himself fallible and human. Until he can do this, an impenetrable wall shuts him out from the living experience of feeling himself a man among men. Here we find a key to the great significance of true, un-stereotyped confession – a significance known in all the initiation and mystery cults of the ancient world, as is shown by a saying from the Greek mysteries: “Give up what thou hast, and thou will receive.” (Carl Jung)
We have a choice about what to eat and when to eat, however, each choice has a reward and/or a consequence.
Points of Focus: Where are you and what are you hiding from? Sharing your weaknesses actually empowers you you overcome them. This can often be accomplished through the simple act of journaling, planing your meals the day before and journaling your successes and failures in that plan the following day. Allowing yourself and others insight into your times of weakness actually brings strength. It allows one to look at the reasons for food choices base on how you feel, and how you felt after the choice. If forces one to think about a choice before it ever has to be made. In my 15 years of medical practice, I have yet to hear a child find fault with a parent who worked tirelessly to make ends meet, admittedly struggled with alcoholism, battled against disease or fought against belittling for a belief. The child has always expressed their admiration of their parent’s courage and understanding of why decisions were made, even when erroneous. It takes courage to admit that wherever you go – there you are.
LIFESTYLE PRINCIPLE 2 – KEEP IT REAL
I no longer believe in coincidence. Whether you have thought about it or not, every interaction you have with others (even our interaction . . . your reading this blog), are not by coincidence. There is a reason. Whether you believe it or not, everything around us testifies that God exists; the Hand of Providence can be seen from the rotation of the earth, planets and stars, the precision of the seasons, the balance of the atmosphere allowing for the perfect pressures and concentration of elements to sustain a life giving breath, to the perfect replication of DNA within billions of cells throughout the body. I’m not trying to get religious, and, no, I can’t prove this through the scientific method . . . But, if the Big Bang started the universe, what started the Big Bang? Where did the first atom or molecule or particle of dust come from? I have a very difficult time accepting that you and I are here by accident, by a chaotic explosion that created order. That implies that there must be a plan, and that plan had to have been set in motion by a Creator. That also implies that that Creator placed solutions to our challenges, including the diseases of civilization, within our grasp and available to those seeking the solutions upon the earth today.
I have seen enough in my medical career to know that simple coincidence has frequently become significantly important, life changing and often life saving. This does not happen by accident and screams loud and clear that there is a plan for you and me. No good father would lock his child in a room without doors or windows or any escape without everything in the room, both good and bad, pointing to the reason the child was in the room, and pointing the way for the child to become his or her best self, physically and emotionally. Life has meaning. It is supposed to. If we get off track, coincidence and interactions lead us back.
“Behold, the hour cometh, yea, is now come, that ye shall be scattered, every man to his own, and shall leave me alone: and yet I am not alone because the Father is with me.” (John 16:32)
The Bible, among other records, records the voices of men and women from years past transcribing their experiences with the Hand of Providence, how that spiritual void was filled, how it helped the with choice and how our lives have deeper meaning and consequence, even amidst significant adversity.
Take a week and look at the synchronicity of your life. Journal about it. Don’t dismiss a second invitation from someone to discuss an opportunity or meet someone your friend thinks could be important to you, open that book that someone left behind on the subway seat beside you. Don’t assume it is meaningless, that some kind person returned your sunglasses or your wallet. Look at the simple interactions and recent relationships. These are the breadcrumbs and the street signs from a loving Creator, a loving Father.
Keeping it real means nothing less than complete authenticity. The last place you want to be is in the first-class seat on the plane to no-where. Have the faith to get off the plane and take the bus, ride your bike, or even swim upstream in the direction you’re supposed to be going. Look for the coincidences, bread crumbs and spiritual street signs in your life.
How does this relate to a ketogenic lifestyle? Every religion or spiritual tradition speaks of a polestar. The polestar is that anchor to which the entire solar system is tied by invisible aerial chords and the engine that powers the universe. Those cords are connected with our own individual polestars. A ketogenic lifestyle is one that encompasses mind, body and spirit. It is a lifestyle that demands that you link and align your personal polestar with the truth inside and around you. It takes both courage and faith, but it brings immeasurable strength and help in achieving your goals. A person out of balance with life is under stress. Chronic stress produces excessive cortisol and other powerful adrenal hormones that displace the body’s and the mind’s endocrinologic balance, leading to weight gain, weight retention, and chronic disease. This often has significant effect externally on the body in processes seen like depression, anxiety, fibromyalgia, and allowing for amplification of inflammation and auto-immune dysfunction. We refer to this inter-relationship in the medical community as psychosomatic and/or viscerosomatic dysfunction, the psyche (the mind) and/or the viscera (internal endocrine organs) directly and adversely influence the function of the soma (the structural body separate from the mind).
“He who does not know himself, does not know anything, but he who knows himself, knows the depth of all things.
” . . . If you bring forth what is within you, what you bring forth will save you. If you do not bring forth what is within you, what you do not bring forth will destroy you.” (Book of Thomas the Contender)
Point of Focus: Your life is never without meaning. Keep it real by recognizing that diet alone may not compete your answer for physical health. Having courage and faith allow you to see and embrace the truth that is right in front of you. The Alcoholics Anonymous’ 12 step program only becomes successful when one realistically and courageously applies their faith to align with the truth they have felt all along. For any long-term lifestyle change to take place, one must connect and live the principles before one truly knows they are true. In this way the Ketogenic Lifestyle becomes real.
