I’ve been looking for the answer for quite some time. . . what role does caffeine play in your and my weight management journey? The answer gave me a headache. . . literally and figuratively.
As many of you, including my office staff, know, I love my Diet Dr. Pepper (and my bacon). I found that being able to sip on a little soda throughout the day significantly helped the carbohydrate cravings and munchies during a busy and stressful day at the office. Diet Dr. Pepper contains caffeine, however, I wasn’t really worried. Caffeine has been well know to have a thermogenic effect which increases your metabolism and has been thought for many years to help with weight loss among the weight loss community.
Diet Dr. Pepper is, also, one of only four diet sodas on the grocery store shelves that doesn’t contain acesulfame potassium (click here to see why most artificial sweeteners cause weight gain). The four diet sodas that I have been comfortable with my patients using are Diet Dr. Pepper, Diet Coke, Diet Mug Root-beer and Diet A&W Cream Soda. These are the last four hold out diet sodas that still use NutraSweet (aspartame) as the sweetener. Most of the soda companies have switched the sweetener in their diet sodas to the insulinogenic acesulfame potassium because it tastes more natural and aspartame has been given a media black eye of late. However, NutraSweet (aspartame) is the only sweetener that doesn’t spike your insulin or raise blood sugar (click here to find out why that is important).
Yes, I know. The ingestion of 600 times the approved amount of aspartame causes blindness in lab rats (but we’re not lab rats, and . . . have you ever met someone that drinks 600 Diet Dr. Peppers in a day? The lethal dose of bananas, which are high in potassium that will stop your heart, is 400). Aspartame can also exacerbate headaches in some (about 5% of people) and I’ve had a few patients with amplified fibromyalgia symptoms when they use aspartame. But for most of us, its a useful sweetener that doesn’t spike your insulin response, halting or causing weight gain.
But, over the last few years, I’ve noticed that increased amounts of Diet Dr. Pepper & Diet Coke seem to cause plateauing of weight and decreasing the ability to shift into ketosis, especially mine. I’ve also noticed (in my personal n=1 experimentation) that my ability to fast after using caffeine regularly seems to be less tolerable, causing headaches and fatigue 8-10 hours into the fast, symptoms that don’t seem to let up until eating. Through the process of elimination, caffeine seems to be the culprit.
After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the August 2004 Diabetes Care Journal screamed for my attention.
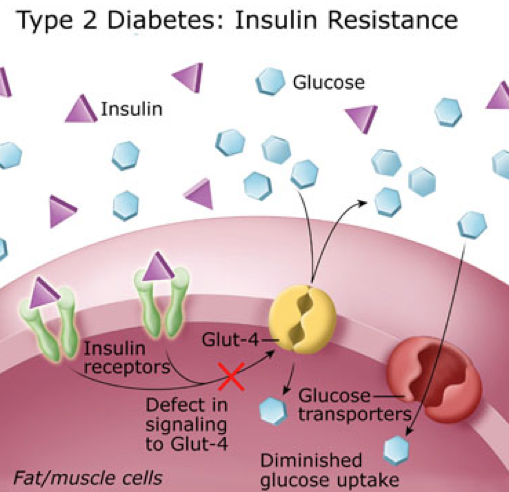
It appears that caffeine actually stimulates a glucose and insulin response through a secondary mechanism. The insulin surge and glucose response is dramatically amplified in patients who are insulin resistant. Caffeine doesn’t effect glucose or insulin if taken while fasting; however, when taken with a meal, glucose responses are 21% higher than normal, and insulin responses are 48% higher in the insulin resistant patient. Caffeine seems to only effect the postprandial (2 hours after a meal) glucose and insulin levels. The literature shows mixed responses in patients when caffeine is in coffee or tea, probably due to the effect of other organic compounds (1).
Caffeine effect on plasma glucose and plasma insulin compared to placebo (1).
Caffeine also diminishes insulin sensitivity and impairs glucose tolerance in normal and already insulin resistant and/or obese patients. This is seen most prominently in patients with diabetes mellitus type II (stage IV insulin resistance). Caffeine causes alterations in glucose homeostasis by decreasing glucose uptake into skeletal muscle, thereby causing elevations in blood glucose concentration and causing an insulin release (2-6).
Studies show that caffeine causes a five fold increase in epinephrine and a smaller, but significant, norepinephrine release. The diminished insulin sensitivity and exaggerated insulin response appears to be mediated by a catacholamine (epinephrine, norepinephrine & dopamine) induced stress response (5). Caffeine has a half life of about 6 hours, that means the caffeine in your system could cause a catacholamine response for up to 72 hours depending upon the amount of caffeine you ingest (7).
The reason for my, and other patient’s, headaches and fatigue after a short fast was due to the exaggerated stress hormone response. Increased levels of insulin were induced by a catacholamine cascade after caffeine ingestion with a meal, dramatically more amplified in a person like me with insulin resistance. The caffeine with the last meal cause hypoglycemia 5-7 hours into the fasting, leading to headaches and fatigue that are only alleviated by eating.
Even when not fasting, the caffeine induced catacholamine cascade causes up to 48% more insulin release with a meal, halting weight loss and in some cases, causing weight gain.
Caffeine is not the “Wonder-Boy” we thought it was.
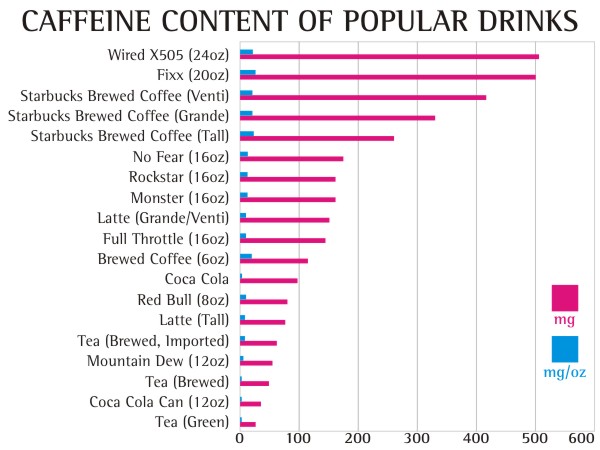
How much caffeine will cause these symptoms? 50 mg or more per day can have these effects.
10,000 mg (10 grams) – lethal dose (Yes, 25 cups of Starbucks Coffee can kill you)
The equivalent of 100 mg of in a human was given to a spider, you can see the very interesting effect on productivity. How often does the productivity of the day feel like the image below?
Normal Spider (9)Spider on caffeine (9)
Beware that caffeine is now being added to a number of skin care products including wrinkle creams and makeup. Yes, caffeine is absorbed through the skin, so check the ingredients on your skin care products.
Diet Dr. Pepper, my caffeine delivery system of choice, has slightly less caffeine (39 mg per 12 oz can or 3.25 mg per oz) than regular Dr. Pepper. I found myself drinking 2-3 liters of Diet Dr. Pepper per day (long 16-18 hour work days in the office). After doing my research, I realized that my caffeine tolerance had built up to quite a significant level (230-350 grams per day).
So, a few weeks ago, I quit . . . cold turkey.
Did I mention the 15 withdrawal symptoms of caffeine? (8)
Headache – behind the eyes to the back of the head
Sleepiness – can’t keep your eyes open kind of sleepiness
Irritability – everyone around you thinks you’ve become a bear
Lethargy – feels like your wearing a 70 lb lead vest
Constipation – do I really need to explain this one?
Depression – you may actually feel like giving up on life
Muscle Pain, Stiffness, Cramping – feel like you were run over by a train
Lack of Concentration – don’t plan on studying, doing your taxes or performing brain surgery during this period
Flu Like Illness – sinus pressure and stuffiness that just won’t clear
Insomnia – you feel sleepy, but you can’t sleep
Nausea & Vomiting – You may loose your appetite
Anxiety – amplified panic attacks or feeling like the sky is falling
Brain Fog – can’t hold coherent thoughts or difficulty with common tasks
I experienced 13 of the 15 that lasted for 4 days. I do not recommend quitting cold turkey unless you have a week off and someone to hold your hand, cook your meals and dose your Tylenol or Motrin. My wife thought I was dying. . . I thought I was dying on day two. I actually had a nightmare about buying and getting into my own coffin. It can take up to three weeks to completely recover from caffeine withdrawal.
