Don’t miss this podcast as Dr. Nally discusses the sugar alcohol, erythritol, and what the Cleveland Clinic’s study really means to those following a Ketogenic Lifestyle. Is there another reason behind attacking erythritol?
Lock-boxes have always fascinated me. Lock-boxes with special keys are even more fascinating. The more I’ve learned about fat cells (adipocytes), the more I think about them as special fuel depositories or fat lock-boxes. Before the invention of refrigerators, fast-food, Bisquick and beer, our bodies preserved and reserved fat as a precious commodity.
The body, when given fat with carbohydrates or excess protein, quickly places the fat into a lock-box for safe keeping. It does this for two reasons. First, the body can store fat very efficiently. Second, hormone signals stimulate fat storage when other fuel sources (carbohydrate & protein) are present in excess. The body can access this stored fuel only when the right presentation of hormonal keys are present. Fascinatingly, we now know from recent research, there are actually three types of lock-boxes for fat in the human body (white adipose tissue, brown adipose tissue, and tan adipose tissue).
The greatest challenge for the obesity doctor is getting into the fat lock-box. Some people’s boxes are like the “Jack-in-the-Box” you had as a child – just add a little exercise spinning the handle and the box pops open (These are those people that say, “Oh, just eat less and exercise and you’ll lose weight.”) For the majority of the people I see, it’s more like the lock above with a four or five part key required to turn the gears just right. (And, that key often only seems available on a quarter moon at midnight when the temperature is 72 degrees.) Fat cells, called adipocytes, require four, and possibly more, keys to open them up and access the fuel inside. Exercise is only one of those keys. However, exercise alone often fails.
Over the last 18 months, I have been surprisingly impressed with the results patients have by the addition of both medium chain triglycerides and exogenous ketones. A number of people have asked me, “Why do you encourage the addition of exogenous ketones to a person already following a ketogenic diet?”
Others just accuse me of self promotion, saying, “You’re just trying to sell a product!”
Or they exclaim, “Giving more ketones is just a waste of time and money.”
A few of the uneducated holler from across cyberspace, “You’re just going to cause ketoacidosis!”
Believe me, I’ve heard it all. And, the skepticism is understandable. I work with people every day, looking closely at weight gain/loss, metabolism, cholesterol, blood pressure, inflammation, etc. With any “low-carb” or “ketogenic product,” I test it out on myself and my family, before I offer it to my patients or even consider encouraging its use in my practice. I have this desire to understand “the how” and “the why” before I prescribe the who and when.
The Fat Lock-Box Keys
First , let’s talk about the adipocyte as a fat lock-box – and where you find the keys. Then, we’ll discuss how products may or may not help.
Insulin
There is only one door INTO the adipocyte for the fat, and the key to that door is insulin. Insulin stimulates an enzyme called lipoprotein lipase that essentially pulls the fat from the cholesterol molecule into the fat cell. Without insulin, fat doesn’t enter the fat cell. As a result, type I diabetics (those that make absolutely no insulin) look anorexic if they don’t take their needed insulin. Insulin is also the first key to the back door on the adipocyte. Actually, if there is too much insulin in the system, fat enters easily through the front door but cannot exit the back door (Picture 1). Insulin seals up the back door so that fat cannot exit very effectively.
That’s why insulin is the master hormone when it comes to obesity. You’ve got to lower the over-all insulin load to get the adipocyte slowing fat entry and increasing fat exit. If you don’t do that, I don’t care how much you exercise, 85% of the population will struggle with weight loss. Hmmm, seems kind a familiar to the last 50 years of our obesity epidemic, No?
Picture 1 – Four Key Pathways to Adipocyte Stimulation of Lipolysis
Catecholamines
The second key to the back door of the fat cells are the catecholamines. These are adrenaline (epinephrine), norepinephrine, adrenocorticotropic hormone (ACTH) and even serotonin. These hormones are produced in the adrenal glands through exercise, fear and even recollection of powerful memories. Medications can also stimulate production of these hormones. The catecholamines stimulate cAMP. cAMP opens the fat cell, releasing fatty acids for fuel.
The thyroid hormone conversion of T4 to T3 also plays a role in uptake of the catecholamines by adnylyl cyclase (AC). Low levels of T3 (like those seen in hypothyroidism or in cases of thyroiditis) also inhibit unlocking of the fat lock-box. Conversion of T4 to T3 is driven by the presence of bile salts in the gut. Increase fat intake increases the presence of the bile salts which naturally leads to better T3 conversion. Hence my constant references to eating more fat and bacon. .
Inflammation & Medications
The third key is an inhibitory effect on adenylyl cyclase (AC) activity by alpha and beta adrenoreceptors, adenosine, prostaglandins, neuropeptide Y, peptide YY, HM74-R & nicotinic acid. These inhibitory and inflammatory hormones produced in the brain, gut and other areas decrease cAMP activity in the fat cell and slow fat loss. The fancy long names are all hormones causing inflammation. Of note, many are also stimulated by medications including blood pressure lowering drugs. Check with your doctor if the medications you are taking may be causing weight gain, or halting your weight loss.
Please note that the first three keys have effect on the cAMP pathway for release of fat from the adipocyte. These three keys turn on or off effective function of cAMP leading release of fatty acids from the fat cell.
Naturitic Peptides
The fourth key follows a separate pathway. This is why I’ve clinically seen patients experience weight loss even in the presence of higher insulin, inflammatory disease or hypothyroidism. This key activates release of the naturitic peptides (ANP, BNP). These hormones are released from the heart when it squeezes more powerfully. As the cardiac muscle contracts, it releases ANP & BNP hormones. These hormones stimulate the cGMP pathway in the adipocyte. It then activates hormone sensitive lipase (HSL) and perilipin to release free fatty acids. Again, this pathway is separate from the pathway by which the first three keys released fat. Exercise increases heart contractility, but is inhibited by high insulin levels. However, ketones themselves also stimulate this increased contractile effect.
There actually is a fifth key not referenced above. The fifth key to the fat lock-box amplifies testosterone’s presence through the HPG axis. Insulin resistance and leptin resistance lower testosterone in men and raise it in women, causing poly-cystic ovarian syndrome (PCOS). Normalizing insulin levels (with a ketogenic diet) while at the same time increasing ketones as the primary fuel powerfully resets the HPG axis through a complex series of hormonal reactions. Growth hormone is balanced and testosterone returns to a normal range.
Clinically, 60% of the people I see in the office have abnormal testosterone due to insulin resistance. This leads to hypogonadism in men and PCOS (abnormal periods, facial hair growth and/or infertility) in women. Restricting carbohydrates and maintaining nutritional ketosis by diet and/or addition of exogenous ketones has a powerful corrective factor in these people.
Testosterone influences the up-regulation of the alpha & beta adrenergic receptors (the 2nd & 3rd key above). Hence, if your testosterone is low, it has a suppression on the way that the catecholamines influence fatty acid release from the fat cells. If your testosterone and growth hormone are normal, muscle development and adrenaline stimulus from exercise helps amplify the use and mobilization of fat from the fat cell. In people with insulin resistance and leptin resistance, exercise and the catecholamines don’t have the same fat burning effect.
What Does This Actually Mean?
Yes, I have greatly simplified a series of very complex hormonal pathways in the explanation of the keys above. Why do you think understanding obesity has been so difficult? Think of your adipocytes as a fat lock-box.
What’s even more important is the knowledge that the fat cell DOES NOT open or close because of calories. There is no dogmatic calorie-meter on the wall of the fat cell. There is no calorie key to the fat lock-box. Really, . . . in the 50 years of studying fat, researchers haven’t found one. (Prove me wrong when you show me an electron micro-graph of a calorie-meter in the wall of a cell). Science has demonstrated multiple times that the lack of food from starvation or excessive fasting suppresses thyroid function (an inhibitory effect on key #3). Restricting calories actually inhibits fat loss in many people.
The fat lock-box keys I refer to above are hormone responses to the presence of macro-nutrients (food). That means, first reduce your carbohydrate intake by eating real food from good sources. You can learn how to get started by registering for my FREE six part weight loss mini-course. Second, be as active as you can. Third, reduce stress and medications that have inhibitory effect on catacholamines. Fourth, balance your thyroid. And, fifth, get into ketosis and consider adding exogenous ketones to your dietary regimen. It really is that simple.
References
(For those of you that still believe there is a calorie key – or just need something to do while in the bathroom):
Lafontan et al. Arterioscler Thromb Vasc Biol. 2005
I am a Family Practice Physician. I spent eleven years of my life training to become a physician certified in Family Medicine. But, I found this wasn’t enough. I struggled to treat the “diseases of civilization” that arise from society, our Western diet and lifestyle.
I, also, specialize in dietary weight/obesity management and low-carbohydrate/ketogenic diets. I actually spent an additional three years obtaining specialized training and board certification in this field. When you add all the training and my years of experience in practice together, I’ve spent over 25 years perfecting this art of medicine.