KetoOS – Drinkable Exogenous Ketones
LIFESTYLE PRINCIPLE 3 – TO cheat, or NOT to cheat, that is the question
I have been asked this question by every patient I have placed on a ketogenic diet at least once and often three or four times throughout the course of our treatment plan. I usually answer this question with a question. “Why do you want to cheat?”
The desire to cheat usually arises form one of three reasons:
You’re not eating enough fat to satiate your appetite and you are truly hungry. The body recognizes that it can use and absorb glucose much faster than fat, as fuel, so it naturally will crave “sweets.” In this case, the case of true hunger, solution is to increase your fat intake. You should be eating at least 50% of your total calories in the form of fat.
Insulin loads are still high, stimulating rebound hunger and hedonistic cravings. You’re either eating too many carbohydrates with your diet or you’re using a sweetener that stimulates insulin without raising blood sugar (See my article The Skinny about Sweeteners).
Cheating with a specific food fulfills a psychological need, feeds an addiction or represents an obligation to fulfill a societal ritual. Journaling helps to identify and break this cycle.
If you are truly in ketosis the cravings to cheat don’t exist, they actually disappear. Other societal rituals, like birthdays, anniversaries, weddings, spiritual ceremonies or rites of passage are often tied to or use food as symbolism. In these cases, the decision to cheat is really yours.
When a person cheats, it can take as many as 3-5 days to get back into ketosis, and for some 2-3 weeks. Carbohydrate cravings will rebound and often be present for up to 72 hours after cheating. You have to decide if cheating is worth 3 days of carbohydrate cravings and 3-7 days of stifled weight loss.
Point of Focus: There are no Ketosis Police! Really. They don’t exist! Dr. Nally will not show up in uniform on your doorstep with a set of handcuffs and a bag of pork rinds. You won’t be arrested for eating bread and those of us who have been following a strict ketogenic lifestyle for years really don don’t mind at all if you decide to cheat. We will smile and we may even ask you how it tastes or if you liked the flavor, but don’t be self-conscious, because when one is in ketosis for a few months, we really don’t crave cheating any longer, and we won’t judge you. And, don’t feel obligated to justify why your cheating, this is a lifestyle. You probably won’t ask me why I chose to wear long sleeves on a hot day in Arizona, for the same reason I won’t ask you why you decided to wear a Speedo.
LIFESTYLE PRINCIPLE 4 – Hunger Management
Life comes at you pretty fast and if you’re not prepared, hunger can bite you. Most people fall off the wagon when they are unprepared for missing a meal on a stressful day. I’ve recently heard the argument that “there is no wagon, so don’t worry about falling off.” This is false security that leaves one unprepared for life events. Pioneers traveled in wagons for two reasons. First, the wagon held supplies essential for survival. Second, wagons usually traveled in wagon trains. This means that there was more than one person on the wagon and there was more than one wagon on the trail with you. Traveling with a wagon train meant you had others on the same trail with the same tools for safety and support.
In the world of fast foot, fast photos and speedy delivery, we often don’t adequately prepare for hunger or cravings. There are some essential hunger management tools for the Ketogenic Lifestyle:
Eat meals containing >50% fat. This, in and of itself, delays hunger and ensures the satiety center of the brain is happy for longer periods of time.
Carry rescue foods with you or keep them at your office or in your fridge at home. These include low-carb nuts like almonds, walnuts, macadamia nuts; Keep hard and string cheese handy for a snack. Use sliced deli-meats with the cheese as a snack when the cravings kick in. Pork Rinds, beef jerky, olives, are great natural food options.
If you have time and can cook, develop your favorite “Fat Bombs“ and have a bag full in the fridge for those cravings.
Having the moral support of a buddy, spouse, friend or work companion who checks on your progress daily, assists with meals and meal choices is priceless. Periscope, a free Twitter based App, has become a means of checking in with your Ketogenic Support group around the world that connects to those you follow on Twitter. You can follow me, @docmuscles, and a number of fascinating health Periscopes that focus on ketogenic, low-carb, whole food paleo approaches: @livinlowcarbman, @_danielleeaton, @kasandrinos, @fatissmartfuel, @domskitchen, @mikemutzel, @keribrewster, @tombilyeu, @glutenfreenj, @paleocomfort.
Being accountable to yourself in a diet journal daily and to your doctor regularly every 1-2 months also helps keep motivation going forward. Jimmy Moore, author and podcaster at the Livin’ La Vida Low-Carb Show has also posted one of the most extensive lists of physicians specializing in ketogenic diets from around the world. You can find that list here.
LIFESTYLE PRINCIPLE 5 – Stress Reduction
Pages and pages can be written about stress reduction. In fact, I’ve written about the chemical responses that stress has on weight gain in my post, Stress. . . The Weight Loss Killer. But there are a few daily essentials that should be added into the Ketogenic Lifestyle to manage stress.
First, are you getting adequate sleep? Remove the television, computer, cell phone, iPad or other electronic distraction from the bedroom. Go to bed at the same time and get up at the same time each day. Give yourself time each day away from being plugged in, logged in or on-line.
