

I’ve been living and teaching patients about using a low-carb/ketogenic and carnivorous lifestyles for over 16 years. I get thousands of questions each month about what to eat. People ask:
- “What foods are ketogenic lifestyle approved?”
- “Can you just give me a list of approved keto foods?”
- “But, can’t I just have some oatmeal?”
In the past, I’ve given people seven day diets, and I’ve given them food lists. But, you know the proverb, “give a man a fish . . .” People still seem confused. I’ve tried teaching people the simple ketogenic principles, “teach a man to fish . . .” and this helps a few others. However, there still seems to be great confusion about what foods can and should be used in a ketogenic lifestyle. Today, I thought I would try to combine both approaches and discuss the basic macro-nutrients that make up a well formulated ketogenic diet.
Carbohydrates
Let’s start with carbohydrates. The first principle that must be followed to enter and stay in ketosis is keep insulin from spiking. This is done by keeping total carbohydrate intake less than 20 grams per day. The liver produces a small amount of carbohydrate every day to protect the brain. Therefore, a low baseline level of continuous insulin production is essential to maintain life. However, it’s the large spikes of insulin after ingesting carbohydrate containing meals that cause the problems. We talk about this at length in my book The Keto Cure.
Carbohydrates are the foods that most commonly cause insulin to spike. It is the rapid rise or spike of insulin levels that drive weight gain, arterial plaque formation, heart disease, inflammation, neuropathy, kidney stones, gout and thyroid problems. Simple and complex carbohydrates cause insulin to surge. Those same simple and complex carbohydrates are the sugars (monosaccharides & disaccharides) and starches (polysaccharides) found in foods.
Fibers are also complex carbohydrates (polysaccharides) in the form of cellulose, lignin and pectin that are more difficult for human digestive enzymes to break down into simple digestible forms of carbohydrate. However, juicing, blending or cooking fibers releases the carbohydrate from the complex form and makes them available to our bodies.
Carbohydrates in their various forms are present in varying amounts in foods like fruit, vegetables, grains, beans, legumes, milk, and processed foods like candy, soda & sweets. (These are the foods to limit or completely avoid).

In general, raw leafy greens contain cellulose and the carbohydrates in these vegetables when eaten raw do not need to be counted. You are free to eat as much as you desire. However, cooking, blending or juicing the leafy green (as noted below) does break the cellulose bonds and increases carbohydrate absorption (that is why cooked, blended, or juiced vegetables taste “sweeter”).
NOTE: I recommend 1-2 cups of raw leafy greens per day. Leafy greens are one of the highest sources of folic acid (spinach, asparagus & okra) and without them in the diet, there is a potential risk of folate deficiency if it isn’t present in animal fat sourcesa. This is especially problematic in pregnant and breast feeding mothers. Yes, I hear you, eggs and meat are another source of folic acid; however, leafy greens like spinach contain four times the folic acid that eggs and meats do. Even iceberg lettuce contains more folic acid than eggs (this is why I caution pure carnivore diets in women of child bearing age without folic acid supplementation).
Foods that are loaded with sugars and starches that should be AVOIDED or USED WITH GREAT PRUDENCE include:
Non-Leafy Green Vegetables (1 cup raw or 1/2 cup cooked) – 10 grams of carbohydrate
Asparagus
Bamboo Shoots
Beans (yellow or green)
Beets
Broccoli
Brussell sprouts
Cauliflower
Cabbage
Celery Leaves
Egg Plant
Leeks
Mushrooms
Okra
Onions
Green Onions
Scallions
Pea Pods
Peppers: Green, Red, Sweet, Hot
Sauerkraut
Spinach
Summer Squash
Turnips
Tomato
Zucchini
(Corn, Carrots and Potatoes are not listed here due to their higher carbohydrate content)
Fruits (portions below) – 15 grams of carbohydrate
Apple (1 small)
Apple Juice (1/2 cup)
Apple Sauce (1/2 cup)
Apricots (2 fresh) Page | 5
Banana (1/2)
Berries (blueberries, black berries, strawberries, loganberries, raspberries – 1 cup)
Cantaloupe (1/4 of a 6 inch melon)
Cherries (12)
Cranberries (1 cup)
Dates (3)
Figs (Fres
Grapefruit Juice (1/3rd cup)
Grapes (17 small)
Honeydew melon (1/8th of a 7inch melon)
Kiwi (1)
Lemons (2)
Mango (1/2)
Nectar (1/3rd cup canned)
Nectarine (1)
Orange (1 small orange)
Orange Juice (1/2 cup)
Peach (1 medium)
Pear (1 small)
Pineapple (1/2 cup chopped)
Plumbs (2)
Prune Juice (1/3 cup)
Prunes (2 fresh or dried)
Raisins (2 Tbsp)
Rhubarb (1 cup cooked)
Tangerine (1)
Watermelon (4 inch x 1 ½ inch thick wedge)
Breads (portions below) – 20 grams of carbohydrate
Bread: white, wheat, French, rye, pumpernickel (1 slice)
Bagel (1/3rd)
Biscuit or Roll (1 small)
Breadcrumbs (1/4th cup dry, grated)
Bread-stick (1)
Buns: hamburger, hot dog (1/2 bun)
Cereal – cooked (1/2 cup)
Cereal – puffed (1 cup)
Cereal – flakes (1/2 cup)
Corn (1/3rd cup or 1 small cob)
Crackers:
Graham (three 2 ½ inch squares)
Oyster (1/2 cup)
Saltines (5)
Soda (3)
Zwieback (2)