Because of this training, I have been very blessed that people from all over the world travel to Surprise, Arizona, to see me for weight management, dietary advise, and counseling on the diseases of civilization. I’ve been amazed that simple changes in diet halt and reverse obesity, arthritis, diabetes, cholesterol, high blood pressure, etc. The list goes on and on …
But I find a disturbing mindset pervasive through the community and the nation:
After listening to an number of people get angry over this issue in the last few weeks, I began wondering to myself…
Stomach Pain & Swelling with Hereditary Angio-Edema (HAE)
Listen to KetoTalk Podcast #32 where we talk about hereditary angio-edema, adequate ketone ranges, statin use while in ketosis and healthy keto questions. You can listen in by going to KetoTalk.com or you can listen in on iTunes.
“About 40 percent of my older patient population who take statins while eating ketogenic experience some form of myalgia they didn’t have before. And there’s an amplified side effect profile: muscle ache, joint pain, generalized fatigue, liver enzyme elevation, and cloudy headed.” — Dr. Adam Nally
KEY QUOTE: “Children are born in ketosis, so ketones are perfect for babies. The level of fat in breast-milk is essential for them to maintain their health and their growth.” — Dr. Adam Nally
Here’s are the 12 questions Jimmy and Adam answered in this special Keto Talk Mailbox Blitz extended podcast today:
– Testimonial from someone who learned his lesson why it’s important to stay ketogenic all the time
– Three-decade study confirms saturated fats are bad for health
– Is increased testosterone from a ketogenic diet a bad thing for women?
– Why am I still struggling with low energy and low ketones after months of being in ketosis?
– Can being in nutritional ketosis above 1.0 mmol cause painful headaches?
– Do artificial sweeteners and stevia raise insulin?
– Is my ketogenic diet causing me to cramp up before and during my half marathon racing?
– Is MCT oil a better fat to use on a ketogenic diet than other fats like coconut oil, cream, or butter?
– Why do I have a constant stomachache while I’m on a ketogenic diet?
– Do you have to be in ketosis to burn fat?
– Does being in ketosis lead to daily spotting and extended periods?
– Are ketones in my baby’s breastmilk safe for her to consume? And why did my milk supply drop when I went keto?
– What is the impact of the supplement creatine on ketones, blood sugar, and insulin levels?
– Can I ease into ketosis as a way to avoid the dreaded “keto flu?”
KEY QUOTE: “If you’re not feeling energy after that adaptation period of 2-4 weeks at the very most, then you’re doing something wrong. Let that be your wakeup call to change something.” — Jimmy Moore
Hypertension (elevated blood pressure) is one of the triad symptoms of metabolic syndrome. Most of the hypertension that I see clinically is driven by insulin resistance as the underlying cause. I see this problem in a very large majority of the people in my office and I am seeing people younger and younger show up with continually increasing blood pressure.
In medical school, we were taught to treat “borderline” or “slightly elevated blood pressure,” through “lifestyle changes” which was another way of saying exercise, caloric restriction & hold the salt. But most physicians today will tell you that exercise, salt & caloric restriction doesn’t work. When asked why the 34 year old male in my office suddenly has elevated blood pressure, the only explanation we had was it is a “genetic problem,” or “blood pressure naturally goes up as we get older,” or “you’ve been eating too much salt,” and they are started on blood pressure medication and sent on their way. But, as time went on, I found that I had to keep adding more and more blood pressure medication to control the continually rising blood pressure of the patients in my practice.
Most of these people will have a progressive elevation in blood pressure over time, and these blood pressure (anti-hypertensive) medications are/were continually raised until the person is on four or five different blood pressure pills at maximal doses. Again, when questioned why, their genetics are blamed and that is the end of it. Or is it?!
What shocked me was that when I took patients off of salt & caloric restriction, and placed them on low carbohydrate high fat diets (and yes, I gave them back their salt), their blood pressure normalized. I noticed that as their fasting insulin levels began to fall, their blood pressure began to return to normal.
What?! Blood pressure rise is caused by insulin?!
Ummm . . . Yes!
I am a prime example. During the first few years of my medical practice and reserve military service, we had routine vitals checkups. I was working out 3-5 days a week with weights and running 3-5 miles 2-3 times a week and restricting my calories to 1500 per day. So, I thought I was in pretty good shape. However, it was not uncommon for for the nurse to raise her eyebrows at my blood pressure readings in the 140-160 systolic and 85-98 range diastolic. “Oh, it’s the lack of sleep last night,” or “it’s the caffeine I had this morning,” would be my excuse. But I was making a lot of excuses, and in light of those excuses, my caloric restriction, exercise and salt restriction, I was also still gaining weight.
By the 5th year of my medical practice, I weighed 60 lbs heavier than I do today and I struggled to keep my blood pressure under 150/95. I was violating my own counsel . . . don’t trust a fat doctor for nutritional advise. (Or, was that advise from Dr.House?)
A much slimmer, healthier and happier Dr. Nally (center) in 2016
After cutting out the carbohydrates (I’ve kept my carbohydrate intake < 20 grams per day), moderating my protein intake and eating all the fat I am hungry for each day, my recent physical examination at the beginning of June 2016 revealed my blood pressure at 112/64. I don’t remember ever having blood pressure that low. And to be honest, I didn’t sleep well the night before my exam due to a number of middle of the night patient calls.
When I first started treating the insulin resistance problem in the human, rather than the blood pressure problem, I began to see immediate reductions in blood pressure within one to two weeks. So much of a reduction that if I didn’t warn the patient that they should begin to back down their blood pressure medications, they would experience symptoms of dizziness, light-headedness, headache and a few patient’s nearly passing out. On a low-carbohydrate, high-fat (ketogenic) diet you need salt (sodium, potassium, & magnesium). The process of burning fat as fuel causes you to lose increased amounts of sodium & potassium, and you have to replace these electrolytes. A number of my patients begin a low-carbohydrate, high-fat diet and are afraid of increasing their salt intake. Not replacing these electrolytes while on a ketogenic diet can also lead to low blood pressure, dehydrate and dizziness.
I often wondered why applying a ketogenic diet had such a profound effect on blood pressure so quickly. Dr. Robert Lustig helped answer that question for me.
In order to understand how the Standard American Diet (we call it the SAD diet in my office) raises your blood pressure, it is important to understand how the body processes the basic sugar molecule. Sugar is one glucose molecule bound to a fructose molecule. This is broken down in the body and 20% of the glucose is metabolized in the liver, the other 80% is sent on to be used as fuel throughout the body. Fructose, however, is where the problems arise. 100% of the fructose is metabolized in the liver, and the by product of fructose metabolism is increasing the liver’s production of MORE glucose and the byproduct of uric acid. Uric acid is produced and this inhibits the production of nitric oxide. The diminished nitric oxide in the presence of an increased level of glucose (stimulating increased insulin production due to eating starches) constricts the blood vessels and raises blood pressure. Yes, that donut you just ate raised your blood pressure for the next 12 hours.
The mechanism that fructose containing carbohydrates, sugars and starches raise blood pressure, cholesterol and cause weight gain can be seen in the really complex diagram found in Dr. Lustig’s 2010 article:
So, how do you lower your blood pressure through diet?
First, cut out all the simple sugars. These include anything with table sugar, high fructose corn syrup and corn syrup. (This is why people with any change in diet see some improvement in weight and blood pressure as they remove the simple sugars like candy, sugared drinks and pastries from their diet.)
Second, limit your overall intake of other sources of carbohydrates including any type of bread, rice, pasta, tortilla, potato, corn and carrots. Realize that carbohydrate in fruit is fructose, and when taken with other forms of glucose can have the same effect as table sugar – it can and will raise your blood pressure, as well as halt or cause weight gain.
Third, if you are taking blood pressure medications for hypertension, see your doctor about close monitoring of your blood pressure as it can and will drop within 2-4 weeks of making these dietary changes.
Maintaining ketosis is really important for weight loss and blood pressure or hypertension control. I am very much an advocate of using real food for this process, but I have also found that the use of exogenous ketone salts aid significantly in maintaining ketosis. I have found that exogenous ketones are the next step in bridging the difficulty of day to day maintenance of ketosis.
It isn’t making the mistakes that’s critical; it’s correcting them and getting on with the task that’s important. If you’ve been calorie restricting and exercising to lower you blood pressure, don’t fret. A simple change in your diet focused on restricting starches and carbohydrates has been demonstrated in my office to be more powerful than many of the blood pressure medications we’ve used for years.
Over the last few months, I’ve found myself amid the center of vehement nutritional arguments about fat, carbohydrates, calories and diet. I have found it fascinating that very intelligent men and women, over the last 50 years, have accepted, without reservation, a dogma taught them by their eighth grade nutrition teachers. This dogma is interlaced and interwoven throughout the textbooks, manuals, and college cafeterias throughout the world.