Second, over exercising or being malnourished can cause chronic stress. I have a number of patient that have been convinced that they have to work out 60 minutes a day 6-7 days per week. It is essential that you realize muscles need a minimum of 48-72 hours to recover from specific types of exercise. If you run for 60 minutes. It will take your muscles 48 hours to recover from the running. If you do upper body weight lifting, it will take 48-72 hours for those muscles to recover from that weight lifting. Exercising the same muscle group with the same exercise over stresses the muscles and leads to significant chronic stress, spiking the cortisol levels and halting weight loss and raising cholesterol & triglycerides. Under eating or fasting to starvation has the same effect.
Third, mild intensity (40% of your maximal exertion level) exercise 2-3 days a week was found in a recent study to lower cortisol and decrease over-all stress, raising serotonin and dopamine in the brain; however, moderate intensity (60% of your maximal exertion level) to high intensity (80% of your maximal exertion level) exercise was found to raise it. A simple 20 minute walk, 2-3 times per week is very effective at stress reduction, reduction in cortisol and improvement in ketosis.
Point of Focus: The goal is cortisol reduction. This can be done through regular and restful sleep and mild exercise. Chronic elevation in cortisol directly stimulates an increase in insulin by increasing the production of glucose in the body, and cortisol blockaids the thyroid axis. Both of these actions halt the ability to loose weight, amplifies the production of inflammatory hormones and drives weight gain. Cortisol also increases appetite. That’s why many people get significant food cravings when they are under stress (“stress eaters”). Cortisol also indirectly affects the other neuro-hormones of the brain including CRH (corticotrophin releasing hormone), leptin, and neuropeptide Y (NPY). High levels of NPY and CRH and reduced levels of leptin have also been shown to stimulate appetite.
Hopefully, this gives you some starting points and direction to your Ketogenic Lifestyle. If I’ve missed something that you’ve found to be essential, let me know. Its always great to hear what has helped you in your Ketogenic journey. Until next time, pass the butter!!!
I’ve had a number of emails and requests from patient’s to locate a source for fat percentages and protein contents of various foods as they prepare and follow a ketogenic lifestyle. I’ve looked all over, however, nothing easy and concise has made itself readily available, and there hasn’t been a simple one page tool at your fingertips . . .
Hopefully, this list will start to fill that gap. Use the list to calculate protein and fat levels as needed. Let me know if I can add to the list or if there are foods you commonly use that I’ve missed. Keep the ketones up and your waistline down!
Nutritional Values of Common Ketogenic Foods:
Food: Protein Contents: Fat Contents:
Steak (Ribeye) – 65 grams per 8 oz. 49%
Steak (Top or Bottom Round) – 23 grams per 3 oz. 33%
Ground Beef (75% Lean) – 22 grams per 3 oz. 55%
Pork Chop (boneless) – 26 grams per 3 oz. 15%
Ham – 17 grams per 3.5 oz. 12%
Bacon (grilled) – 22 grams per 3.5 oz. 75%
Sausage (beef) – 14 grams per 3.5 oz. 79%
Sausage (pork) – 17 grams per 3.5 oz. 75%
Chicken Breast (boneless, skinless) – 24 grams per 3 oz. 18%
Turkey Breast – 24 grams per 3 oz. 15%
Yellowfin Tuna – 25 grams per 3 oz. 10%
Light Tuna – 22 grams per 3 oz. 8%
Halibut – 23 grams per 3 oz. 19%
Sockeye Salmon – 23 grams per 3 oz. 22%
Tilapia – 21 grams per 3 oz. 13%
Deli Meats:
Roast Beef – 18 grams per 3 oz. 16%
Canadian bacon – 15 grams per 3 oz. 33%
Pepperoni – 18 grams per 3 oz. 83%
Roast Turkey Breast – 18 grams per 3 oz. 15%
Snacks:
Beef Jerky (Jack Links) – 13 grams per 1 oz. 9%
Peanut Butter (Peter Pan Crunchy) – 8 grams per 2 tbsp. 76%
Mixed Nuts – 6 grams per 2 oz. 79%
Almonds, raw – 6 grams per 1 oz. 66%
Walnuts, raw – 4 grams per 1 oz. 85%
Sunflower seeds, raw – 6 grams per 1 oz. 76%
Tofu – 12 grams per 3 oz. 30%
Greek Yogurt – 23 grams per 8 oz. 0%
Cheeses:
Swiss Cheese – 24 grams per 3 oz. 66%
Cream Cheese – 11 grams per 3.5 oz. 79%
Ricotta cheese – 10 grams per 3.5 oz. 63%
Cheddar cheese – 24.6 grams per 3.5 oz. 74%
Eggs – 6 grams per 1 large egg 60%
(Adapted from http://www.caloriecount.com)
A printable PDF copy of this information is available here:
To live in the presence of great truths and eternal laws, to be led by permanent ideals – that is what keeps a man patient when the world ignores him, and calm and unspoiled when the world praises him. Hopefully, these posts are adding to your stable ideals.
How much protein should you be using? Watch the periscope below . . . and good morning from Surprise, Arizona!!
I’ve included the calculations you will need to get a ballpark estimate on your protein intake from your ideal body weight
Ideal Body Weight (IBW):
These calculations are estimated ideal body weight in kilograms (kg). You can convert your weight in pounds (lbs) to kilograms (kg) with the following formula:
The average male needs 1.2 mg/kg protein per day. The average female needs 1.0 mg/kg protein per day.