The other way to quit is to decrease your caffeine intake by 50 mg every two days. That means decrease caffeine by:
1 can of soda every two days
1/4 cup of coffee every day
1/2 can of Energy Drinks every two days
1 cup of tea every two days
The benefit of this method is that withdrawal symptoms are much less severe without the caffeine headache and the ability to remain productive. It will take longer, but quitting cold turkey is not a pretty picture. Been there . . . done that, . . . and I’m not going back. I actually lost another half inch off my waistline by day 5 of caffeine discontinuation.
What is the take home message here? If you have any degree of insulin resistance, caffeine makes it worse and will amplify your weight gain as well as decrease the productivity of your day.
How do you know if you're insulin resistant? What questions need to be asked? What should your numbers be? And, many other great ketosis questions. Also, why does Dr. Nally look like he has dirt on his chin? See it here . . .
Diseases seem to arrive in three’s each day in my office. Today I had three different patients with cholesterol concerns who were notably confused about what actually makes the cholesterol worse, and what causes weight gain. Each of them, like many patients that I see, were stuck in a state of confusion between low fat and low carbohydrate lifestyle change. My hope is to give my patients and anyone reading this blog a little more clarity regarding what cholesterol is, how it is influenced and how it affect our individual health.
First, the standard cholesterol profile does not give us a true picture of what is occurring at a cellular level. The standard cholesterol panel includes: total cholesterol (all the forms of cholesterol), HDL (the good stuff), LDL-C (the “bad” stuff) and triglycerides. It is important to recognize that the “-C” in these measurements stands for “a calculation” usually completed by the lab, and not an actual measurement. Total cholesterol, HDL-C and triglycerides are usually measured and LDL-C is calculated using the Friedewald equation [LDL = total cholesterol – HDL – (triglycerides/5)]. (No, there won’t be a quiz on this at the end . . . so relax.)
However, an ever increasing body evidence reveals that the concentration and size of the LDL particles correlates much more powerfully to the degree of atherosclerosis progression (arterial blockage) than the calculated LDL concentration or weight (1, 2, 3).
There are three sub-types of LDL that we each need to be aware of: Large “fluffy” LDL particles (type I), medium LDL particles (type II & III), and small dense LDL particles (type IV).
Weight & Size of VLDL, LDL & HDL
Why LDL-C is misleading: Identical LDL-C of 130 mg/dL can have a low risk (Pattern A) with a few “big fluffy LDL particles or high risk (Pattern B) with many small dense LDL particles.
Second, it is important to realize that HDL and LDL types are actually transport molecules for triglyceride – they are essentially buses for the triglycerides (the passengers). HDL can be simplistically thought of as taking triglycerides to the fat cells and LDL can be thought of as taking triglycerides from the fat cells to the muscles and other organs for use as fuel.
Third, it is the small dense LDL particles that are more easily oxidized and because of their size, are more likely to cause damage to the lining of the blood vessel leading to damage and blockage. The large boyant LDL (“big fluffy LDL particles”) contain more Vitamin E and are much less susceptible to oxidation and vascular wall damage.
Eating more fat or cholesterol DOES NOT raise small dense LDL particle number. Eating eggs, bacon and cheese does not raise your cholesterol! What increases small dense LDL particles then? It is the presence of higher levels of insulin. Insulin is increased because of carbohydrate (sugars, starches or fruits) ingestion. It is the bread or the oatmeal you eat with the bacon that is the culprit. The bread or starch stimulates and insulin response. Insulin stimulates the production of triglycerides and “calls out more small buses” to transport the increased triglyceride to the fat cells (4, 5, 6, 7).
Fourth, following a very low carbohydrate diet or ketogenic diet has been demonstrated to decreased small dense LDL particle number and correlates with a regression in vascular blockage (8, 9). So, what does this really mean to you and me? It means that the low-fat diet dogma that that has been touted from the rooftops and plastered across the cover of every magazine and health journal for the last 50 years is wrong. . . absolutely wrong.
I talk about this and answers questions on today’s Periscope. You can see the recording on Katch.me with the comments in real time here:
Superko HR, Gadesam RR. Is it LDL particle size or number that correlates with risk for cardiovascular disease? Curr Atheroscler Rep. 2008 Oct;10(5):377-85. PMID: 18706278
Rizzo M, Berneis K. Low-density lipoprotein size and cardiovascular risk assessment. QJM. 2006 Jan;99(1):1-14. PMID: 16371404
Rizzo M, Berneis K, Corrado E, Novo S. The significance of low-density-lipoproteins size in vascular diseases. Int Angiol. 2006 Mar;25(1):4-9. PMID:16520717
Howard BV, Wylie-Rosett J. Sugar and cardiovascular disease: A statement for healthcare professionals from the Committee on Nutrition of the Council on Nutrition, Physical Activity, and Metabolism of the American Heart Association. Circulation. 2002 Jul 23;106(4):523-7. PMID: 12135957
Elkeles RS. Blood glucose and coronary heart disease. European Heart Journal (2000) 21, 1735–1737 doi:10.1053/euhj.2000.2331
Stanhope KL, Bremer AA, Medici V, et al. Consumption of Fructose and High Fructose Corn Syrup Increase Postprandial Triglycerides, LDL-Cholesterol, and Apolipoprotein-B in Young Men and Women. The Journal of Clinical Endocrinology and Metabolism. 2011;96(10):E1596-E1605.
Shai I et al. Cirulation. 2010; 121:1200-1208
Krauss RM, et al. Prevalence of LDL subclass pattern B as a function of dietary carbohydrate content for each experimental diet before and after weight loss and stabilization with the diets. American Journal of Clinical Nutrition. 2006; 83:1025-1031
Gentile M, Panico S, et al., Clinica Chimica Acta, 2013, Association between small dense LDL and early atherosclerosis in a sample of menopausal women, Department of Clinical Medicine and Surgery, University “Federico II” Medical School, Naples, Italy Division of Cardiology, Moscati Hospital, Aversa, Italy A. Cardarelli Hospital, Naples, Italy
This week I had the pleasure of seeing a really nice 46 year old Hispanic male who is fairly new to the office. He came back in to see me in follow up on his diabetes. To give you a bit of background history, the patient came to see me about 6 months ago, just not feeling very well. Based on his symptoms of fatigue, history of elevated blood sugar and family history, lab work was completed.He saw us initially with a Hemoglobin A1c of 12.3% in June (normal should be 4.9%-5.6%). This means he had an average blood sugar over the previous three months of about 310 mg/dL (normal should be < 110 mg/dL).
Past Medical History include: Diabetes Mellitus – type II (not on any medications when initially seen), Hypertension (high blood pressure), Dyslipidemia (elevated cholesterol) and a non-specific heart arrhythmia.
Medications: None
Surgeries: Knee & shoulder arthroscopies
Family History: Father Diabetes, Stroke, Heart Disease, Hypertension, Elevated Cholesterol
After getting his labs back, we had a very long conversation about the need to either fix his diet dramatically, or he may be looking at using 3-4 oral medications or even insulin to control his blood sugar.
When I see average blood sugars (HbA1c) stay over 6.5% (or greater than 140 mg/dL), the risk for retinal, kidney and nerve damage is significant and often irreversible after 4-5 years. Most physican’s are affraid to lower the HbA1c to less than 7.0% with medications due to low blood sugar events, and so the diabetes community has “settled” with 7.0% as being effective. However, it still isn’t low enough. I saw this happen with my father and with other members of me family. I’ve seen it happen over and over with my patients over the last 15 years when they have not lowered their blood sugar and reduced the high insulin loads that occur in response to those high blood sugar levels. It has been my experience that HbA1c can be very safely lowered to the normal range, as low as 5.2-5.6% without symptomatic low blood sugars, with the correct diet and careful use of medications.