It is a well known fact, however, that hydrogen is the most common element in the universe and is used as a basic building block for most molecular structures. What many don’t realize is there exists another element yet to be added to the periodic table that is almost as prevalent called moronium (pending symbol approval – Mu). It fills the blank space on the table of elements between Hydrogen and Helium. I, and those who have been able to identify this element, suspect that moronium is a gas at room temperature and has some affinity to binding the white matter of the brain responsible for catechol-O-methyltransferase (COMT) gene regulation of the prefrontal cortex. It is suspected by some that when it is inhaled by a person of low intellect, it has only a mild effect. However, when combined with either oxygen (O), hydrogen (H) or Helium (He) and inhaled by those of higher intelligence, it has a much wider, more potent and even stupefying diffusion effect, that is quite surprising to witness.
Moronium reacts adversely when diffused into blood with a higher alcohol concentration and seems to spontaneously combust when it is exposed to old paper and libraries. Moronium is very difficult and very expensive to isolate. Moronium seems to be more prevalent during the summer and winter solstices, which may be why moronium intoxication seems to appear around holidays. Recent attempts in a nearby lab to synthetically create even small crystals of moronium cause an explosion, physically and psychologically stupefying all of the researchers involved and inducing them to leave the study of science and pursue individual careers as drummers.
The presence of moronium seems to be higher in those that do not read, or have an aversion to reading. There is some correlation that moronium drops in proportion to listening to iTunes podcasts, however, follow-up reading does appear to have a potential lowering affect on the moronium levels within the brain.
Why do I bring this up?
I suspect that this little known element may be responsible for intelligent men and women introducing questionable theoretical science as incontrovertible truth. Those with suppressed COMT regulation seem to have a propensity to accept theoretical science because it sounds good, even when there’s really no way to actually prove the theory at the time, or when colleagues have accepted the theory in a peer-pressure instead of peer-review situation.
The stupefying effect of moronium bound COMT produces dogma like:
Miasmatic Theory of Disease (A noxious poisonous vapor of air called miasma filled with decomposed particles of matter believed to be the cause of cholera and chlamydia or the Black Death)
The amazing thing about science is that it is self-correcting (at least it used to be). A scientist makes a set of observations about nature, and then identifies a plausible theory within the laws of nature to fit those observations. Then, researchers take that theory and test it in as many ways as possible, attempting to disprove the theory and isolate the cause of the observation. If the theory withstands scrutiny it becomes widely accepted.
At any given point in the future, if contradicting evidence emerges, the original theory is discarded and a new theory is then identified. In essence, this is the simple scientific method, however, in modern day application, it has become a great deal more messy than you’d think.
This approach (application of “the scientific method”) was skirted during the 1960’s and 1970’s regarding the “fat causes heart disease” theoretical proposition. Interestingly, there was also a notable increase in the number drummers and musicians during the 1980’s Hair Bands era. This begs the questions, which I wholly agree needs further study: Does moronium exist? and . . . . Did levels of moronium actually increase between 1960 and 1990 causing a surge in the presence and popularity of Hair Bands?
It only took us 20 years to get past the Era of the HairBands, hopefully we can turn the nutritional ship around and recognize the real culprit causing the Diseases of Civilization.
Ketosis in 60 minutes . . .
The Multi-Vitamin Dr. Nally Personally Uses
(Author’s Note: For those who may possibly be under the influence of moronium toxicity, the post above is written in sarcastic jest, and to be clear, there IS NOT an element currently under investigation called moronium!)
Ketogenic Lifestyle Rule #2: Life Begins at the Edge of Your Comfort Zone
We have been taught for over 50 years that the minimum carbohydrate intake necessary to maintain health is 130 grams per day, with the average diet of 2000 calories per day containing around 300 grams per day based on 1977 recommendations that 55-60% of are dietary intake should come from carbohydrates. This value was initially established during World War II by a committee of scientists tasked with determining dietary changes that might effect national defense (1). These “guidelines,” originally called the Recommended Daily Allowances (RDA) and accepted by many as the gospel truth, have been modified every ten years and in 1997 changed to the Dietary Reference Intake (DRI). However, the recommended carbohydrate values have not changed other than “avoiding added sugars” in the most recent 2015 recommendations.
In light of the fact that there are NO actual diseases caused by lack of carbohydrate intake, most dietitians and physicians still preach the carbohydrate dogma originally outlined by the RDA. I say dogma, because these recommendations are based on a diet that vilifies fat, particularly animal fat like red meat. Say the words “red meat” around a dietician these days you’d think Voldemort (“He Who Shall Not Be Named”) had returned.
I bring up the carbohydrate quandary because it is a question that I am asked every single day. The question that seems to be asked of me, more and more, is what exactly is a carbohydrate?
Let’s make it simple. There are really only three types of carbohydrates:
Sugar
Starch (known as complex carbohydrates)
Fiber
Let’s start with Sugar. The simple form of carbohydrates, and the form that spikes your blood sugar and insulin rapidly, are called mono-saccharides (glucose, galactose, fructose & xylose). When two of these mono-saccharides are bound together they form disaccharides like sucrose, also known as “table sugar” (glucose + fructose), lactose found in milk (glucose + galactose), and maltose found in cereals and sweet potatoes (glucose + glucose).
Milk Sugar or Lactose (glucose + glucose)
The simple monosaccharides or disaccharides are easy broken into their mono-saccharide form in the blood stream and require the body to produce insulin to be used. The person with insulin resistance, impaired fasting glucose or type II diabetes often produces 2-10 times the normal amount of insulin to correctly use these mono-saccharides (see why this is a problem in: The Dreaded Seven: Seven Detrimental Things Caused By High Insulin Levels). Remember, fruit is also simple sugar containing the mono-saccharide fructose . . . which we call “natures candy” in my office.
“Yea, I know sugar is bad for me, but Dr. Nally, I just eat the good starches.”
If I had a nickel for every time I’ve herd that phrase . . .
We’ve become comfortable with shunning fat and “simple sugar,” but in the process we’ve been eating more “good starch.” But the “good starches” are also saccharides – just in longer chains of more than three glucose molecules bound together. Our gut easily breaks the bonds between the glucose links and turns these starches into mono-saccharides to be used as fuel. It takes a bit longer than the simple sugars above, so the release of insulin is slower (which is why it has a better glycemic index score), but whether you produce the insulin in the first hour or the second hour after eating it, insulin is still insulin. In the case of insulin resistance, the damage is still done.
These good starches make up “comfort food” like bread, rice, pasta, potatoes, corn, grains & oats. To the patient with insulin resistance, impaired fasting glucose or type II diabetes, the higher insulin response stimulates increased weight gain, rise in cholesterol, shift in hormone function and progression of atherosclerosis (vascular and heart disease). See the recent article on Why Your Oatmeal is Killing Your Libedo.
What about “resistance starches?” These are still starches and I am finding clinically that they still cause a rise in insulin and push people out of ketosis (See Common Ketosis Killers).
Finally, Fiber. Fiber is a carbohydrate, however, it is the indigestible part of the plant. Fiber has double bonds between the saccharides that human gastrointestinal tracts cannot digest. In most cases, fiber passes right through the intestines without being digested. It actually acts like a broom for your colon, helping the intestines to move nutrients through the system. This is why I recommend 1-2 leafy green salads a day for most patient’s following ketogenic diet. Fiber does help to promote bowel function.
The Leafy Greens
Fruit, non-green vegetables, pasta, grains and breads do contain good sources of fiber, however, these foods also have absorbable starches making them problematic as noted above.
The take home message is this, the use of starch or simple carbohydrate will be problematic for weight loss, cholesterol control, blood sugar control or blood pressure control in a patient with insulin resistance.
Therefore, the ketogenic lifestyle truly begins at the end of your comfort zone.
I thought that over the next few weeks I’d address a number of Ketogenic Lifestyle Rules that I have adopted. These seem to help and bring a little clarity to one following a Ketogenic Lifestyle or someone on the road to becoming a true “Ketonian.”
The first of these rules is that there should ALWAYS be bacon in the fridge!
We address this rule and some interesting facts around having bacon in the fridge in this evening’s Persicope below. We also address the benefits of journaling, how to help stop binge eating, what are your real protein needs, and red-meat fear-mongering. We even discuss whether or not pigs like bacon. Enjoy!
(Just a note: I love Katch.me’s service; however, due to the contract language allowing Katch.me to have unlimited rights to my Periscope Videos, I have withdrawn from Katch and my videos are no longer available on this medium until the contract usage can be modified.)
Join Dr. Nally on this evening’s Periscope as we talk about your biggest weight loss struggles in rapid fire style. We cover topics this evening from the effects of cheating on a ketogenic diet to how to overcome a weight loss stall . . . join us to hear the whole conversation.
I’ve been looking for the answer for quite some time. . . what role does caffeine play in your and my weight management journey? The answer gave me a headache. . . literally and figuratively.