Males:
IBW = 50 kg + 2.3 kg for each inch over 5 feet.
Females:
IBW = 45.5 kg + 2.3 kg for each inch over 5 feet.
Examples: If I am 6 feet tall, as a male, then I add 50 kg to 27.6 kg ( 6′ tall is 12 inches over 5′ x 2.3 kg) = 77.6 mg of protein requirement per day. That means that if I (a 6′ tall male) ate three times a day, then my protein requirements are 25.9 mg per meal.
The most exaggerated “frowney” face I get in the office seems to occur when patient’s find out that they cannot eat oatmeal or cereal any longer when following a low-carbohydrate dietary lifestyle. No, oatmeal is NOT good for you . . . I don’t care what WebMD recently said. No, steel-cut oats are even worse (1/4th cup of steel-cut oats is 27 grams of carbohydrate – Who only eats 1/4th cup of oatmeal? Most people eat at least 1/2 -1 cup at a sitting. You do the math . . .)
When I mentioned this to a disabled patient, even her service dog frowned.
Now, before you go running to Larry, the Quaker Oats Mascot (he’s been around for over 140 years), and ask his weight loss advise, I have the solution.
Larry, the Quaker Oats mascot loses 10 lbs for new 2012 cover (He finally figures it out after 137 years)
My angelic wife, Tiffini, the amazing homestead chef and animal husbandry specialist on our little farm, started making low-carb granola for our horseback trail rides. Prior to our discovery of a ketogenic lifestyle, granola was a staple in our pantry, on road trips and in the saddle bags on the trail. This has now replaced any craving either of us had for granola. It carries nicely all day in a Ziplock bag on horseback. It even tastes fantastic in a bowl with unsweetened almond milk as a breakfast alternative if you’re tired of eggs and bacon (but, who ever tires of eggs and bacon? I know . . . Right?!!)
I’ve been nibbling from this actual cookie-sheet of low-carb granola while writing this post. . . I wish you were here to share it with. Soooooo very good, and good for your ketogenic lifestyle. I think I’m going to eat another handful while I finish up Part II of the Principle Based Ketogenic Lifestyle post. Enjoy . . .
In a food processor, process the almonds and 1 cup of the pecans until it resembles coarse crumbs. Using a knife (preferably a sharp one – remember all bleeding stops eventually), chop the remaining 1/4 pecans coarsely.
Melt the butter and place it in mixing bowel or mixer (We use a Kitchen Aid Mixer). Pour the coarsely chopped nuts into the mixing bowl. Stir in flax seed meal, sunflower seeds, coconut flakes, pepitas and vanilla whey protein powder. Blend in the remaining wet mixture, egg whites and add a pinch of salt. Mix until it forms “clumps.”
Spread the mixture evenly on a large wax paper covered baking or cookie sheet and bake at 350 degrees F for 20-25 minutes or until golden brown. Let it cool on the baking sheet to crisp up for a few hours.
It can be stored in a Ziplock bag in the refrigerator.
It has been resoundingly clear to me over the last couple of weeks that there is a tremendous need for a principle based approach to a ketogenic diet. This approach, however, must be simple. So many of the approaches to weight loss I read about are complex and the questions that arise from these approaches are innumerable. Losing weight should not be as difficult as putting a man on the moon. To quote a patient recently, “If it ain’t simple, Doc, I ain’t doing it. . .”
I agree.
Any approach that requires the conversion of food to numbers or calories or exchanges becomes cumbersome, and I personally won’t follow it for more than a week. The principle based approach should be simple and is really based upon the mantra:
Give a man a fish and he will eat today. Teach a man to fish and he will eat for the rest of his life.
Ketogenic diets are wrongly referred to as diets. What I’m talking about is a ketogenic lifestyle. Simple lifestyle design should not be hard. So, what do you say? Shall we learn to fish?!
I assume that if you’re reading this article, you already understand that weight gain is not due to an over intake of calories. Weight gain is due to hormone signals throughout the body leading to the storage of fat . . . specifically, triglycerides being taken up into the fat cells. The hormone that independently controls uptake of fat into each fat cell is insulin. Insulin is an essential hormone, but too much of it stimulates the adipose (fat cells) to over-stock triglycerides or essentially “get fat.” It, actually, is that simple. There’s really only one rule to this lifestyle: If it raises your insulin it will halt or stall your weight loss. Write that on your hand or your forehead or in your planner, the lifestyle revolves around that one rule.
Most people start a ketogenic diet because they want to lose weight and have failed at multiple other dietary approaches. Reasons for weight control failure are often multi-faceted, but they all start with from a position of flawed understanding. The majority of approaches to weight management come from the false assumption that weight is gained because of an over-consumption of calories or a lack of physical activity to burn excess calories. People have faithfully been restricting calories and exercising to exhaustion since the early 1980’s to no avail. (Well, 1% of people succeed, but the rest of us failed this approach). The definition of insanity is repetitive completion of an ineffective action and expecting a different outcome each subsequent time around. If you still think that caloric restriction and exercise is successful, I’ll be shipping your drawstring white vest and your invitation to a padded cell shortly.