As you can see, a dramatic change in his blood sugar has occurred in a three month interval. Not only that, we see a significant change in his cholesterol profile.
Previously, we looked at LDL-C for heart disease risk, however, I have multiple patients that have had heart disease with normal LDL-C ( <100 mg/dL). LDL-C is just a summation of all the particles. The LDL particle is actually made up of three sub-types and it is specifically the small dense particle that causes the vascular risk. You can see a dramatic normalization of the small dense particle LDL with no change in LDL-C and minimal change in Total Cholesterol in the patient’s labs when he reduces his carbohydrate intake. This is a pattern I see every single day. When serial carotid ultrasound studies are completed, I see reduction in blockage and reduction in the vascular wall thickening. I will be very interested to see the vascular studies on this patient and I will await his results as he tightens up his diet even further.
All in all, he has dramatically brought his diabetes under control with carbohydrate restriction and if he continues this lifestyle, he has reduced his risk for retinal damage, reduced his risk for kidney damage, reduced his risk for nerve damage and essentially added 20 years to his life.
(Disclosures: Dr. Nally has no vested interest, monitary or otherwise, in Novo Nordisc or it’s products including liraglutide.)
I can’t help myself. Some days I enjoy a good murder mystery, but on others, I enjoy a good journal article elucidating our understanding of leptin. No, leptin is not a tiny Irish folk character or even a superhero. Leptin is a hormone. It’s made by fat cells. Anything made by fat cells becomes fascinating to a “fat doctor.”
Why is learning about leptin illuminating?
Well, if Sir Arthur Conan Doyle was an Obesity Specialist, the mystery would have been that Mr. Plump was killed by the wrench in the kitchen, but the wrench seems to have never left tool case in the garage. No one has been able to figure out how leptin, the allegorical wrench, plays its roll in lepin resistance. We know that a lack of leptin allows hunger to persist and a person without leptin will continue to eat without the sensation of feeling full – leading to obesity. What we haven’t understood is – what causes the brain to no longer sense larger and larger amounts of leptin being produced by those who are obese.
That is . . . we haven’t understood it until now. . .
We have known for some time that the hormone leptin is a key hormone produced by the adipose (fat) cells that suppresses hunger. A majority of obese patients in my clinic have elevated circulating leptin levels 2-10 times the normal levels. We know that a lack of leptin leads to obesity, but the patients that I see in the office are producing an over abundance consistent with leptin resistance. The leptin signal is not being recognized by the brain. This is very similar to type II diabetes and insulin resistance. The pancreas is producing an over abundance of insulin, but the cells are recognizing the signal to let the glucose in through the door way.
Three recent and very interesting studies have pointed to the probable cause. First, one of the most common genetic disorders causing human obesity is loss of function of the melanocortin receptor.
Image adapted from 2011 “The Skinny About Fat” presentation – Adam Nally, D.O.
If the MC-4R receptor is broken, suppression of appetite is limited, continued eating occurs and weight gain continues. Leptin, produced by every adipose cell in the body, is carried in the blood stream to the brain and must pass through the blood-brain barrier. Once it crosses the blood-brain barrier and enters the hypothalamus, it has a stimulatory effect on the MC-3R receptor in the Arcuate Nucleus of the hypothalamus causing stimulation of the MC-4R receptor in the Parventricular Nucleus and Lateral Hypothalamus to turn off hunger.
Image adapted from 2011 “The Skinny About Fat” presentation – Adam Nally, D.O.
However, if leptin cannot cross the blood brain barrier, the signal is never received from the adipose cells and continued eating without satiation (feeling full) persists. Studies have shown that dietary fructose ingestion alone or in combination with diets high in fat suppress the transmission of leptin across the blood-brain barrier.
Image adapted from 2011 “The Skinny About Fat” presentation – Adam Nally, D.O.
Fructose is the primary component of high-fructose corn syrup, and makes up 45-50% of every other type of natural form of sugar (sucrose). Yes, it’s the major component found in table sugar, brown sugar, honey, agave, molasses and maple syrup. This is why a Paleolithic Diet isn’t fully effective for people with leptin resistance.
Lastly, anything that raises triglycerides inhibits leptin from crossing the blood-brain barrier.
Image adapted from 2011 “The Skinny About Fat” presentation – Adam Nally, D.O.
Insulin has a direct effect on triglycerides. (See the articles “Insulin Resistance & The Horse,” “Fat Thoughts on Cholesterol,” “Ketogenic Living” and “So, What is this Ketogenic Thing?“). If your insulin levels go up, triglyceride production goes up. The patient with insulin resistance, pre-diabetes, impaired fasting glucose or type II diabetes produces between two to ten times the normal amount of insulin when eating the standard American diet (SAD diet). These patients have significant triglyceride elevation because of the high insulin response to carbohydrates in their diet. (Many of them were told by their doctor that “It’s just genetic so take your Lipitor.”) Statin drugs lower the LDL-C (calculated “bad cholesterol” level), but don’t reduce triglycerides effectively. Inadequate treatment of high triglycerides allows poor blood-brain barrier transmission of leptin and worsening leptin resistance.
In fact, this is the challenge and problem with the “frequent fasting” or “intermittent fasting” fad for weight loss that has been popping up in the blogosphere. If fasting reaches a state of starvation (which is a very fine line metabolically), it stimulates a stress response . . . causing a spike in cortisol, release of glycogen (a form of sugar), a compensatory release of insulin and a spike in triglycerides. If you have tried intermittent fasting and you’ve gained weight, you are probably not “fasting,” your probably “starving.” We’ve known for years that triglycerides are elevated in starvation. This diminishes leptin’s ability to cross the blood-brain barrier and leads to worsening leptin and insulin resistance.
High leptin levels caused by leptin resistance also seems to play a significant role in the development of diabetic retinopathy – damage to the tiny blood vessels at the back of the eye feeding the retina. Diabetic retinopathy starts insidiously without any symptoms initially and can lead to eventual blindness if not treated. Leptin seems to upregulate vascular endothelial growth factor (VEGF) which leads to narrowing of the blood vessels called “ischemia.” Chronic ischemia of the retinal vessels leads to damage to the delicate retinal cells of the eye.
So what do you do if you have leptin resistance. First, eliminate carbohydrates from your diet, especially sugars, high fructose corn syrup and any other form of simple sugar. This is why I am such a big fan of low carbohydrate, high fat diets.
Third, use a supplement containing alpha-lipoic acid, carnosine high gamma vitamin E and benfothiamin (derivative of Vitamin B1). These have been demonstrated to decrease inflammation and render protection to the blood vessels.
The use of Epigallocatechin gallate (EGCg), a derivative extract of green tea, has been shown to repress hepatic glucose production, one of the insidious factors of insulin resistance, and may play a role in stabilizing the effect insulin has on production of triglycerides. You should consider using KetoEssentials. It is my specially formulated multivitamin that contains all of the above supplements, and includes methylated folic acid (B9), the necessary vitamin B6 & B12, chromium, vandium & zinc that help to further stabilize insulin resistance.
Fourth, get a good night’s sleep. Lack of sleep causes a stress response, increases cortisol, raises blood sugar and insulin leading to further leptin resistance.
Fifth, mild to moderate resistance exercise has been shown for years to improve insulin resistance significantly. If you’re not exercising, take a 20 minute walk 2-3 times per week, ride a bike for 20 minutes, start a weight lifting program, consider yoga or Pilates, Remember, jumping to conclusions, flying off the handle, carrying things too far, dodging responsibility and pushing your luck don’t qualify as resistance exercise.
Above all, if you’re having trouble losing weight, controlling insulin or leptin, see your doctor. He or she can really help.
References:
Ray F. Gariano, Anjali K. Nath, Donald J. D’Amico, Thomas Lee, and M. Rocio Sierra–Honigmann. “Elevation of Vitreous Leptin in Diabetic Retinopathy and Retinal Detachment.” Invest Ophthalmol Vis Sci. 2000;41:3576–3581
Hammes HP, Du X . “Benfotiamine blocks three major pathways of hyperglycemic damage and prevents experimental diabetic retinopathy.” Nat Med. 2003 Mar;9(3):294-9. Epub 2003 Feb 18.