As many of you, including my office staff, know, I love my Diet Dr. Pepper (and my bacon). I found that being able to sip on a little soda throughout the day significantly helped the carbohydrate cravings and munchies during a busy and stressful day at the office. Diet Dr. Pepper contains caffeine, however, I wasn’t really worried. Caffeine has been well know to have a thermogenic effect which increases your metabolism and has been thought for many years to help with weight loss among the weight loss community.
Diet Dr. Pepper is, also, one of only four diet sodas on the grocery store shelves that doesn’t contain acesulfame potassium (click here to see why most artificial sweeteners cause weight gain). The four diet sodas that I have been comfortable with my patients using are Diet Dr. Pepper, Diet Coke, Diet Mug Root-beer and Diet A&W Cream Soda. These are the last four hold out diet sodas that still use NutraSweet (aspartame) as the sweetener. Most of the soda companies have switched the sweetener in their diet sodas to the insulinogenic acesulfame potassium because it tastes more natural and aspartame has been given a media black eye of late. However, NutraSweet (aspartame) is the only sweetener that doesn’t spike your insulin or raise blood sugar (click here to find out why that is important).
Yes, I know. The ingestion of 600 times the approved amount of aspartame causes blindness in lab rats (but we’re not lab rats, and . . . have you ever met someone that drinks 600 Diet Dr. Peppers in a day? The lethal dose of bananas, which are high in potassium that will stop your heart, is 400). Aspartame can also exacerbate headaches in some (about 5% of people) and I’ve had a few patients with amplified fibromyalgia symptoms when they use aspartame. But for most of us, its a useful sweetener that doesn’t spike your insulin response, halting or causing weight gain.
But, over the last few years, I’ve noticed that increased amounts of Diet Dr. Pepper & Diet Coke seem to cause plateauing of weight and decreasing the ability to shift into ketosis, especially mine. I’ve also noticed (in my personal n=1 experimentation) that my ability to fast after using caffeine regularly seems to be less tolerable, causing headaches and fatigue 8-10 hours into the fast, symptoms that don’t seem to let up until eating. Through the process of elimination, caffeine seems to be the culprit.
After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the August 2004 Diabetes Care Journal screamed for my attention.
It appears that caffeine actually stimulates a glucose and insulin response through a secondary mechanism. The insulin surge and glucose response is dramatically amplified in patients who are insulin resistant. Caffeine doesn’t effect glucose or insulin if taken while fasting; however, when taken with a meal, glucose responses are 21% higher than normal, and insulin responses are 48% higher in the insulin resistant patient. Caffeine seems to only effect the postprandial (2 hours after a meal) glucose and insulin levels. The literature shows mixed responses in patients when caffeine is in coffee or tea, probably due to the effect of other organic compounds (1).
Caffeine effect on plasma glucose and plasma insulin compared to placebo (1).
Caffeine also diminishes insulin sensitivity and impairs glucose tolerance in normal and already insulin resistant and/or obese patients. This is seen most prominently in patients with diabetes mellitus type II (stage IV insulin resistance). Caffeine causes alterations in glucose homeostasis by decreasing glucose uptake into skeletal muscle, thereby causing elevations in blood glucose concentration and causing an insulin release (2-6).
Studies show that caffeine causes a five fold increase in epinephrine and a smaller, but significant, norepinephrine release. The diminished insulin sensitivity and exaggerated insulin response appears to be mediated by a catacholamine (epinephrine, norepinephrine & dopamine) induced stress response (5). Caffeine has a half life of about 6 hours, that means the caffeine in your system could cause a catacholamine response for up to 72 hours depending upon the amount of caffeine you ingest (7).
The reason for my, and other patient’s, headaches and fatigue after a short fast was due to the exaggerated stress hormone response. Increased levels of insulin were induced by a catacholamine cascade after caffeine ingestion with a meal, dramatically more amplified in a person like me with insulin resistance. The caffeine with the last meal cause hypoglycemia 5-7 hours into the fasting, leading to headaches and fatigue that are only alleviated by eating.
Even when not fasting, the caffeine induced catacholamine cascade causes up to 48% more insulin release with a meal, halting weight loss and in some cases, causing weight gain.
Caffeine is not the “Wonder-Boy” we thought it was.
How much caffeine will cause these symptoms? 50 mg or more per day can have these effects.
10,000 mg (10 grams) – lethal dose (Yes, 25 cups of Starbucks Coffee can kill you)
The equivalent of 100 mg of in a human was given to a spider, you can see the very interesting effect on productivity. How often does the productivity of the day feel like the image below?
Normal Spider (9)Spider on caffeine (9)
Beware that caffeine is now being added to a number of skin care products including wrinkle creams and makeup. Yes, caffeine is absorbed through the skin, so check the ingredients on your skin care products.
Diet Dr. Pepper, my caffeine delivery system of choice, has slightly less caffeine (39 mg per 12 oz can or 3.25 mg per oz) than regular Dr. Pepper. I found myself drinking 2-3 liters of Diet Dr. Pepper per day (long 16-18 hour work days in the office). After doing my research, I realized that my caffeine tolerance had built up to quite a significant level (230-350 grams per day).
So, a few weeks ago, I quit . . . cold turkey.
Did I mention the 15 withdrawal symptoms of caffeine? (8)
Headache – behind the eyes to the back of the head
Sleepiness – can’t keep your eyes open kind of sleepiness
Irritability – everyone around you thinks you’ve become a bear
Lethargy – feels like your wearing a 70 lb lead vest
Constipation – do I really need to explain this one?
Depression – you may actually feel like giving up on life
Muscle Pain, Stiffness, Cramping – feel like you were run over by a train
Lack of Concentration – don’t plan on studying, doing your taxes or performing brain surgery during this period
Flu Like Illness – sinus pressure and stuffiness that just won’t clear
Insomnia – you feel sleepy, but you can’t sleep
Nausea & Vomiting – You may loose your appetite
Anxiety – amplified panic attacks or feeling like the sky is falling
Brain Fog – can’t hold coherent thoughts or difficulty with common tasks
I experienced 13 of the 15 that lasted for 4 days. I do not recommend quitting cold turkey unless you have a week off and someone to hold your hand, cook your meals and dose your Tylenol or Motrin. My wife thought I was dying. . . I thought I was dying on day two. I actually had a nightmare about buying and getting into my own coffin. It can take up to three weeks to completely recover from caffeine withdrawal.
The other way to quit is to decrease your caffeine intake by 50 mg every two days. That means decrease caffeine by:
1 can of soda every two days
1/4 cup of coffee every day
1/2 can of Energy Drinks every two days
1 cup of tea every two days
The benefit of this method is that withdrawal symptoms are much less severe without the caffeine headache and the ability to remain productive. It will take longer, but quitting cold turkey is not a pretty picture. Been there . . . done that, . . . and I’m not going back. I actually lost another half inch off my waistline by day 5 of caffeine discontinuation.
What is the take home message here? If you have any degree of insulin resistance, caffeine makes it worse and will amplify your weight gain as well as decrease the productivity of your day.
How do you know if you're insulin resistant? What questions need to be asked? What should your numbers be? And, many other great ketosis questions. Also, why does Dr. Nally look like he has dirt on his chin? See it here . . .
Adrenal Fatigue? Adrenal Insufficiency? Cortisol? PseudoCushing’s Syndrome? What do these terms mean and why are they all over the internet these days? And, what do they have to do with your weight loss?
This was our topic this evening on PeriScope. Katch Dr. Nally speak about this topic with rolling comments at Katch.me/docmuscles. Or you can watch the video below:
If you’re not sure about what this is, you’re not alone. I think I’ve heard the term “Adrenal Fatigue” at lease four times a day for the last three months. If you ask your doctor, they’ll probably scratch their heads too. The funny thing is that “Adrenal Fatigue” isn’t a real diagnosis, but it is all over the internet and it shows up in the titles of magazines in the grocery store every day. There’s even and “Adrenal Fatigue For Dummies” so it must be real, right?!
No. It isn’t a real diagnosis. It is a conglomeration of symptoms including fatigue, difficulty getting out of bed in the morning, and “brain fog” that have been lumped together to sell an “adrenal supplement.” (Sorry, but that’s really what it is all about.) Do a Google search and the first five or six sites describing adrenal fatigue claim the solution is taking their “special adrenal supplement.”
I know what you’re thinking, “Your just a main stream, Western Medicine doctor, Dr. Nally, you wouldn’t understand.” Actually, I do understand.
Adrenal fatigue has risen in popularity as a “lay diagnosis” because many patients show up at their doctors office with significant symptoms that actually interfere with their ability to function, and after all the testing comes back negative for any significant illness, they are told that they are normal. But the patient still has the symptoms and no answer or treatment has been offered. It’s discouraging. . . very discouraging.