Let me put it clearly. We’ve been exercising and cutting our calories since 1975 and look at what it’s gotten us . . .
. . . . a country that is now recognized as the “United States of Corpulence.” Super-Size me has become literal. “Houston . . . we have a problem . . . !”
The rule above is based on foundational principles. Understanding of the principles allows one to successfully apply the rule above.
PRINCIPLE 1
The first principle in a ketogenic lifestyle is understanding that the problem is not caloric, but hormonal. Choices and actions from here on out must be based on this understanding. Anything that will raise insulin will thwart ketosis. Insulin stimulates lipoprotein lipase, the enzyme that pulls the triglycerides into the fat cells. Without insulin, we don’t gain weight. (That’s why type I diabetes are usually very slender and skinny).
The standard lab value for normal fasting insulin levels reflect 10-22 uIU/L as the normal. However, in my office, glucose tolerance tests and postprandial glucose tests consistent with impaired fasting glucose are routinely positive when the fasting insulin level is >5 uIU/L.
Point of Focus: If your having trouble, look at the hormones. Food stimulates hormone responses. Focus on the hormone response to your diet.
PRINCIPLE 2
A ketogenic diet is one where the body uses fatty acids as the primary fuel. Those triglycerides mentioned above are made up of three fatty acids linked to a glycerol molecule. To use the triglycerides, the three fatty acids must be broken away from the glycerol by hormone sensitive lipase (HSL). Insulin directly inhibits HSL. Keeping insulin levels low is the first step in shifting to a ketogenic metabolism. Lowering insulin allows access to the fatty acids in your fat cells. Triglycerides are not water soluble and the rate by which they can be taken up and burned in the mitochondria limits the speed by which triglycerides can be used as fuel. The by product of triglyceride burning is ketones. Ketones themselves can be used as fuel and over 4-6 weeks, the body can enhance its ability to use ketones when fat is the primary fuel. This is called “Keto-Adaptation.”
Point of Focus: Too much carbohydrate in the diet shifts the body from it’s use of fat and triglycerides back to glucose. In general, to become “keto-adapted,” limit carbohydrate to < 20 grams per day. Keep protein at around 0.8 to 1 gram of protein per pound of body weight.
KetoOS – Drinkable Exogenous Ketones
PRINCIPLE 3
Wait a minute!? Where do the ketones come in? When fatty acids are burned or oxidized in the mitochondria of cells within the liver, they are converted into Acetyl-CoA. The Acetyl-CoA is used to form ATP for energy in the Citric Acid Cycle.
IF excess Acetyl-CoA production occurs or if inadequate oxaloacetate is present, the extra Acetyl-CoA is transformed into ketone bodies – specifically beta-hydroxybutyric acid and acetoacetic acid. Fat can be oxidized or burned for fuel while ketones are being produced. Ketones are much smaller molecules and can more easily be transported in the blood than triglycerides, as they are water soluble. The ketones themselves can also be used or burned as fuel as the body upregulates the mitochondria’s ability to use the ketones as fuel as well. As I mentioned above, this process of “keto-adaptation” can take 4-6 weeks. Keto-adaptation results in humans having a greater desire to be physically active – the miraculous conversion of the couch-potato into the bacon-burning triathlete.
Point of Focus: Sugar is a drug. Its byproduct has the same hedonic effect on the brain as morphine. Sugar withdrawal can commonly cause headache, anxiousness, insomnia, dizziness, fatigue and moodiness within the first week of carbohydrate restriction on the road to keto-adaptation.
PRINCIPILE 4
For the average person to become “ketotic” or reach a state of ketosis, it takes lowering the carbohydrates to less than 20 grams per day (and sometimes less than 10 grams per day) for at least 3-7 days. Yes, it can actually take a week to reach ketosis. I have a few patient’s that are so insulin resistant that it takes longer. This means that to reach that fat burning state, one must maintain a low insulin response by restricting starch or carbohydrate intake to less than 20 grams per day for a minimum of a week. For your body to efficiently use the fuel it can take up to 6 weeks. This is why many people state that they “don’t feel good” or “can’t maintain their exercise levels” when starting a ketogenic diet. For most people, once they reach the 6 week mark, mitochondria have been unregulated and “fine tuned” to burn ketones, fat burning becomes efficient and energy levels begin to increase. In fact, for many like myself, you’ll finally feel like exercising for the first time in you life.
Point of Focus: If you’re already exercising, don’t be surprised if you feel more sluggish for the first four weeks. If you’re not exercising, I don’t recommend starting until after you pass through the Keto-Adaptive phase.
PRINCIPLE 5
Clinically, the average patient in my office will lose 5-15 lbs each month for the first three months. Then the weight loss will slow to 2-5 lbs per month. However, 1/2-1 inch continues to disappear off the waist circumference measurement every month. THIS IS NORMAL. Continued weight loss of 15 lbs a month will leave you looking like the Michelin Tire Man – rolls of skin without fat. The body slows the weight loss to keep up with skin and connective tissue remodeling. As long as ketosis is maintained, the fat will continue to melt away. At this point, I’m not so worried about scale weight as I am your waist circumference.
Point of Focus: Successful ketosis does not always affect the scale, but usually causes your pants to fall down.