Hipkiss AR, Brownson . “Reaction of carnosine with aged proteins: another protective process?” Ann N Y Acad Sci. 2002 Apr;959:285-94.
Zachary A. Knight, K. Schot Hannan, Matthew L. Greenberg, Jeffrey M. Friedman. “Hyperleptinemia Is Required for the Development of Leptin Resistance.” PLoS ONE 5(6): e11376. doi:10.1371/journal.pone.0011376.
Min-Diane Li. “Leptin and Beyond: An Odyssey to the Central Control of Body Weight.” The Yale Journal of Biology and Medicine. 2011;84(1):1-7.
Eri Suganami, Hitoshi Takagi,Hirokazu Ohashi, Kiyoshi Suzuma, Izumi Suzuma, Hideyasu Oh, Daisuke Watanabe, Tomonari Ojimi, Takayoshi Suganami, Yasushi Fujio, Kazuwa Nakao, Yoshihiro Ogawa and Nagahisa Yoshimura. “Leptin Stimulates Ischemia-Induced Retinal Neovascularization: Possible Role of Vascular Endothelial Growth Factor Expressed in Retinal Endothelial Cells.” Diabetes. September, 2004. vol. 53 no. 9 2443-2448
Joseph R. Vasselli, Philip J. Scarpace, Ruth B. S. Harris, and William A. Banks. “Dietary Components in the Development of Leptin Resistance.” Adv. Nutr. 2013: 4: 164–175.
Joseph R. Vasselli. “Fructose-induced leptin resistance: discovery of an unsuspected form of the phenomenon and its significance.” Am J Physiol Regul Integr Comp Physiol. 2008 Nov;295(5):R1365-9. doi: 10.1152/ajpregu.90674.2008. Epub 2008 Sep 10.
Waltner-Law ME, Wang XL Epigallocatechin gallate, a constituent of green tea, represses hepatic glucose production. J Biol Chem. 2002 Sep 20;277(38):34933-40. Epub 2002 Jul 12.
85% of the people that walk through my office doors have some degree of insulin resistance.
What is “insulin resistance?” It is an over production of insulin in response to ANY form of carbohydrate intake (yes, even the “good carbs” cause an insulin over-response in a person with insulin resistance.)
How do I know this? Because I routinely check insulin levels (I check them every three months) and the down stream markers of insulin on a large number of the patients that I see. I have been fascinated by the fact that a diet high in both sugar and fat [like the Standard American Diet, (SAD) diet] turn on the genetics leading to insulin resistance. Starch and sugar load the genetic gun.
Insulin acts like a key at the glucose doorway of every cell in your body. In many people, the insulin signal is blocked by hormones produced in the fat cell and the the insulin, acting like a “dull or worn out key” – can’t open the glucose doorway as efficiently.
So, the body panics, and releases extra insulin in response to the same load of carbohydrate or glucose. People with insulin resistance will produce between 2-20 times the normal amount of insulin in response to a simple carbohydrate load. Recent studies(1, 2) reveal high cholesterol and diets high in both fat and carbohydrate cause insulin resistance to progress or worsen.
So, instead of producing enough insulin to accommodate the one slice of bread or the one apple that you might eat, the insulin resistant person produces enough insulin for an entire loaf of bread or an entire bushel of apples. This excess insulin then stimulates one or all of the following:
Weight Gain – Insulin directly stimulates weight gain by activating lipoprotein lipase to take up triglycerides into the fat cells. This causes direct storage of fat and increases your waistline. (3)
Elevated Triglycerides – Insulin directly stimulates production of free fatty acids and triglycerides through hepatic gluconeogenesis and is even more notably amplified by the broken signaling mechanism of the FOX-01 phosphorylation mechanism in patients with insulin resistance. (4)
Increased number of Small Dense LDL (sdLDL) particles – Low density lipoprotein (LDL, or “bad cholesterol”) is actually comprised of various sized lipoproteins including small, medium and large. As triglycerides increase, the small dense LDL particle numbers increase. Research points to the fact that it is the small dense particle that is highly atherogenic (leading to the formation of vascular plaques within the arteries). (5, 8)
Elevated Uric Acid – Leptin resistance and insulin resistance syndromes are often found together and are suspected to have significant influence on each other. High insulin loads lead to “sick adipose cells” causing leptin resistance. This has a dramatic effect on hepatic fructose metabolism increasing the production of uric acid. Excess insulin suppresses urinary excretion of uric acid and dramatically increases serum content of uric acid and the risk of kidney stones and gout. (6, 7)
Increased Inflammation – Increased levels of circulating insulin have a direct correlation on raising many of the inflammatory markers and hormones including TNF-alpha and IL-6 in the body (9). Any disease process that is caused by chronic inflammation can be amplified by increased circulating levels of insulin including asthma, acne, eczema, psoriasis, arthritis, inflammatory bowel and celiac disease, etc.
Elevated Blood Pressure – Increased uric acid production from insulin resistance as noted above directly suppresses production of nitric oxide within the vasculature and increases blood pressure (7). This completes the triad of metabolic syndrome (elevated triglycerides & cholesterol, weight gain, and elevated blood pressure) found in patients with insulin resistance.
Water Retention – We have known for many years that insulin affects the way the kidney uses sodium in the distal nephron. Insulin has a direct effect on sodium retention in the kidney. As insulin levels rise, the kidney retains increased levels of sodium (10). Water follows sodium and thereby causes fluid retention. This is the reason that many of my insulin resistant patients who have struggled with leg swelling and edema suddenly improve when they correct their diet and their high circulating insulin levels fall. It is also the reason that many of my patients show up in my office after the holidays with swollen legs and amplified swelling in their varicose veins after cheating on their ketogenic diets.
If you are plagued by any or all of these, my first suggestion is to see your doctor and get screened for insulin resistance. I treat patients with these every day and have reversed these effects in thousands of patients with the correct diet and/or medications. Having seen these signs and patterns over the last 20 years of medical practice, I am still astonished every day by the dramatic effect our diet plays on the hormonal changes within the body. Remember that the food you eat is actually the most powerful form of medicine . . . and the slowest form of pernicious poison.
Cholesterol Elevation Impairs Glucose-Stimulated Ca2+Signaling in Mouse Pancreatic β-Cells, Endocrinology, June 2011, Andy K. Lee, Valerie Yeung-Yam-Wah, Frederick W. Tse, and Amy Tse; DOI: http://dx.doi.org/10.1210/en.2011-0124
Glucose-Stimulated Upregulation of GLUT2 Gene Is Mediated by Sterol Response Element–Binding Protein-1c in the Hepatocytes, DIABETES, VOL. 54, JUNE 2005; Seung-Soon Im, Seung-Youn Kang, So-Youn Kim, Ha-il Kim, Jae-Woo Kim, Kyung-Sup Kim and Yong-Ho Ahn
Selective versus Total Insulin Resistance: A Pathogenic Paradox, Cell Metabolism, Volume 7, Issue 2, 6 February 2008, Pages 95–96, Michael S. Brown, Joseph L. Goldstein
Association between small dense LDL and early atherosclerosis in a sample of menopausal women, Department of Clinical Medicine and Surgery, University “Federico II” Medical School, Naples, Italy Division of Cardiology, Moscati Hospital, Aversa, Italy A. Cardarelli Hospital, Naples, Italy, Gentile M, Panico S, et al., Clinica Chimica Acta, 2013
Sugar, Uric Acid and the Etiology of Diabetes and Obesity. Diabetes. 2013;62(10):3307-3315, Richard J. Johnson; Takahiko Nakagawa; L. Gabriela Sanchez-Lozada; Mohamed Shafiu; Shikha Sundaram; Myphuong Le; Takuji Ishimoto; Yuri Y. Sautin; Miguel A. Lanaspa
Fructose: metabolic, hedonic, and societal parallels with ethanol. J Am Diet Assoc. 2010 Sep;110(9):1307-21. doi: 10.1016/j.jada.2010.06.008. Lustig RH
Cardiovascular Risk in Patients Achieving Low-Density Lipoprotein Cholesterol and Particle Targets. Atherosclerosis. Vol 235; 585-591, May 2014, Peter P. Toth, Michael Grabner, Rajeshwari S. Punekar, Ralph A. QuimboMark J. Cziraky c, Terry A. Jacobson
Chronic Subclinical Inflammation as Part of the Insulin Resistance Syndrome The Insulin Resistance Atherosclerosis Study (IRAS), Circulation, July 2000, 102:42-47; Andreas Festa, MD; Ralph D’Agostino, Jr, PhD; George Howard, DrPH; Leena Mykka¨nen, MD, PhD; Russell P. Tracy, PhD; Steven M. Haffner, MD
The Effect of Insulin on Renal Sodium Metabolism. Diabetologia. September 1981, Volume 21, Issue 3, pp 165-171. R. A. DeFronzo
Whenever you find yourself on the side of the majority, it is time to pause and reflect.