That’s because the symptoms are actually the body’s response to chronic long term stress. Many of my patients, myself included, have found themselves “stuck” in their weight loss progression, feeling fatigued, struggling to face the day, with a number of symptoms including cold intolerance, memory decline, difficulty concentrating, depression, anxiety, dry skin, hair loss, and even infertility in some cases. Is it poor functioning adrenal glands? No, your feeling this way because the adrenal glands are actually doing their job!!
If the adrenal glands weren’t working you’d experience darkening of the skin, weight loss, gastric distress, significant weakness, anorexia, low blood pressure, and low blood sugar. The symptoms are actually called Addison’s disease and it is actually fairly rare (1 in 100,000 chance to be exact). So what is causing the symptoms you ask?
There are a number of reasons, but one that I am seeing more and more frequently is “Pseudo-Cushings’s Syndrome.” Pseudo-Cushing’s Syndrome is a physiologic hypercortisolism (over production of cortisol) that can be caused by five common issues:
Chronic Physical Stress
Severe Bacterial or Fungal Infections that Go Untreated
Malnutrition or Intense Chronic Exercise
Psychological Stress – including untreated or under-treated depression, anxiety, post-traumatic stress, or dysthymia (chronic melancholy)
Alcoholism
The psychiatric literature suggest that up to 80% of people with depressive disorders have increased cortisol secretion (1,2,3). People with significant stressors in their life have been show to have an increased corsiol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing a daily, cyclic over production of cortisol and then normalization of cortisol after resolution of the stressor. This cortisol response is not high enough to lead to a true Cushing’s Syndrome, but has the effect of the symptoms listed above and begins with limiting ones ability to loose weight.
I’m convinced that this is becoming more and more prevalent due to the high paced, high-stress, always on, plugged in, 24 hour information overload lives we live.
What is cortisol? It is a steroid hormone made naturally in the body by the adrenal cortex (outer portion of the adrenal gland). Cortisol is normally stimulated by a number of daily activities including fasting, awakening from sleep, exercise, and normal stresses upon the body. Cortisol release into the blood stream is highest in the morning, helping to wake us up, and tapers into the afternoon. Cortisol plays a very important role in helping our bodies to regulate the correct type (carbohydrate, fat, or protein) and amount of fuel to meet the bodies physiologic demands that are placed upon it at a given time (4,5,6).
Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids or proteins into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues (by stimulating insulin production) and turns on the maturation process of adipocytes (it makes your fat cells age – nothing like having old fat cells, right?!) In the process, cortisol suppresses the immune system through an inhibitory effect designed to decrease inflammation during times of stress (7,8,9). If this was only occurring once in a while, this cascade of hormones acts as an important process. However, when cortisol production is chronically turned up, it leads to abnormal deposition of fat (weight gain), increased risk of infection, impotence, abnormal blood sugars, brain fog, head
aches, hypertension, depression, anxiety, hair loss, dry skin and ankle edema, to name a few.
The chronic elevation in cortisol directly stimulates increased insulin formation by increasing the production of glucose in the body, and cortisol actually blunts or block-aids the thyroid function axis. Both of these actions halt the ability to loose weight, and drive weight gain.
Cortisol also increases appetite (10). That’s why many people get significant food cravings when they are under stress (“stress eaters”). Cortisol also indirectly affects the other neuro-hormones of the brain including CRH (corticotrophin releasing hormone), leptin, and neuropeptide Y (NPY). High levels of NPY and CRH and reduced levels of leptin have also been shown to stimulate appetite and cause weight gain (10-11).
How do you test for Pseudo-Cushing’s Syndrome?
Testing can be done by your doctor with a simple morning blood test for cortisol. If your cortisol is found to be elevated, it needs to be repeated with an additional 24 hour urine cortisol measurement to confirm the diagnosis. If Cushing’s Syndrome is suspected, some additional blood testing and diagnostic imaging will be necessary. Pseudo-Cushing syndrome will demonstrate a slightly elevated morning cortisol that doesn’t meet the criteria for true Cushing’s type syndrome or disease.
How do you treat it?
First, the stressor must be identified and removed. Are you getting enough sleep? Is there an underlying infection? Is there untreated anxiety or depression present? Are you over-exercising? These things must be addressed.
Second, underlying depression or anxiety can be treated with counseling, a variety of weight neutral anti-depressant medications or a combination of both. Many of my patients find that meditation, prayer, and journaling are tremendous helps to overcoming much of the anxiety and depression they experience.
Third, adequate sleep is essential. Remove the television, computer, cell phone, iPad or other electronic distraction from the bedroom. Go to bed at the same time and get up at the same time each day. Give yourself time each day away from being plugged in, logged in or on-line.
Fourth, mild intensity (40% of your maximal exertion level) exercise 2-3 days a week was found to lower cortisol; however, moderate intensity (60% of your maximal exertion level) to high intensity (80% of your maximal exertion level) exercise was found to raise it (12). A simple 20 minute walk, 2-3 times per week is very effective. Find a hobby that you enjoy and participate in it once or twice a week. Preferably, a hobby that requires some physical activity. The activity will actually help the sleep wake cycles to improve.
Fifth, follow a low carbohydrate or ketogenic diet. Ketogenic diets decrease insulin and reverse the effect of long term cortisol production. Ketogenic diets a have also been shown to decrease or mitigate inflammation by reducing hyperinsulinemia commonly present in these patients (13).
So, the take home message is . . . take your adrenal glands off of overdrive.
References:
Pfohl B, Sherman B, Schlechte J, Winokur G. Differences in plasma ACTH and cortisol between depressed patients and normal controls. Biol Psychiatry 1985; 20:1055.
Pfohl B, Sherman B, Schlechte J, Stone R. Pituitary-adrenal axis rhythm disturbances in psychiatric depression. Arch Gen Psychiatry 1985; 42:897.
Gold PW, Loriaux DL, Roy A, et al. Responses to corticotropin-releasing hormone in the hypercortisolism of depression and Cushing’s disease. Pathophysiologic and diagnostic implications. N Engl J Med 1986; 314:1329.
Ely, D.L. Organization of cardiovascular and neurohumoral responses to stress: implications for health and disease. Annals of the New York Academy of Sciences (Reprinted from Stress) 771:594-608, 1995.
McEwen, B.S. The brain as a target of endocrine hormones. In Neuroendocrinology. Krieger and Hughs, Eds.: 33-42. Sinauer Association, Inc., Massachusetts, 1980.
Vicennati, V., L. Ceroni, L. Gagliardi, et al. Response of the hypothalamic- pituitary-adrenocortical axis to high-protein/fat and high carbohydrate meals in women with different obesity phenotypes. The Journal of Clinical Endocrinology and Metabolism 87(8) 3984-3988, 2002.
Wallerius, S., R. Rosmond, T. Ljung, et al. Rise in morning saliva cortisol is associated with abdominal obesity in men: a preliminary report. Journal of Endocrinology Investigation 26: 616-619, 2003.
Epel, E.S., B. McEwen, T. Seeman, et al. Stress and body shape: stress-induced cortisol secretion is consistently greater among women with central fat.
Psychosomatic Medicine 62:623-632, 2000.
Tomlinson, J.W. & P.M. Stewart. The functional consequences of 11_- hydroxysteroid dehydrogenase expression in adipose tissue. Hormone and Metabolism Research 34: 746-751, 2002.
Epel, E., R. Lapidus, B. McEwen, et al. Stress may add bite to appetite in women: a laboratory study of stress-induced cortisol and eating behavior.Psychoneuroendocrinology 26: 37-49, 2001.
Cavagnini, F., M. Croci, P. Putignano, et al. Glucocorticoids and neuroendocrine function. International Journal of Obesity 24: S77-S79, 2000.
Hill EE, Zack E, Battaglini C, Viru M, Vuru A, Hackney AC. Exercise and circulating cortisol levels: the intensity threshold effect. J Endocrinol Invest. 2008. Jul;31(7):587-91.
Fishel MA et al., Hyperinsulinemia Provokes Synchronous Increases in Central Inflammation and β-Amyloid in Normal Adults. Arch Neurol. 2005;62(10):1539-1544. doi:10.1001/archneur.62.10.noc50112.
What laboratory testing is necessary when you start your weight loss journey on a Ketogenic, Low-Carbohydrate, Paleolithic or any other dietary changes? Why do you need them and what are you looking for? We discuss these questions and others on today’s PeriScope. Lots of questions from around the world to day . . . this one lasted a bit longer than normal . . . 45 minutes to be specific. But it’s a good one because of all of your fantastic questions! You really don’t want to miss this one.
You can see the video below or watch the video combined with the rolling comments here on Katch.me/docmuscles.