PRINCIPLE 6
It has been my experience that it takes about 18 months for the average patient to reverse the insulin resistance while following a carbohydrate-restricted, high-fat ketogenic lifestyle. There is no quick fix for this. If there was, I’d be sitting on a beautiful beach in the Caribbean.
Point of Focus: The Ketogenic dietary lifestyle is actually the antidote to insulin resistance, diabetes and the diseases of civilization.
PRINCIPLE 7
Improvement in insulin resistance has also been demonstrated with mild to moderate intensity resistance exercise. Moderate intensity resistance exercise is 20-30 minutes of exercise like walking, easy jogging, cycling, lifting weights, yoga or Pilates with speeds or weight heavy enough to break a sweat, but not so fast or heavy that you cannot carry on a conversation with your exercise partner. Exercise improvesinsulin resistance – BUT IT DOESN’T CAUSE WEIGHT LOSS! Yes, I know, Jack LaLanne just rolled over in his grave. But, let me say that again. Exercise improves insulin resistance, but it does not improve weight loss!! The three largest and most intensive studies of exercise involving over 67,000 people demonstrate that you can exercise till the cows come home and you’ll average about 1% weight loss. If you exercise, realize it WILL make you hungry. Eating the wrong food (carbohydrate containing foods) will stimulate insulin release causing your exercise to be fruitless (Actually, your diet should be “fruit-less” anyway)
Point of Focus: Exercise because you feel like it, it improves insulin sensitivity and it decreases stress, not for weight loss.
PRINCIPLE 8
If you are eating enough fat, you won’t be hungry. Although this doesn’t always hold true in the case of patient’s with lepin resistance. 40-60% of patients with insulin resistance have a concomitant leptin resistance (see the article on lepin resistance here). A ketogenic diet is one in which 50% or more of total calories come from fat. No, you don’t have to count calories, just pick foods that contain 45% fat or more. Look for grass fed products as they will be higher in Omega 3 fatty acids. Red meat is 55% fat. Pork is 45% fat. This is where the chicken salad or turkey wrap fails (see Why Does Your Chicken Salad Stop Weight Loss). Look for alternatives to replace your basic meals and snacks. If you love chips, try pork rinds or make chips from fried cheese or pepperoni. Guacamole is a great replacement for bean dip.
Point of Focus: There is no need to eat 3-6 times per day. As you increase the fat in your diet you will feel more full. Eat when you are hungry, whether that is 3 times a day or once day, listen to your body.
PRINCIPLE 9
I’ve been following a ketogenic diet for over 10 years. The most common complaint I hear is, “Dr. Nally, I’m tired of eating eggs.” Ketogenic diets don’t have to be boring. There are hundreds of resources on the web for spicing up your ketogenic diet. See the Recommended Sites page above for some ideas to start. The Ketogenic Cookbook by Jimmy Moore and Maria Emmerich is a recent edition to the literature and a fantastic resource. Check out Franziska Spritzler’s Low Carb Dietitian website and new book as well. If you live in the UK, you should see Emily Maguire’s website and blog. She just completed a world tour, sampling all the low carbohydrate foods and restaurants around the world. If you are a picture person, check out the Best Keto Meals of 2015 Pinterest page followed by almost 16,000 people. If you haven’t takent the time, you should visit Dr. Andreas Eenfeldt’s website. He is one of Sweden’s premier ketogenic doctors has an immense number of resources at his website, Diet Doctor. Finding someone that can help you fine tune your diet is also essential. You can find a list of doctors that use ketogenic diets here.
Point of Focus: This lifestyle will require you to use real, whole food and cook like your grandmother or great grandmother did in the past. Unfortunately, we’ve lost a great deal of the art of cooking that needs to be re-discovered. If your lifestyle is too busy to cook and prepare real food, that busyness is probably causing you stress, another culprit in the weight gain cycle. The truth will set you free, but it will probably make you miserable first.
PRINCIPLE 10
WARNING! A very sweet patient of mine was given these instructions to treat her weight and blood sugar abnormalities. She applied these principles and they worked marvelously. She called me a few weeks later, however, mad as a wet hen. She placed her husband (not my patient at the time) on the same dietary changes. Her husband, who had significant blood pressure problems and was on four different blood pressure medications I later found out, had a sudden drop in his blood pressure and passed out. As happens to many of my patients, blood pressure, ejection fraction of the heart and blood sugars quickly begin to normalize. However, he never saw his doctor and never had is blood pressure medications adjusted. Because of the normalization that can occur in as rapidly as 1-2 weeks, the medications became much too strong, he passed out and ended up in the emergency room. These dietary principles are effective. They are often just as powerful as a number of the medications that we routinely prescribe.
Point of Focus: Please see your doctor before beginning any of these dietary recommendations, especially if you have any underlying medical conditions including Hypertension, Diabetes, Congestive Heart Failure, Coronary Artery Disease, Gout, Kidney Stones, etc., please do not try the dietary changes alone. Find a physician trained in the use of this type of dietary lifestyle in combination with close monitoring of your blood pressure, blood sugar and other key vital signs.
Stay tuned for Ketogenic Principles . . . Part II in the series where we’ll address Food Psychology, To Cheat or Not to Cheat, and Keeping it Real . . .