– Mark Twain
Why should we limit ourselves to thinking outside the box. Can’t we just get rid of the box?
True discovery consists in seeing what everyone has seen . . . then, thinking what no one has thought.
People were burned at the stake because they refused to believe the Earth was not the center of the universe. They were beheaded because they had a sneaking suspicion that the world was not flat.
Is it really that hard to accept that our weight gain and diabetes is driven by a hormonal signal, and not by gluttony or caloric intake of fat?
The challenge with the current thought model on the cause of obesity is that it does not account for metabolic syndrome. In the practice of medicine over the last 15 years, an interesting pattern has emerged. I noticed that there was a spike in fasting and postprandial insulin levels 5-10 years prior to the first abnormal fasting and postprandial blood sugars. These patients were exercising regularly and eating a diet low in fat. But they saw continued weight gain and progressed down the path of metabolic syndrome. 10-15 years later, they fall into the classification of type II diabetes.
The only thing that seems to halt this process in these patients is carbohydrate restriction. Fasting insulin levels return to normal, weight falls off, and the diseases of civilizations disappear as insidiously as they arose.
So you tell me, is the world flat? Is the Earth the center of the universe?
I recently read a blog post decrying anyone that would recommend a low carbohydrate / ketogenic diet to their patients.
What?!
In fact, this particular blog outlined a number of “adverse reactions” to a ketogenic diet, and based upon these perceived reactions, the writer advised severe caution with its use in just about anyone. It is important to note at the outset that most of the data this blogger quotes are from older studies completed in children for the treatment of epilepsy with specific liquid ketogenic dietary meal replacements. (Not what you’d expect in a low-carb / ketogenic diet for the average obese adult today.)
Diet Confusion
Thanks to recent misinformation by a number of medical professionals, including the person writing the blog referenced above, a poor understanding of fatty acid metabolism by the general community, and a distinct lack of understanding of human adaptability recorded over the last 5,000-6,000 years, there is still significant confusion about ketogenic diets.
It is important to recognize the crucial fact that the human body is designed to function quite well when supplied any of three macronutrients: carbohydrates, proteins or fats. It does so through an amazing series of enzymatic reactions referred to as the Krebs (tricarboxylic acid) cycle, producing needed ATP (adenosine triphosphate) required for our muscles to contract, our heart to beat and our diaphragm to expand our lungs. What’s even more amazing that that the body was designed to recognize the season we are in based up on the food we eat. That is, until we invented refrigerators in 1913. (Now our bodies think it’s year round summer time . . . wait . . . I live in Arizona where it is year round summer time.)
No, this is not a post about unplugging your refrigerator, living on solar, getting off the grid and saving energy.
Our bodies recognize the seasons we are in based upon inherent hormone release. The key hormone is insulin. Insulin can be looked at as the seasonal indicator to our bodies. Insulin production rises and falls based on our intake of carbohydrates (sugar, starches, some fibers). Insulin, essentially, tells our bodies when it is a “time of plenty” and when it was a “time of famine.” Why? You ask. We didn’t have refrigerators 100 years ago and you were lucky if you had a root cellar. The body needs to know when to store for the famine (the winter) that was around the corner. Insulin is that signal.
During the summer, potatoes, carrots, corn and other fruits are readily available. These are all starchy carbohydrates and they all require the body to stimulate an insulin response so that they can be absorbed. Insulin stimulates fat storage (J Clin Invest. 2000;106(4):473-481. doi:10.1172/JCI10842). Just like bears, our bodies were designed to store for the winter.
If you think back in history, your grandparents probably used stored meats & cheeses that could be salted or smoked for preserving during this time of year. Those crossing the plains were commonly found with pemmican, a concentration of fat and protein used as a portable nutrition source in the absence of other food. (Chapter VIII. Narrative of the Life of David Crockett, of The State of Tennessee, Written by Himself, Sixth Edition [E.L. Carey and A. Hart:Philadelphia] 1834, 1837; Marcy, The Prairie Traveler, p. 31.) Think about conversations you may have had with your grandmother when she told you that for Christmas, she received an orange. A single orange for a gift?! Many of my patients drink 12-15 of them in a glass every morning. The winter diets of our grandparents were very low in starches and carbohydrates. When carbohydrate intake is low, little insulin is produced.
Again, insulin is the hormone that tells you that you’re in “a time of plenty” and stimulates weight gain and cholesterol production to prepare for winter. Those prescribing the use of ketogenic diets understand this innate human adaptive trait, and use it to effect changes in weight, cholesterol and other desired metabolic changes.
Three types of ketones. Uptodate.com, May 2015
Now, let’s define the difference between ketosis and keto-acidosis and try to clarify the misinformation that is being spread around the blogosphere.
A ketone is a molecule the body produces from the breakdown of fat and some proteins (amino acids). There are specifically three types of ketones: beta-hydroxybutyric acid, acetoacetic acid and acetone. If ketosis was “bad,” then why would our bodies produce these molecules? They are not bad, and in fact, multiple studies show that the body is often more efficient and effective when it functions on ketones rather than glucose as its primary fuel source. The body can only supply a limited amount of sugar or glucose for fuel. If you talk to runners, marathoners or triathletes, they will tell you that after about 45-90 minutes of continuous endurance exercise the glucose supply runs out and they will experience what is termed a “bonk” (have a low-blood sugar or hypoglycemic episode). Unfortunately, our bodies can only store about 18-24 hours of glucose.
Metobolic Changes of Ketogenic Diet (American Journal of Physiology – Endocrinology and Metabolism Published 1 June 2007 Vol. 292 no. 6, E1724-E1739 DOI: 10.1152/ajpendo.00717.2006)
However, the body can store days upon days of fat in the form of triglyceride in the fat cells. Triglyceride is broken down into ketones. If glucose is the “unleaded” fuel, you can think of ketones as the “diesel fuel” that is easier to store and runs longer.
The average body functioning on ketones as the primary fuel will have a ketone level measured in the blood somewhere between 0.4 and 4 mmol/L. Because of a balance that is created by the use of ketones and a feedback mechanism that kicks in when the ketone level rises, the body will maintain a pH of around 7.4.
Ketoacidosis is dramatically different. If you are a type I diabetic, you don’t produce any insulin. The feedback mechanism regulating ketone use is broken and the ketone levels and triglyceride breakdown speeds up because the body can’t access glucose and can’t produce insulin. The ketone levels spike and the level can rise to > 25 mmol/L. In the presence of a high blood sugar and high ketone level, the acid level in the blood shifts to a pH of less than 7.3. This is referred to as metabolic acidosis and can be life threatening as the low pH shuts down the bodies’ enzymatic processes and a person becomes critically ill and without treatment, can die. (Kitabchi AE et al., Clinical features and diagnosis of diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults. www.uptodate.com, May 2015.)
If you’re not a type I diabetic, you have nothing to worry about. Regardless of what the “ketogenic nay-sayers” blog about, your liver makes approximately 240g of glucose per day, this stimulates a basal release of insulin which keeps the pH in check. It’s also what keeps weight loss at a consistent pace of around 2-10 lbs per month.