A list of the labs that we discussed are listed below:
Fasting insulin with 100 gram 2 or 3 hour glucose tolerance test with insulin assay every hour
CMP
CBC
HbA1c
Leptin
Adiponectin
C-Peptid
NMR Liprofile or Cardio IQ test
Lipid Panel
Urinalysis
Microalbumin
Apo B
C-reactive protein
TSH
Thyroid panel
Thyroid antibodies
AM Cortisol
This list will at least get one started, provide the screening necessary to identify insulin resistance (Diabetes In-Situ), Impaired fasting glucose, diabetes and allow for screening for a number of the less common causes of obesity.
I would highly recommend that you get these through your physician’s office so that appropriate follow up can be completed. These labs will need to be interpreted by your physician, someone who understands and is familiar with various causes of obesity.
I just completed my reading of Dr. Joseph Kraft’s Diabetes Epidemic & You. This text originally printed in 2008 and was re-published in 2011. I am not really sure why I have never seen this book until now, but I could not put it down. I know, I am a real life medical geek. But seriously, you should only read this book if you are concerned about your health in the future. Otherwise, don’t read it.
For the first time in 15 years, someone has published and validated what I have been seeing clinically in my office throughout my career. Dr. Kraft is a pathologist that began measuring both glucose and insulin levels through a three hour glucose tolerance blood test at the University of Illinois, St. Joseph Hospital in Chicago. This test consists of checking blood sugar and insulin in a fasted state, and then drinking a 100 gram glucose load followed by checking blood sugar and insulin at the 30, 60, 120 and 180 minute marks (a total of three hours).
Dr. Kraft completed and recorded this test over a period of almost 30 years on 14,384 patients between 1972 and 1998. His findings are landmark and both confirm and clarify the results that I have seen and suspected for years.
I am convinced that our problem with treating obesity, diabetes and the diseases of civilization has been that we defined diabetes as a “disease” based on a lab value and a threshold instead of identifying the underlying disease process. We have been treating the symptoms of the late stage of a disease that started 15 to 20 years before it is ever actually diagnosed. Diabetes is defined as two fasting BS >126, any random blood sugar >200, or a HbA1c >6.5%. (Interestingly this “disease” has been a moving target. When I graduated from medical school it was two fasting blood sugars >140 and the test called hemoglobin A1c (HbA1c) that we use today for diagnosis didn’t even exist). The semantics associated with this problem is that many of us recognize that the disease is not actually diabetes. The disease is (as far as we understand it today) insulin resistance or hyperinsulinemia. This is where Dr. Kraft’s data is so useful. Diabetes, as it is defined above, is really the fourth stage of insulin resistance progression over a 15-20 year period and Dr. Kraft’s data presents enormous and very clear evidence to that effect.
When I first entered private practice 15 years ago, I noticed a correlation and a very scary trend that patients would present with symptoms including elevated triglycerides, elevated fasting blood sugar, neuropathy, microalbuminuria, gout, kidney stones, polycystic ovarian disease, coronary artery disease and hypertension that were frequently associated with diabetes 5-15 years before I ever made the diagnosis of diabetes mellitus. I began doing 2 hour glucose tolerance tests with insulin levels and was shocked to find that 80-85% of those people were actually diabetic or very near diabetic in their numbers. The problem with a 2 hour glucose tolerance test, is that if you are diabetic or pre-diabetic, you feel miserable due to the very profound insulin spike that occurs. A few patients actually got quite upset with me for ordering the test, both because of how they felt after the test, and the fact that I was the only physician in town ordering it. So, in an attempt to find an easier way, I found that the use of fasting insulin > 5 nU/dl, triglycerides > 100 mg/dl and small dense LDL particle number > 500 correlated quite closely clinically with those patients that had positive glucose tolerance tests in my office. There is absolutely no data in the literature about the use of this triangulation, but I found it to be consistent clinically.
I was ecstatic to see that Dr. Kraft plowed through 30 years and over 14,000 patients with an unpleasant glucose tolerance test and provided the data that many of us have had to clinically triangulate. (I’m a conservative straight white male, but if Dr. Kraft would have been sitting next to me when I finished the book this afternoon, I was so excited that I probably would have kissed him.)
Insulin resistance or hyperinsulinemia (the over production of insulin between 2-10 times the normal amount after eating carbohydrates) is defined as a “syndrome” not a disease. What Dr. Kraft points out so clearly is that huge spikes in insulin occur at 1-2 hours after ingestion of carbohydrates 15-20 years prior to blood sugar levels falling into the “diabetic range.” He also demonstrates, consistently, the pattern that occurs in the normal non-insulin resistant patient and in each stage of insulin resistance progression.
The information extrapolated from Dr. Kraft’s research give the following stages:
Stages of insulin resistance by 3 hr OGTT extrapolated from “Diabetes Epidemic & You”
From the table above, you can see that the current definition of diabetes is actually the fourth and most prolifically damaging stage of diabetes. From the data gathered in Dr. Kraft’s population, it is apparent that hyperinsulinemia (insulin resistance) is really the underlying disease and that diabetes mellitus type II should be based upon an insulin assay instead of an arbitrary blood sugar number. This would allow us to catch and treat diabetes 10-15 years prior to it’s becoming a problem. In looking at the percentages of these 14,384 patient, Dr. Kraft’s data also implies that 50-85% of people in the US are hyperinsuliemic, or have diabetes mellitus “in-situ” (1). This means that up to 85% of the population in the U.S. is in the early stages of diabetes and is the reason 2050 projections state that 1 in 3 Americans will be diabetic by 2050 (2).
Insulin resistance is a genetically inherited syndrome, and as demonstrated by the data above has a pattern to its progression. It is my professional opinion that this “syndrome” was, and actually is, the protective genetic mechanism that protected groups of people and kept them alive during famine or harsh winter when no other method of food preservation was available. It is most likely what kept the Pima Indians of Arizona, and other similar groups, alive while living for hundreds of years in the arid desert. This syndrome didn’t become an issue among these populations until we introduced them to Bisquick and Beer.
The very fascinating and notably exciting aspect of this whole issue is that insulin resistance is made worse by diet and it is completely treatable with diet. This is where the low carbohydrate diet, and even more effective ketogenic diet or lifestyle becomes the powerful tool available. Simple carbohydrate restriction reverses the insulin spiking and response. In fact, I witness clinical improvement in the insulin resistance in patients in my office over 18-24 months every day. You can get a copy of my Ketogenic Diet here in addition to video based low carbohydrate dietary instruction.
Until we are all on the same page and acknowledge that diabetes is really the fourth stage of progression on the insulin resistance slippery slope, confusion and arguments about treatment approaches will continue to be ineffective in reducing the diseases of civilization.
It is well know that one of the most profound complications of diabetes is damage to the kidney and the very small arteries within the kidney acting as your body’s filtration system. The kidney begins to lose the ability to adequately filter and retain microscopic protein progressively over time. As the blood sugar and insulin levels continually rise over time in the patient with diabetes or pre-diabetes, damage to the delicate filtering system of the kidneys occur. This very common and progressively damaging problem is called “nephropathy.”
Chronic elevated blood sugar and insulin cause the filtering system to become more and more “leaky” and ineffective.
We knew in 1972 that patients with diabetes had thickening of the basement membrane or endothelium of the small tubles within the kidneys. In fact, 98.6% of diabetics tested had thickening of this area of endothelium and tubules also called the renal glomeruli (1). This allows the glomerulus or filtration system of the kidney to become more “leaky” and microscopic protein loss begins to occur through the kidney. This loss of important proteins in the blood is called “albuminuria” or “micro-albuminuria.” It is a flag that further damage of the kidney can and will occur without making significant changes to lower the blood sugar and the insulin. As of today, it is not totally clear how the basement membrane is damaged at the microscopic level, however, there is some evidence that elevated insulin has both a physical and immune type effect that stimulates oxidative stress, atherogenesis, immunoglobulins, as well as the formation advanced glycation end products leading to endothelial wall damage (2).
Recent research reveals that a ketogenic diet effectively repairs and/or completely reverses the albuminuria (3).
Evidence in my office of the significant improvement in micro-albumin can be seen in the one of a number of case studies below:
72 year old male with history of diabetes, diabetic nephropathy already treated with full dose statins, ACE inhibtors, metformin, and Januvia. (Remember, microalbumin should be <30 mg/g)
Date Microalbumin HbA1c
8/12/2010 2264 mg/g 6.4% Started carb restriction <30 g per day.
10/01/2010 1274 mg/g 5.2%
1/08/2011 1198 5.8% Admits to cheating over holidays
12/26/2013 2434 mg/g 6.8% Returned from 2 yr travel-off diet
2/27/2014 399 mg/g 6.3% Restarted carb restriction <20g per day
6/20/2014 190 mg/g 7.0% Traveling – no carb restriction
The patient began following a ketogenic diet in 2010. After improvement he moved out of town for two years and “fell of the wagon.” Upon returning h restarted his carbohydrate diet and was only partially following it. As you can see, he also admitted to some cheating on the carbohydrate restriction over the holidays. In light of this, carbohydrate restriction decreased his albuminuria from 2400 to 97 mg/g within a period of 18 months.