I have found, over time, that happiness in life seems to be the greatest when I strive for balance in the three basic aspects of life: Mind, Body & Spirit. Yes, I am a physician, and I spend the majority of my day applying advise and treatment plans that have been demonstrated to be effective through the tried and true scientific method. However, I know from personal experience, and from working closely with patients for over 15 years, that science alone, does not bring fullness and happiness to life. Truth and learning can be found through study and also by faith. Finding balance and peace physically is important, but finding that balance emotionally and spiritually are often essential. Being able to follow a Ketogenic Lifestyle effectively over the long term (longer than 6 months) actually requires understanding of some basic principles. This is the first in a series of articles regarding The Principle Based Ketogenic Lifestyle.
I treat patients with obesity, one of the most difficult diseases to address in the medical office. I find that just applying diet alone doesn’t always solve the problem. If the patient’s life is out of balance emotionally or spiritually, the stress this causes often halts effective weight loss and metabolic healing. You may disagree with me on political or religious issues, but healing is not about politics nor is it about religious doctrine – it is about understanding where we are, the path forward, and our potential to get there. The mind, body and spirit are deeply interconnected. Often, until we recognize and treat those connections, true healing cannot occur.
The first step in treating any illness, including weight, is recognition of the problem. The Medical Community has recognized Obesity as a disease, but obesity is also a symptom of underlying physical metabolic dysfunction that may be tied to the mind and spirit. Daily journaling is the tool that lets one see if the dysfunction is tied to mind or spirit. I ask my patients to keep a daily food journal. This is very important in looking at the patterns of macro-nutrient intake. But the more powerful effect of journaling allows one to see how food is tied to emotion – mentally and spiritually.
Simply writing down what you eat each day, when you eat it, and how you felt after you at it is actually quite profound. The patterns that emerge are usually seen and identified by the patient long before I ever see them. In fact, patient’s often bring those patterns up before ever showing me their food journals.
I’ve found, in keeping a food journal myself, that combining my journaling with other other daily goals, uplifting thoughts and reminders was even more helpful and powerful. This can be done on paper, a notebook, a planner or even on the computer. (I have a few patients who are accountants or engineers – they bring in complex spread sheets). What is important is daily consistency. It takes about 3-4 weeks of journaling to begin to see patterns.
I have taken the advise of one of the leaders of my church to “ponderize” a scripture, meaningful poetic verse or truth filled quote each week as part of the journaling process. He defined “ponderizing” as the act of pondering and memorizing a scripture or a favorite uplifting poem or verse each week. This is done by writing the verse on a written card or note in a place that you will see it frequently each day during the week. When you see it, read it and ponder it. Just the process of frequently reading it will lead to memorization each week. I have found that reading and pondering a verse 3-4 times a day for a week, lends itself to easy memorization. Each time you read the verse, think about it and ponder it for a moment, then go on with your day. This will give you a brief opportunity to elevate your thoughts each day, and will give you a place your mind can go and think when you don’t have to think. It gives your subconscious mind the ability to solve complex patterns at a higher level.
Said David O. McKay, “Tell me what you think about when you don’t have to think, and I’ll tell you what you are.” “As a man thinketh in his heart, so is he . . . ” (Proverbs 23:7).
For some reason, with all the cares of the day, work, family and the challenges of life, I have fallen out of this habit for some time. When this leader mentioned this process in his comments, I was reminded of the peace and balance I used to feel each week when doing this simple activity. I have recommitted myself to restart this activity and I invite you to do the same. This time to ponder opens your mind and allows you access the deeper worries and fears holding you from what you what to accomplish. It takes great courage to make permanent lifestyle and dietary changes. When someone can’t clearly see what lies ahead, it fills them with fear, doubt or both. But journaling, even in its simplest form, gives a person the ability to resist and then master the patterns that have kept them from change. As Mark Twain said, “Courage is resistance to fear, mastery of fear – not absence of fear.”
Courage is tested when we purse difficult goals, fight against disease with unknown outcomes, or work to regain health. The testing can be painful. Journaling, and ponderizing in the process, gives courage to take small steps, one day at a time. Admitting to, journaling when we fail or make mistakes, fear of failure or feeling unsure actually increases our courage. Being given a week to ponderize an uplifting scripture or verse enhances that courage . Journaling successes and failures empowers us individually. The psychiatrist Carl Jung wrote:
“There appears to be a conscience in mankind which severely punishes the man who does not somehow and at some time, at whatever cost to his pride, cease to defend and assert himself, and instead confess himself fallible and human. Until he can do this, an impenetrable wall shuts him out from the living experience of felling himself a man among men. Here we find a key to the great significance of true unstereotyped confession – a significance known in all the initiation and mystery cults of the ancient world, as is shown by a saying from the Greek mysteries: ‘Give up what thou hast, and thou will receive.'”
Journaling and ponderizing allows one a form of confession and renewal. It gives one courage that you have survived today’s challenges and seen the pattern of fallibility in them. It is actually energizing. And, the path to healing begins to become clear.
Journaling also is a great way to outline side effects from carbohydrate withdrawl that will last for 2-4 weeks (That’s for another blog post, however).
Feel free to ask me about the verse that I am ponderizing each week. I will happily tell you which verse I am pondering and memorizing; but, I will in tern, ask you which verse you are ponderizing.