If you are a type I diabetic, don’t fret. Carbohydrate restriction can still be used very effectively. It just takes some balancing and understanding of your individual metabolism. Talk to your physician and/or medical bariatrician about how to follow a carbohydrate restricted diet while using insulin.
What about all the other “adverse effects” the blogosphere and other so-called experts claim about ketogenic diets?
Let’s take them on one by one. Are you ready?
Gastrointestinal (GI) disturbances – Yes. Any time you change your diet you may experience diarrhea, constipation or gassiness. Most of the time, this is because you are either 1) not eating enough leafy greens (fiber) or 2) you’re using a supplement that contains an artificial sweetener. Most of the studies on ketogenic diets did not incorporate fiber and the studies used to make this point were on children who used a ketogenic fat supplement shake or liquid preparations containing these artificial sweeteners to make them palatable. If you have spoken to any bariatrician, they will tell you, the best way to follow a ketogenic diet is to eat real food. If you want to read about the anecdotal GI effects of sweeteners, read the comment section in Amazon about the Haribo Sugar Free Gummy Bears.
Inflammation Risk – In every patient that I have placed on a ketogenic diet in the last 8 years, all inflammatory markers including CRP, Sedimentation Rate and Uric Acid have all decreased. Inflammation gets better on an appropriately formulated ketogenic diet. The older studies of ketogenic diets in children contain most of their fat from Omega-6 fatty acids from vegetable oil which will increase inflammation and oxidative stress, spike the cortisol levels and have the secondary effect of actually raising the triglycerides. (Simopoulos AP,The importance of the ratio of omega-6/omega-3 essential fatty acids, Biomed Pharmacother., 2002 Oct;56(8):365-79.)
Muscle Cramps/Weakness – The process of weight loss occurs by burning fat into CO2 and water. We breathe the CO2 out, but the water produced has to follow salts out through the kidneys. Hence, we lose salts. This can cause weakness and muscle cramps. The solution? Stop restricting salt on a low carbohydrate diet. We are the only mammal that restricts salt and we do it because low-fat diets cause us to retain water. Low carbohydrate diets do the opposite. Use sea salt or sip beef or chicken bouillon broth with your dinner. The use of yellow mustard also helps (the small amount of quinine in yellow mustard stops the cramping). If you have congestive heart failure, talk to your doctor about monitoring your salt intake in balance with your diuretic or water pill.
Hypoglycemia – If you read the ketogenic diet research, most of it was done on epileptic children. The diets called for a period of starvation, then the use of a ketogenic liquid based on the John’s Hopkin’s protocol. It is a well-known fact in medicine that starvation in children can frequently cause hypoglycemia, especially in children with other genetic or congenital defects leading to forms of epilepsy. In clinical practice, with ketogenic diet use in adults, hypoglycemia is rare.
Low Platelet Count (Thrombocytopenia) – Again, this was seen in the epileptic children who were placed into starvation first, then introduced a liquid fat replacement shake to stop intractable seizures. These liquids or shakes were often nutrient deficient in other essentials. Folic acid, B12 and copper deficiency can occur when not eating “real food.” Low platelet counts are rarely seen on ketogenic diets based around “real food.” Many children in the ketogenic studies had been on or were concomitantly on valproic acid for their seizures. Valproic acid is commonly known to cause thrombocytopenia (Barry-Kravis E et al, Bruising and the ketogenic diet: evidence for diet-induced changes in platelet function. Ann Neurol. 2001 Jan;49(1):98-103.; Kraut E, Easy Bruising, http://www.uptodate.com, May 2015.)
Easy Bruising – This is usually due to inadequate protein supplementation as was the case in much of the ketogenic literature where protein levels were also restricted. (Kraut E, Easy Bruising, http://www.uptodate.com, May 2015.)
Pancreatitis – Patients who are insulin resistant or have impaired fasting glucose commonly have high triglycerides. Elevation in triglycerides itself is a cause of pancreatitis. Ketogenic diets lower the triglycerides. However, if a patient has not been following their diet as directed, spikes in the triglycerides can occur placing the person at risk for pancreatitis.
Long QT Intervals/Heart Arrhythmias – The list of things causing Long QT intervals and abnormal heart rhythms is long and variable (Acquired Long QT Syndrome. Berul C et al. www.uptodate.com, May 2015). It is well know that starvation, rapid weight loss and liquid protein diets can cause a delay in the conduction signal in the heart. Anyone wishing to start any diet should have an electrocardiogram (EKG) through their doctor to ensure that the diet (of any type) doesn’t exacerbate a prolonged QT interval.
Three year weight loss and metabolic improvement in a patient on a Low-Carb / Ketogenic diet. Note: Patient admits to not following ketogenic diet during holidays from Nov 2013 – Feb 2014 (see the dramatic changes to the body when cheating happens)
Cardiomyopathy – Prolonged QT intervals have been associated with cardiomyopathy and the former can stimulate the later. Any diet that has the potential to prolong a QT interval has the potential to cause cardiomyopathy. Hence the need for regular EKG monitoring on any diet (Acquired Long QT Syndrome. Berul C et al. www.uptodate.com, May 2015).
Lipid/Cholesterol Changes – In the 8 years I have been applying ketogenic diets to patients, I have seen dramatic improvement in the triglycerides and HDL levels. The only time triglycerides rise over 100 is if the patient is using artificial sweeteners or is cheating on the carbohydrate restriction. Total cholesterol commonly rises, however, this is indicative of the fact that there is a shift in the LDL particle size and this affects the calculation of both total cholesterol and LDL-C. In light of this, most of my patients have dramatic improvement in triglycerides and small dense LDL particle number. I’ve included the common cholesterol changes I seen in my office as a few case reports to demonstrate the effectiveness of a ketogenic diet:
2 year ketogenic dietary labs and weight loss
Myocardial Infarction – It is interesting that one blogger includes this on the list of adverse reactions, however, when you actually read the study, the author of the paper make an “assumption” that there was potential for heart attack due to an elevated total cholesterol, however, a correlation was never made. Again, in the 8 years I have been using ketogenic diets, I have seen dramatic improvement in cholesterol profiles, inflammatory markers, atherosclerosis and carotid intimal studies (Shai I et al, Circulation 2010; 121:1200-1208).
Three year metabolic history of a Low-Carbohydrate / Ketogenic diet
Menstrual Irregularities / Amenorrhea – It is well known that any diet causing protein or other nutritional deficiency will affect the menstrual cycle first and growth second. The only time menstrual irregularities occur with a ketogenic or Low-Carb diet is when a patient is not taking in enough protein or is not eating real food. What amazes me is that a properly applied ketogenic diet causes normalization of the menstrual cycle, and in my practice, I’ve had a number of women successfully be able to conceive after making a ketogenic dietary change.
For more details on the nutrient content of a ketogenic diet, see the recent article by a friend of mine, Maria Emmerich. She’s been creating ketogenic diets for years and has a number of fantastic books my wife and I have been using in our home over the last nine years. She is one among many that can give you some direction on how to devise a healthy, real food based ketogenic diet. See the page on my website here that will give you some direction in formulating your Ketogenic Lifestyle.
Nally Family Low-Carb / Ketogenic Cheese Cake
So, to celebrate Mother’s Day, today, with my family, I am going to indulge in some Low-Carb / Ketogenic Cheese Cake!! Happy Mother’s Day, to all of you and especially to all you mothers out there making a healthy difference in the lives of your families! (You can find the recipe for this delicious cheese cake here)
In the words of Sir William Ostler, “If it were not for the great variability among individuals, medicine might well be a science and not an art.”
This post isn’t going to win me any friends . . . in fact, mentioning this topic a few days ago has already angered a number of them and resulted in an online tongue lashing by a few others. However, I can’t resist. And, based on some very persuasive data and personal experience, I don’t care.