References:
Siperstein MS, Unger RH, Madison LL. “Further Electron Microscopic Studies of Diabetic Microagniopathy.” Early Diabetes: Advances in Metabolic Disorders, sup 1. New York: Academic Press, 1972, p261-271.
Nasr SH, D’Agati VD. “Nodular glomerulosclerosis in the nondiabetic smoker.” J Am Soc Nephrol. 2007;18(7):2032.
Poplawski MM, Mastaitis JW, Isoda F, Grosjean F, Zheng F, Mobbs CV (2011) Reversal of Diabetic Nephropathy by a Ketogenic Diet. PLoS ONE 6(4): e18604. doi:10.1371/journal.pone.0018604
This evening on PeriScope, we talked about the 10 things you can do to stay motivated on your low-carb lifestyle. A number of great questions were asked including:
How much carbohydrate should be restricted?
What labs should you be monitoring regularly?
What’s a normal blood sugar?
Why is Dr. Nally freezing in Denver?
Is fermented food good for you?
Why should you eat pickles and kimchi even when you’re not pregnant?
And, much much more . . . It’s like a college ketogenic course on overdrive . . . for FREE!!!
You can see the PeriScope with the comments rolling in real-time here: katch.me/docmuscles
Join me as we chew the phat of ketogenic lifestyles PeriScope style and answer many questions like, “Why do I get ‘hangry’?” What causes hypoglycemia? How many times a day should I eat? and many more . . .
We talk briefly about why 60% of people with insulin resistance may need methylated folic acid to help with B vitamin absorption/use and where it can be found. (See me recent article about this called The Power of a Good Vitamin.)
You can see the whole PeriScope conversation on Katch.me/docmuscles with the comments scrolling or you can see the video stream below:
Diseases seem to arrive in three’s each day in my office. Today I had three different patients with cholesterol concerns who were notably confused about what actually makes the cholesterol worse, and what causes weight gain. Each of them, like many patients that I see, were stuck in a state of confusion between low fat and low carbohydrate lifestyle change. My hope is to give my patients and anyone reading this blog a little more clarity regarding what cholesterol is, how it is influenced and how it affect our individual health.
First, the standard cholesterol profile does not give us a true picture of what is occurring at a cellular level. The standard cholesterol panel includes: total cholesterol (all the forms of cholesterol), HDL (the good stuff), LDL-C (the “bad” stuff) and triglycerides. It is important to recognize that the “-C” in these measurements stands for “a calculation” usually completed by the lab, and not an actual measurement. Total cholesterol, HDL-C and triglycerides are usually measured and LDL-C is calculated using the Friedewald equation [LDL = total cholesterol – HDL – (triglycerides/5)]. (No, there won’t be a quiz on this at the end . . . so relax.)
However, an ever increasing body evidence reveals that the concentration and size of the LDL particles correlates much more powerfully to the degree of atherosclerosis progression (arterial blockage) than the calculated LDL concentration or weight (1, 2, 3).
There are three sub-types of LDL that we each need to be aware of: Large “fluffy” LDL particles (type I), medium LDL particles (type II & III), and small dense LDL particles (type IV).
Weight & Size of VLDL, LDL & HDL
Why LDL-C is misleading: Identical LDL-C of 130 mg/dL can have a low risk (Pattern A) with a few “big fluffy LDL particles or high risk (Pattern B) with many small dense LDL particles.
Second, it is important to realize that HDL and LDL types are actually transport molecules for triglyceride – they are essentially buses for the triglycerides (the passengers). HDL can be simplistically thought of as taking triglycerides to the fat cells and LDL can be thought of as taking triglycerides from the fat cells to the muscles and other organs for use as fuel.
Third, it is the small dense LDL particles that are more easily oxidized and because of their size, are more likely to cause damage to the lining of the blood vessel leading to damage and blockage. The large boyant LDL (“big fluffy LDL particles”) contain more Vitamin E and are much less susceptible to oxidation and vascular wall damage.
Eating more fat or cholesterol DOES NOT raise small dense LDL particle number. Eating eggs, bacon and cheese does not raise your cholesterol! What increases small dense LDL particles then? It is the presence of higher levels of insulin. Insulin is increased because of carbohydrate (sugars, starches or fruits) ingestion. It is the bread or the oatmeal you eat with the bacon that is the culprit. The bread or starch stimulates and insulin response. Insulin stimulates the production of triglycerides and “calls out more small buses” to transport the increased triglyceride to the fat cells (4, 5, 6, 7).
Fourth, following a very low carbohydrate diet or ketogenic diet has been demonstrated to decreased small dense LDL particle number and correlates with a regression in vascular blockage (8, 9). So, what does this really mean to you and me? It means that the low-fat diet dogma that that has been touted from the rooftops and plastered across the cover of every magazine and health journal for the last 50 years is wrong. . . absolutely wrong.
I talk about this and answers questions on today’s Periscope. You can see the recording on Katch.me with the comments in real time here:
Superko HR, Gadesam RR. Is it LDL particle size or number that correlates with risk for cardiovascular disease? Curr Atheroscler Rep. 2008 Oct;10(5):377-85. PMID: 18706278
Rizzo M, Berneis K. Low-density lipoprotein size and cardiovascular risk assessment. QJM. 2006 Jan;99(1):1-14. PMID: 16371404
Rizzo M, Berneis K, Corrado E, Novo S. The significance of low-density-lipoproteins size in vascular diseases. Int Angiol. 2006 Mar;25(1):4-9. PMID:16520717
Howard BV, Wylie-Rosett J. Sugar and cardiovascular disease: A statement for healthcare professionals from the Committee on Nutrition of the Council on Nutrition, Physical Activity, and Metabolism of the American Heart Association. Circulation. 2002 Jul 23;106(4):523-7. PMID: 12135957
Elkeles RS. Blood glucose and coronary heart disease. European Heart Journal (2000) 21, 1735–1737 doi:10.1053/euhj.2000.2331
Stanhope KL, Bremer AA, Medici V, et al. Consumption of Fructose and High Fructose Corn Syrup Increase Postprandial Triglycerides, LDL-Cholesterol, and Apolipoprotein-B in Young Men and Women. The Journal of Clinical Endocrinology and Metabolism. 2011;96(10):E1596-E1605.
Shai I et al. Cirulation. 2010; 121:1200-1208
Krauss RM, et al. Prevalence of LDL subclass pattern B as a function of dietary carbohydrate content for each experimental diet before and after weight loss and stabilization with the diets. American Journal of Clinical Nutrition. 2006; 83:1025-1031
Gentile M, Panico S, et al., Clinica Chimica Acta, 2013, Association between small dense LDL and early atherosclerosis in a sample of menopausal women, Department of Clinical Medicine and Surgery, University “Federico II” Medical School, Naples, Italy Division of Cardiology, Moscati Hospital, Aversa, Italy A. Cardarelli Hospital, Naples, Italy
This week I had the pleasure of seeing a really nice 46 year old Hispanic male who is fairly new to the office. He came back in to see me in follow up on his diabetes. To give you a bit of background history, the patient came to see me about 6 months ago, just not feeling very well. Based on his symptoms of fatigue, history of elevated blood sugar and family history, lab work was completed.He saw us initially with a Hemoglobin A1c of 12.3% in June (normal should be 4.9%-5.6%). This means he had an average blood sugar over the previous three months of about 310 mg/dL (normal should be < 110 mg/dL).
Past Medical History include: Diabetes Mellitus – type II (not on any medications when initially seen), Hypertension (high blood pressure), Dyslipidemia (elevated cholesterol) and a non-specific heart arrhythmia.
Medications: None
Surgeries: Knee & shoulder arthroscopies
Family History: Father Diabetes, Stroke, Heart Disease, Hypertension, Elevated Cholesterol
After getting his labs back, we had a very long conversation about the need to either fix his diet dramatically, or he may be looking at using 3-4 oral medications or even insulin to control his blood sugar.
When I see average blood sugars (HbA1c) stay over 6.5% (or greater than 140 mg/dL), the risk for retinal, kidney and nerve damage is significant and often irreversible after 4-5 years. Most physican’s are affraid to lower the HbA1c to less than 7.0% with medications due to low blood sugar events, and so the diabetes community has “settled” with 7.0% as being effective. However, it still isn’t low enough. I saw this happen with my father and with other members of me family. I’ve seen it happen over and over with my patients over the last 15 years when they have not lowered their blood sugar and reduced the high insulin loads that occur in response to those high blood sugar levels. It has been my experience that HbA1c can be very safely lowered to the normal range, as low as 5.2-5.6% without symptomatic low blood sugars, with the correct diet and careful use of medications.
As you can see, a dramatic change in his blood sugar has occurred in a three month interval. Not only that, we see a significant change in his cholesterol profile.