Macaroni noodles (1/2 cup cooked)
Matzo (one 5 inch square)
Muffin – English (1/2 plain)
Muffin – bran (1 small) Page | 6
Toast – Melba (4 rectangles)
Pasta (1/2 cup) Peas – green (1/2 cup)
Pita bread (1 small)
Popcorn – air popped, dry (3 cups)
Potato – New, Russet or sweet (1/2 cup)
Pretzels (3/4th oz)
Rice – cooked (1/3rd cup)
Rice Cakes (2 plain)
Tortilla (1 small)
Dairy (portions below) – 25 grams of carbohydrate
Milk – whole, 1%, 2% and skim (1 cup)
Powdered Skim Milk – dry (1/3rd cup)
Yogurt:
Plain (1 cup)
Light – sweetened with NutraSweet (1 cup)
Regular – fruit filled (1/2 cup)
Cottage Cheese (2 cups)
American Cheese (12 slices)
You may use hard cheeses, cream cheese, sour cream, and mascarpone as great options on a ketogenic diet because they contain very little carbohydrate and are high in fats.
Proteins
Proteins are large molecules made of of long chains of amino acids and are essential for a vast array of functions within the human being including structural formation, enzymatic reactions, immune response, cell adhesion, DNA replication, and molecular transport to name just a few. There are 22 amino acids that make up the protein molecules used in the human body. Interestingly, microorganisms and plants can make all 22 of these amino acids on their own. However, humans (and a number of other mammals) can’t make 15 of these amino acids on our own and we must obtain them from our diets.

How much protein do you actually need? Understanding your individual needs baseline protein needs can be calculated from your ideal body weight (IBW). IBW can be very easily calculated from your height and your level of activity. I give you this calculation because many female patients I see do not eat enough protein. Lack of protein will halt weight loss (as the body thinks it is starving.)
Your daily protein need can be calculated by the following:
Males: IBW = 50 kg + 2.3 kg for each inch over 5 feet. Males need 1.2 g protein per kg of IBW.
Females: IBW = 45.5 kg + 2.3 kg for each inch over 5 feet. Females need 1.0 g protein per kg of IBW.
If you are exercising more than 30 minutes 3 days per week then those values increase to 1.4 grams per kg for females and 1.6 grams per kg for males.
Example:
A 6 foot male’s IBW would be 50 kg + (2.3kg x 12 inches) = 77.6 kg x 1.2g/kg if sedentary or 1.6g/kg if exercising 4-5 days per week.
A 5 foot 4 inch females IBW would be 45.5 kg + (2.3kg x 4 inches) = 54.7 kg x 1.0g/kg if sedentary or 1.4g/kg if exercising 4-5 times per week.
This will give you a starting point for your daily protein needs and you can divide this number by the number of meals per day to get the protein needs at each meal. However, many of my patients after three months of ketogenic living need more protein to continue seeing weight loss.
What if I eat too much protein? There is still significant controversy over exactly how much protein is necessary on a daily basis. The reason is that many amino acids when ingested in significant amounts stimulate an insulin surge by themselves. These include arginine, lysine and tryptophan. Eating proteins that are high in these three amino acids in my very insulin resistant patients will raise insulin enough to halt weight loss, cause worsening inflammation, raise blood pressure and cholesterol.