Truth is truth . . . it doesn’t change no matter how you spin it, or attempt to fit it into your paradigm. The problem is what we have accepted in the last 40-50 years as “the scientific truth about getting healthy” is far from truth. By getting healthy, I’m implying the application of main-stream methods accepted to lose weight, reduce cholesterol, improve blood pressure and reduce your risk of heart disease and diabetes.
For the last 40 years we’ve been told that the only way to get and live healthy is to restrict our calories. This main-streamed advise continues even today in our USDA 2010 Dietary Guidelines. And, if you ascribe to this futile dogma propagated since the 1970’s, then you’ll know that the “only acceptable way” to do this is to “eat less fat” (because fat is the most caloric dense of the macro-nutrients, right?) and to “exercise more” (because that’s how we burn calories, right?!) Well, that’s what I thought, too. And that is the health prescription I doled out to my-self and to all of my patients for the first 8 years of my practice.
Interestingly, most of them, including myself, took that prescription of a caloric restricted diet of 1200-1500 calories per day and exercise 3-6 days a week for 30-60 minutes and ran with it. Personally, I restricted calories to 1200-1500 per day and began running triathlons. I performed cardiac monitored running, swimming and cycling for an hour a day during the week and 2 hours on the weekend. I lifted weights 2-3 days per week as well. Guess what it got me? Fat.
It raised my triglycerides by 100 points, elevated my LDL-C and increased my waistline by 3 inches. Yes, I gained weight. But, hey, my doctor was happy because my HDL-C went up by 4 points.
I saw this identical pattern with 3/4ths the patients in my office. A fourth of my patient’s (the group without any genetic insulin resistance) saw weight loss and improvement in their cholesterol profiles, but the rest didn’t. I had the exciting opportunity to introduce the saddened and discouraged 3/4ths of my patients to STATIN drugs and blood pressure medications. My average patient’s gained 2-3% of their body fat each year. Those that exercised like fiends were lucky if their weigh gain just stabilized.
What I saw in my office over a period of eight years was that exercise and caloric restriction didn’t work. But I couldn’t say that, because that goes against everything your 8th grade health teacher taught you. It contradicted your neighborhood dietitian, and it spat in the face of the food pyramid and the USDA Guidelines. The Government wrong? Never. . . . Speaking contradictory of the calorie-in/calorie-out exercise dogma was heresy, right? Contradict, Dr. Ornish, wouldn’t be heard of?!!
If I’ve learned one thing in my medical career, it is this: “Don’t be afraid to question everything” – even Dr. Dean Ornish, the USDA and the American Heart Association. And, fascinatingly, I’m not the only on that did.
——
——
Three Massive Studies did just that . . . question whether this exercise and caloric restriction dogma really works. This is what applying exercise and caloric cutting did for almost 67,000 people between 1972 and 2010 – little to nothing.
WHAT?!! Nothing?! You can’t be serous?
The first of these trials was the MRFIT (Multiple Risk Factor Intervention) Trial. It started in 1972, looking at 12,866 men with high risk for heart disease and followed them over seven years. All of them were placed on caloric restricted low fat diets and encouraged to exercise. It demonstrated that low fat diets and exercise FAILED to reduce weight or stop coronary artery disease in 100% of the cases. Don’t believe me? Read it for yourself (JAMA. 1982; 248 (12):1465-1477).
The second of these trials was the Women’s Health Initiative (WHI). This study started in 1991 and followed 48,835 women (yes, that’s a small city of women) for eight years. They didn’t believe the MRFIT results apparently, so they had a low fat (caloric restricted) arm and a control arm [the SAD diet (Standard American Diet)]. The women on the low fat arm lost a whooping 0.4 kg over the 8 year period (JAMA. 2006 Jan 4;295(1):39-49). 0.4 kg, really!?? That’s almost an entire pound of weight loss over 8 years. Quick, call Barnes & Noble so we can package that diet and sell it on Opra!! (Oh, wait, the news media was a little embarrassed by the findings and never really mentioned them.)
Lastly, if research on 60,000 men and women wasn’t enough to demonstrate what most primary care physicians seen in their offices daily, we had to do the Look AHEAD Study(Action for Health in Diabetes). This study started in 2001 and was supposed to run for 13.5 years. It studied 5,145 Type II diabetic patients with intensive lifestyle intervention. These patients were placed on intensive caloric and fat restriction of 1200-1800 calories per day with exercise and behavioral counseling. It was so unsuccessful, that they stopped the trial at 9.6 years – cause it wasn’t working.
The patients did lose some weight through Look AHEAD . . . an average of 6% of their body fat (That means you would have lost 15.6 lbs over 9 years if you weighed 260 lbs. Successful? . . . NOT). What made this trial worse is that it didn’t improve risk for coronary artery disease and people didn’t live longer (N Engl J Med 2013; 369:145-154). They just got the exciting chance to eat cardboard for 9 years of their lives. Sad. Very sad.
So, what does all this mean? Exercising your brains out at an expensive gym every morning won’t do much more than help you loose 1% of your body fat. It won’t increased your life span and it won’t decrease your risk of heart disease, despite what Dr. Ornish said. If you like spending $40 per month just to stare at sweaty fat bodies jumping up and down in spandex, by all means, please keep going to the gym. But I’d much rather spend that $40 on a nice rib eye steak at a restaurant staring at my wife. But, the benefits of saturated fat . . . that’s for another post.
Don’t get me wrong. I love lifting weights. I love riding my horse. I truly enjoy working in my yard. I even enjoy riding my bicycle. But I do these things now because they bring me peace, decrease my stress, and allow me to connect with nature. Believe me, there’s nothing natural about a 250 pound man in spandex staring at himself in a mirror repetitively lifting 30 pound bars of iron. But, we won’t go there.
My friends, and a few of my patients, get their knickers in a wad trying to decry the fact that I’m giving people a reason not to go running. Maybe I am. To be honest, there’s really only one reason I want to run, . . . and that’s when I’m being chased by a bear. But what good does it do to guilt a person into participation in an activity that isn’t really benefiting their health or help them lose weight, unless they really truly enjoy the activity for the sake of the activity?
Our health is not based upon a caloric scale of inputs and outputs. We are hormonal machines. We gain or lose weight and we gain or lose muscle based on powerful hormone signals, specifically insulin. Simple carbohydrate restriction has profound effects upon our weight, blood pressure, cholesterol and inflammatory states. Until we each come to grips with the fact that the food we eat triggers hormone responses in our bodies, we will continue down the path of diseases of civilization. Hippocrates summed it up when he said, “Let food be thy medicine, and let medicine be thy food.”
As a family practice physician and bariatrician, my job is to examine and treat the “Diseases of Civilization.” The Diseases of Civilization are those diseases arising out of the changes induced by industrializing and modernizing a society of people. These include diseases like diabetes, dyslipidemia (abnormal cholesterol), heart disease, hypertension, gout, vascular disease, & stroke. It is interesting that the so called Diseases of Civilization didn’t really appear on the scene until the early 1900’s. Yes, we have now identified some of these diseases in the early Egyptians, but to my point, as a society modernizes or industrializes, certain types of disease begin to arise. The Canadian cardiologist William Osler, one of the founding professors of John’s Hopkins Hospital, documented the first “syndrome” associated with narrowing of the arteries causing heart disease at the turn of the 19th century, and in 1912, the American Cardiologist James Herrick is credited with the discovery that narrowed arteries cause angina, a form of chest pain with exertion.
Today we know that underlying each of these diseases is the phenomenon of insulin over production, which seems to arise between five and twenty years prior to the onset of the Diseases of Civilization. Metabolic Syndrome, Dysmetabolic Syndrome or Syndrome X is the name we’ve given to the presentation of three or more of these diseases at once in one person. There is still argument as to whether insulin over production is the chicken or the egg, but what I see clinically has convinced me that insulin is culprit.
May 2013 Metabolism “Insulin Resistance: An adaptive mechanism . . .” 62(5):622-33. doi: 10.1016/j.metabol.2012.11.004. Epub 2012 Dec 20.