This week, the verse I am ponderizing comes from the Bible – Genesis 35:2-3:
“Then Jacob said unto his household, and to all that were with him, Put away the strange gods that are among you, and be clean, and change your garments: And let us arise, and go up to Beth-el; and I will make there an altar unto God, who answered me in the day of my distress, and was with me in the way which I went.”
Did you begin your food journal? And, what verse are you going to ponderize this week?


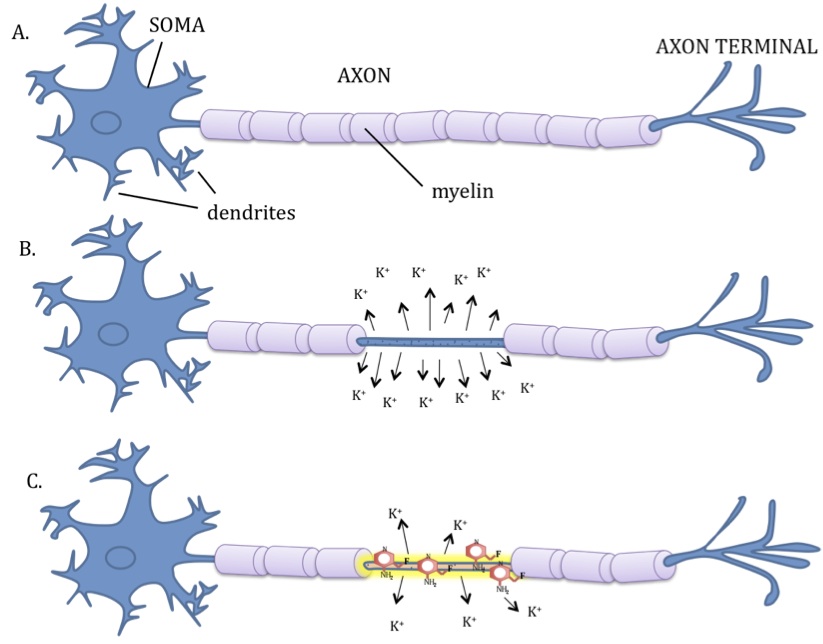










 That something else should be fat. Protein must be moderated, as it will also be stored as fat if you eat too much. So, if the carbohydrates are kept low, fat intake can be increased and the body will pick the fat it wants and essentially throw the rest out without raising cholesterol, causing weight gain or causing heart disease. This is why we want you to use good natural animal fats like butter, hard cheese, olive oil, coconut oil, avocado, etc. Look for fats highest in omega-3 fatty acids as these decrease inflammation and improved weight loss. Look for meats highest in fat like red meat (55% fat) and pork (45% fat). Take the food pyramid and flip it over.
That something else should be fat. Protein must be moderated, as it will also be stored as fat if you eat too much. So, if the carbohydrates are kept low, fat intake can be increased and the body will pick the fat it wants and essentially throw the rest out without raising cholesterol, causing weight gain or causing heart disease. This is why we want you to use good natural animal fats like butter, hard cheese, olive oil, coconut oil, avocado, etc. Look for fats highest in omega-3 fatty acids as these decrease inflammation and improved weight loss. Look for meats highest in fat like red meat (55% fat) and pork (45% fat). Take the food pyramid and flip it over.
 20% of women that I see in my practice who are over 55 years old, need some degree of estrogen replacement before they are able to lose weight. Estrogen plays a very large role in regulation of the metabolism and when deficient, causes weight retention or weight gain. Talk to your doctor about the risks and benefits of estrogen for you individually in this situation.
20% of women that I see in my practice who are over 55 years old, need some degree of estrogen replacement before they are able to lose weight. Estrogen plays a very large role in regulation of the metabolism and when deficient, causes weight retention or weight gain. Talk to your doctor about the risks and benefits of estrogen for you individually in this situation.
 People with significant stressors in their life have been show to have an increased corsiol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing a daily, cyclic over production of cortisol and then normalization of cortisol after resolution of the stressor. This cortisol response is not high enough to lead to a true
People with significant stressors in their life have been show to have an increased corsiol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing a daily, cyclic over production of cortisol and then normalization of cortisol after resolution of the stressor. This cortisol response is not high enough to lead to a true  Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids or proteins into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues (by stimulating insulin production) and turns on the maturation process of adipocytes (it makes your fat cells age – nothing like having old fat cells, right?!) In the process, cortisol suppresses the immune system through an inhibitory effect designed to decrease inflammation during times of stress (7,8,9). If this was only occurring once in a while, this cascade of hormones acts as an important process. However, when cortisol production is chronically turned up, it leads to abnormal deposition of fat (weight gain), increased risk of infection, impotence, abnormal blood sugars, brain fog, head
Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids or proteins into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues (by stimulating insulin production) and turns on the maturation process of adipocytes (it makes your fat cells age – nothing like having old fat cells, right?!) In the process, cortisol suppresses the immune system through an inhibitory effect designed to decrease inflammation during times of stress (7,8,9). If this was only occurring once in a while, this cascade of hormones acts as an important process. However, when cortisol production is chronically turned up, it leads to abnormal deposition of fat (weight gain), increased risk of infection, impotence, abnormal blood sugars, brain fog, head

































{kind=link}