Do you have to avoid these foods on a ketogenic diet? No, however, when you are using them more than 2-3 times a week, weight loss is inhibited and one’s ability to maintain ketosis is blunted.
However, two recent studies(1, 2) demonstrate that when protein intake is increased beyond a certain threshold, growth hormone counterbalances the insulin response and stimulates muscle growth instead of weight gain. That threshold seems to be around 90 grams of protein per day as women and 150 grams of protein as men.
Yes, this is much higher protein in take than the calculation for baseline protein needs we’ve used for years outlined above. We are learning a great deal about protein. For years, we’ve been missing the mark on protein needs. This revolves around the need of leucine to stimulate muscle growth.
What proteins can you use? The following list should be helpful. Remember that protein and fat often come packaged together in nature. As we discuss below, to maintain adequate ketosis, total fat intake should between 70-90% of your total calories. In order to maintain fat contents greater than 70%, you’ll want to use proteins sources that are the highest in fat (like red meat and pork) or add fat (like cooking in butter or coconut oil) to those that are lower in fat content.
Food: Protein Content: Fat Content:
Ground Beef (75% Lean) – 16 grams per 4 oz. 78%
Steak (Ribeye) – 39 grams per 8 oz. 74%
Steak (Top or Bottom Round) – 33 grams per 6 oz. 53%
Bacon (pan fried) – 3 grams per 1 slice 69%
Sausage (beef) – 14 grams per 3.5 oz. 79%
Sausage (pork) – 17 grams per 3.5 oz. 75%
Pork Chop (boneless) – 18 grams per 3 oz. 31%
Ham (cured whole boneless) – 19 grams per 3.5 oz. 28%
Sockeye Salmon – 23 grams per 3 oz. 22%
Halibut – 23 grams per 3 oz. 19%
Chicken Breast (boneless, skinless) – 24 grams per 3 oz. 18%
Turkey Breast – 24 grams per 3 oz. 15%
Tilapia – 21 grams per 3 oz. 13%
Yellowfin Tuna – 25 grams per 3 oz. 10%
Light Tuna – 22 grams per 3 oz. 8%
Deli Meats:
Pepperoni – 18 grams per 3 oz. 83%
Roast Beef – 21 grams per 3 oz. 48%
Canadian bacon – 17 grams per 3 oz. 42%
Roast Turkey Breast – 18 grams per 3 oz. 15%
Snacks:
Beef Jerky (Jack Links) – 13 grams per 1 oz. 9%
Peanut Butter (Peter Pan Crunchy) – 8 grams per 2 tbsp. 76%
Macadamia nuts, raw 2.2 grams per 12 nuts 89%
Mixed Nuts – 6 grams per 2 oz. 79%
Almonds, raw – 6 grams per 1 oz. 66%
Walnuts, raw – 4 grams per 1 oz. 85%
Sunflower seeds, raw – 6 grams per 1 oz. 76%
Tofu – 12 grams per 3 oz. 30%
Greek Yogurt – 23 grams per 8 oz. 0%
Cheeses:
Cream Cheese – 11 grams per 3.5 oz. 79%
Cheddar Cheese – 24.6 grams per 3.5 oz. 74%
Swiss Cheese – 24 grams per 3 oz. 66%
Ricotta cheese – 10 grams per 3.5 oz. 63%
Eggs – 6 grams per 1 large egg 70%
Look for foods who’s ratio of protein to fat is close to or greater than 1:1. For example, eggs are 6 grams of protein and 6 grams of fat.
It is essential to understand that not all sources of protein are equal in their absorption in the human gut.
- Egg protein utilization – 50%
- Meat protein utilization – 40%
- Cheese protein utilization – 40%
- Whey protein utilization – 18%
- Vegetable protein utilization – 14%
Therefore, the two most important things you can do to optimize your ketogenic lifestyle is lower the carbohydrate intake to less than 20 grams per day, and use adequate high quality protein. Muscle gain and fat loss are most effectively achieved when high quality protein is used.
If you are struggling or just getting started, get a copy of Dr. Nally’s Ketogenic Diet here.



 So, how do you manipulate the hormones in a way to control the rebounding hunger and suppression of metabolism? This is where we put a bit of twist on the knowledge we’ve gained from alternate day fasting. Recent research shows that “mild” energy deficit in a pulsatile manner, that has the ability to mimicking the body’s normal bio-rhythm’s is dramatically effective in reducing weight and maintaining normal hormonal function without cause of rebound metabolic slowing (4).
So, how do you manipulate the hormones in a way to control the rebounding hunger and suppression of metabolism? This is where we put a bit of twist on the knowledge we’ve gained from alternate day fasting. Recent research shows that “mild” energy deficit in a pulsatile manner, that has the ability to mimicking the body’s normal bio-rhythm’s is dramatically effective in reducing weight and maintaining normal hormonal function without cause of rebound metabolic slowing (4).