Insulin is a very powerful hormone that acts as a key, opening a door in just about every cell in the body, letting glucose (the primary form of fuel derived from carbohydrate) into the cell. For reasons that appear to be genetic, this key becomes “dull” in a portion of the population and does not unlock the door fast enough to lower the blood sugar. So, the body panics, and stimulates production of additional insulin, 2-10 times more in many people. However, the insulin that was produced initially, eventually kicks in. This extra insulin, acting at a slower rate, is the underlying culprit to the Diseases of Civilization.
How, you ask? Let me explain.
Insulin does more than just open the door for glucose.
1. Insulin causes weight gain. It turns on the storage of fat by activating an enzyme called lipoprotein lipase, pulling the triglycerides out of the cholesterol molecules and depositing them in the adipose tissue (fat cells).
2. Insulin raises cholesterol. It drives increased triglyceride production in the liver, especially in the presence of fructose.
3. Insulin triggers atherosclerosis. Triglycerides are essentially the passenger in the LDL (bad cholesterol) molecule. Higher triglycerides cause increased LDL production leading to increased atherosclerosis (narrowing of the arteries).
4. Insulin causes gout & kidney stones. Insulin increases uric acid production and in a round about way can increase calcium oxylate as well, increasing the risk of kidney stones and gout.
5. Insulin raises blood pressure. Insulin stimulates the retention of sodium, causing and increase in blood pressure.
Tiffini & Jazz riding near the top of the White Tank Mountains
6. Insulin makes inflammation worse. Insulin drives the inflammatory cascade and increases free radicals, and stimulates the inflammatory hormones causes arthritis, allergic rhinitis, psoriasis, dermatitis, and inflammatory bowel problems to be amplified.
My intent is not to demonize insulin. It is an essential hormone, however, when five to ten times the normal amount of insulin is being produced, you’re going to amplify the problems above by five to ten times normal. Type II Diabetes is really just a consequence of 15-20 years of over production of insulin.
This isn’t just something that affects humans. either. We have been seeing this in other species of the animal kingdom as well. Take for example my wife’s horse, Jazz. She’s a beautiful grey Arab/Saddle-Bred who kept having problems with laminitis, or more colloquially known as “founder.” Her diet consisted predominantly of alfalfa at the time, considered a moderate starch containing form of feed.
Laminitis is a progressively increasing tenderness to the hoof of horses or cattle that can be disabling and if not treated appropriately can cause permanent lameness in the animal. Recent literature in the veterinary world have identified that animal diets high in starch have a propensity to cause laminitis as well as colic. First identified in the equine community in the 1980’s with glucose tolerance tests, insulin resistance has been identified as a significant factor in hoof disease. The use of Corn, Oats, Barley or even Alfalfa as a primary form of feed for a horse with insulin resistance greatly increases the risk of laminitis.
Like Jazz, many horses in the arid Arizona climate are fed primarily with oats and alfalfa. Jazz was tested and found to have insulin resistance. Since Jazz has been placed on a much lower starch containing feed, she has had no further problems with laminitis. We converted all our horses to Bermuda grass.
Bailey, Jazz, Nayha & Houdini grazing in the back pasture
Our family and our horses are all now on Low-Carb diets to some degree and have been for the last seven years. No further hoof problems with the horses, and 55 lbs of weight loss with normalization of cholesterol in their owner, me.
Trail Riding in the White Tank Mountains
For those with interest, studies reveal feeds in order of the highest to lowest starch (carbohydrate) content to be: Sweet Feed, Corn, Oats, Barley, Wheat Bran, Beat Pulp, Alfalfa, Rice Bran, Soybean hulls, Bermuda Grass. Take a look the Low Carbohydrate help section in the menu above to see the carbohydrate content of many of the foods for human consumption.
It’s time we recognize that our diet and lifestyles have lead us to the Diseases of Civilization, and those diets and lifestyles have even effected our animals.
Weight loss, better put as “fat loss,” is a journey. A journey brought you to where you stand today, and it will be an even more exciting journey getting back to that size you’ve been daydreaming about. So, how do you most effectively start down the path of this journey? That is the great question. It is the most important question I get asked every day. In the words of Napoleon Hill, “Desire is the starting point of all achievement, not a hope, not a wish, but a keen pulsating desire which transcends everything.”
First, Know Where You Are Coming From. A journey requires knowing where you were, were you are today and where you want to go. Get a journal and weight yourself. Write it down and then check your weight every 3-5 days. DO NOT weigh yourself every day. I repeat DO NOT weight yourself every day. This can be discouraging because is is normal to fluctuate 2-5 lbs every day based on meals and water intake. Many people see this fluctuation and thing they are failing, then give up. The journal helps this. Recording your weight helps you see the progress.
The journal is also to help you record what you eat. Plan and record your meals IN YOUR JOURNAL. If you are being followed by a weight loss specialist, they will want to see your journal. If you are seeing me in my office, bring the journal with you to EVERY visit. Record every thing you eat. And, record your water intake. I am amazed at how many of my patient’s are dehydrated and just putting water back into their systems help them loose weight.
Second, Plan Your Day. Planning is the key to weight loss on any program. You should plan your exercise and plan your meals the night before. Failing to plan is really just planning to fail. Your plan should include 1) keeping carbohydrate intake less than 20 grams per day and 2) getting adequate proteins to match your goals.
Third, What’s the Underlying Cause of Your Weight Struggles?
You can’t effectively lose weight unless you understand why you are gaining weight. Two thirds of my patients are hyperinslinemic – they produce too much insulin in response to any sugar, starch or carbohydrate. This is also called “insulin resistance.” This is the primary cause of weight gain in 85% of the population. People produce between two to thirty times the normal amount of insulin in response to a piece of bread or a bowl of cereal. When they eat a single piece of bread, their bodies respond as if they ate the whole loaf. If they eat a bowl of cereal, their bodies respond as if they ate the whole box of Captain Crunch.
This variable over production of insulin is why some patient’s gain more weight than others eating and exercising the same way. Your doctor can easily identify this through blood work. For starters, if your waist circumference is larger than 40 inches as a male or larger than 35 inches as a female, you’re probably insulin resistant. Most men complain they don’t have a tape measure to measure their belly, so I tell them if they walk toward the wall and the first thing that touches the wall is their belly, “you’re insulin resistant.”
Skin Tags
Skin tags or the presence of thickened browning skin at areas of skin folds (acanthosis nigricans) are classic signs of insulin resistant.
Acanthosis Nigricans of the Neck-line
Hypoglycemia or low blood sugar is another sign of hyperinsulinemia or insulin resistance. This is where a person gets light headed or dizzy 2-5 hours after eating a meal that contains mainly starch or sugar.
Insulin resistance requires a dramatically different dietary approach than the standard diets we’ve been taught all our lives. The “heart healthy” diet, DASH diet, vegetarian/vegan diet, low fat diet or calorie restricted diet just don’t work with hyperinsulinemia or insulin resistance. If you are insulin resistant, a low fat/calorie restricted diet will not be very effective, and you may even gain weight with this approach as many of my patients have experienced.
If you have any of these symptoms, you need to follow up with your doctor or weight management specialist. Find out where your insulin levels are in relationship to your diet. Losing weight is possible. You can get started here with my ketogenic dietary program.
As this is a journey, it will probably have a number of twists and turns that are often made easier with a road map. Getting checked out with your doctor, and evaluating your metabolic status is your road map. Check out the health programs I offer to my patients to get this road map. I’ve also produced hundreds of videos on YouTube and DocMuscles.Locals.com to help you down the road. Either way, enjoy the journey!!

 After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the August 2004 Diabetes Care Journal screamed for my attention.
After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the August 2004 Diabetes Care Journal screamed for my attention.






























 Fat.
Fat.







 And, record your water intake. I am amazed at how many of my patient’s are dehydrated and just putting water back into their systems help them loose weight.
And, record your water intake. I am amazed at how many of my patient’s are dehydrated and just putting water back into their systems help them loose weight.

{kind=link}