 If you are interested in the low-carb, moderate protein, high-fat, ketogenic diet, then
If you are interested in the low-carb, moderate protein, high-fat, ketogenic diet, then 

















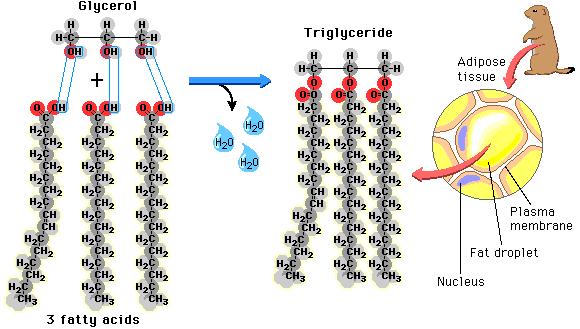 as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
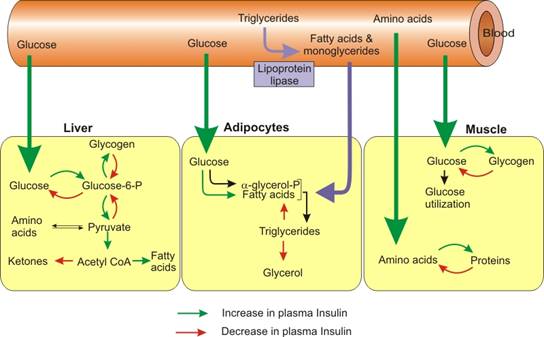 before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).
before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).
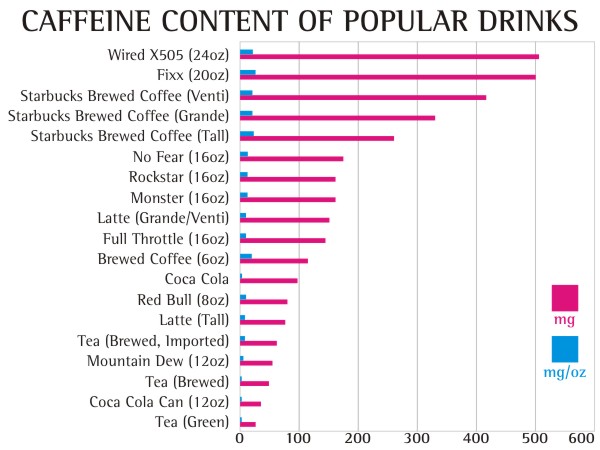
 After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the
After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the 





 That something else should be fat. Protein must be moderated, as it will also be stored as fat if you eat too much. So, if the carbohydrates are kept low, fat intake can be increased and the body will pick the fat it wants and essentially throw the rest out without raising cholesterol, causing weight gain or causing heart disease. This is why we want you to use good natural animal fats like butter, hard cheese, olive oil, coconut oil, avocado, etc. Look for fats highest in omega-3 fatty acids as these decrease inflammation and improved weight loss. Look for meats highest in fat like red meat (55% fat) and pork (45% fat). Take the food pyramid and flip it over.
That something else should be fat. Protein must be moderated, as it will also be stored as fat if you eat too much. So, if the carbohydrates are kept low, fat intake can be increased and the body will pick the fat it wants and essentially throw the rest out without raising cholesterol, causing weight gain or causing heart disease. This is why we want you to use good natural animal fats like butter, hard cheese, olive oil, coconut oil, avocado, etc. Look for fats highest in omega-3 fatty acids as these decrease inflammation and improved weight loss. Look for meats highest in fat like red meat (55% fat) and pork (45% fat). Take the food pyramid and flip it over.
 20% of women that I see in my practice who are over 55 years old, need some degree of estrogen replacement before they are able to lose weight. Estrogen plays a very large role in regulation of the metabolism and when deficient, causes weight retention or weight gain. Talk to your doctor about the risks and benefits of estrogen for you individually in this situation.
20% of women that I see in my practice who are over 55 years old, need some degree of estrogen replacement before they are able to lose weight. Estrogen plays a very large role in regulation of the metabolism and when deficient, causes weight retention or weight gain. Talk to your doctor about the risks and benefits of estrogen for you individually in this situation.










{kind=link}