Previously, we looked at LDL-C for heart disease risk, however, I have multiple patients that have had heart disease with normal LDL-C ( <100 mg/dL). LDL-C is just a summation of all the particles. The LDL particle is actually made up of three sub-types and it is specifically the small dense particle that causes the vascular risk. You can see a dramatic normalization of the small dense particle LDL with no change in LDL-C and minimal change in Total Cholesterol in the patient’s labs when he reduces his carbohydrate intake. This is a pattern I see every single day. When serial carotid ultrasound studies are completed, I see reduction in blockage and reduction in the vascular wall thickening. I will be very interested to see the vascular studies on this patient and I will await his results as he tightens up his diet even further.
All in all, he has dramatically brought his diabetes under control with carbohydrate restriction and if he continues this lifestyle, he has reduced his risk for retinal damage, reduced his risk for kidney damage, reduced his risk for nerve damage and essentially added 20 years to his life.
(Disclosures: Dr. Nally has no vested interest, monitary or otherwise, in Novo Nordisc or it’s products including liraglutide.)
Look what I just got in the mail this afternoon. . . my copy of Jimmy Moore & Maria Emmerich’s The Ketogenic Cookbook!
Wow. Great info, fantastic recipes (with amazing pictures, by the way!) and the most up to date ketogenic advise out there. I’m impressed.
What a fantastic addition to my library. I was going snap a few shots of my favorite dishes in it, but my wife picked it up while I was typing and won’t put it down. . . .
I recently read a blog post decrying anyone that would recommend a low carbohydrate / ketogenic diet to their patients.
What?!
In fact, this particular blog outlined a number of “adverse reactions” to a ketogenic diet, and based upon these perceived reactions, the writer advised severe caution with its use in just about anyone. It is important to note at the outset that most of the data this blogger quotes are from older studies completed in children for the treatment of epilepsy with specific liquid ketogenic dietary meal replacements. (Not what you’d expect in a low-carb / ketogenic diet for the average obese adult today.)
Diet Confusion
Thanks to recent misinformation by a number of medical professionals, including the person writing the blog referenced above, a poor understanding of fatty acid metabolism by the general community, and a distinct lack of understanding of human adaptability recorded over the last 5,000-6,000 years, there is still significant confusion about ketogenic diets.
It is important to recognize the crucial fact that the human body is designed to function quite well when supplied any of three macronutrients: carbohydrates, proteins or fats. It does so through an amazing series of enzymatic reactions referred to as the Krebs (tricarboxylic acid) cycle, producing needed ATP (adenosine triphosphate) required for our muscles to contract, our heart to beat and our diaphragm to expand our lungs. What’s even more amazing that that the body was designed to recognize the season we are in based up on the food we eat. That is, until we invented refrigerators in 1913. (Now our bodies think it’s year round summer time . . . wait . . . I live in Arizona where it is year round summer time.)
No, this is not a post about unplugging your refrigerator, living on solar, getting off the grid and saving energy.
Our bodies recognize the seasons we are in based upon inherent hormone release. The key hormone is insulin. Insulin can be looked at as the seasonal indicator to our bodies. Insulin production rises and falls based on our intake of carbohydrates (sugar, starches, some fibers). Insulin, essentially, tells our bodies when it is a “time of plenty” and when it was a “time of famine.” Why? You ask. We didn’t have refrigerators 100 years ago and you were lucky if you had a root cellar. The body needs to know when to store for the famine (the winter) that was around the corner. Insulin is that signal.
During the summer, potatoes, carrots, corn and other fruits are readily available. These are all starchy carbohydrates and they all require the body to stimulate an insulin response so that they can be absorbed. Insulin stimulates fat storage (J Clin Invest. 2000;106(4):473-481. doi:10.1172/JCI10842). Just like bears, our bodies were designed to store for the winter.
If you think back in history, your grandparents probably used stored meats & cheeses that could be salted or smoked for preserving during this time of year. Those crossing the plains were commonly found with pemmican, a concentration of fat and protein used as a portable nutrition source in the absence of other food. (Chapter VIII. Narrative of the Life of David Crockett, of The State of Tennessee, Written by Himself, Sixth Edition [E.L. Carey and A. Hart:Philadelphia] 1834, 1837; Marcy, The Prairie Traveler, p. 31.) Think about conversations you may have had with your grandmother when she told you that for Christmas, she received an orange. A single orange for a gift?! Many of my patients drink 12-15 of them in a glass every morning. The winter diets of our grandparents were very low in starches and carbohydrates. When carbohydrate intake is low, little insulin is produced.
Again, insulin is the hormone that tells you that you’re in “a time of plenty” and stimulates weight gain and cholesterol production to prepare for winter. Those prescribing the use of ketogenic diets understand this innate human adaptive trait, and use it to effect changes in weight, cholesterol and other desired metabolic changes.
Three types of ketones. Uptodate.com, May 2015
Now, let’s define the difference between ketosis and keto-acidosis and try to clarify the misinformation that is being spread around the blogosphere.
A ketone is a molecule the body produces from the breakdown of fat and some proteins (amino acids). There are specifically three types of ketones: beta-hydroxybutyric acid, acetoacetic acid and acetone. If ketosis was “bad,” then why would our bodies produce these molecules? They are not bad, and in fact, multiple studies show that the body is often more efficient and effective when it functions on ketones rather than glucose as its primary fuel source. The body can only supply a limited amount of sugar or glucose for fuel. If you talk to runners, marathoners or triathletes, they will tell you that after about 45-90 minutes of continuous endurance exercise the glucose supply runs out and they will experience what is termed a “bonk” (have a low-blood sugar or hypoglycemic episode). Unfortunately, our bodies can only store about 18-24 hours of glucose.
Metobolic Changes of Ketogenic Diet (American Journal of Physiology – Endocrinology and Metabolism Published 1 June 2007 Vol. 292 no. 6, E1724-E1739 DOI: 10.1152/ajpendo.00717.2006)
However, the body can store days upon days of fat in the form of triglyceride in the fat cells. Triglyceride is broken down into ketones. If glucose is the “unleaded” fuel, you can think of ketones as the “diesel fuel” that is easier to store and runs longer.
The average body functioning on ketones as the primary fuel will have a ketone level measured in the blood somewhere between 0.4 and 4 mmol/L. Because of a balance that is created by the use of ketones and a feedback mechanism that kicks in when the ketone level rises, the body will maintain a pH of around 7.4.
Ketoacidosis is dramatically different. If you are a type I diabetic, you don’t produce any insulin. The feedback mechanism regulating ketone use is broken and the ketone levels and triglyceride breakdown speeds up because the body can’t access glucose and can’t produce insulin. The ketone levels spike and the level can rise to > 25 mmol/L. In the presence of a high blood sugar and high ketone level, the acid level in the blood shifts to a pH of less than 7.3. This is referred to as metabolic acidosis and can be life threatening as the low pH shuts down the bodies’ enzymatic processes and a person becomes critically ill and without treatment, can die. (Kitabchi AE et al., Clinical features and diagnosis of diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults. www.uptodate.com, May 2015.)
If you’re not a type I diabetic, you have nothing to worry about. Regardless of what the “ketogenic nay-sayers” blog about, your liver makes approximately 240g of glucose per day, this stimulates a basal release of insulin which keeps the pH in check. It’s also what keeps weight loss at a consistent pace of around 2-10 lbs per month.
If you are a type I diabetic, don’t fret. Carbohydrate restriction can still be used very effectively. It just takes some balancing and understanding of your individual metabolism. Talk to your physician and/or medical bariatrician about how to follow a carbohydrate restricted diet while using insulin.
What about all the other “adverse effects” the blogosphere and other so-called experts claim about ketogenic diets?
Let’s take them on one by one. Are you ready?
Gastrointestinal (GI) disturbances – Yes. Any time you change your diet you may experience diarrhea, constipation or gassiness. Most of the time, this is because you are either 1) not eating enough leafy greens (fiber) or 2) you’re using a supplement that contains an artificial sweetener. Most of the studies on ketogenic diets did not incorporate fiber and the studies used to make this point were on children who used a ketogenic fat supplement shake or liquid preparations containing these artificial sweeteners to make them palatable. If you have spoken to any bariatrician, they will tell you, the best way to follow a ketogenic diet is to eat real food. If you want to read about the anecdotal GI effects of sweeteners, read the comment section in Amazon about the Haribo Sugar Free Gummy Bears.
Inflammation Risk – In every patient that I have placed on a ketogenic diet in the last 8 years, all inflammatory markers including CRP, Sedimentation Rate and Uric Acid have all decreased. Inflammation gets better on an appropriately formulated ketogenic diet. The older studies of ketogenic diets in children contain most of their fat from Omega-6 fatty acids from vegetable oil which will increase inflammation and oxidative stress, spike the cortisol levels and have the secondary effect of actually raising the triglycerides. (Simopoulos AP,The importance of the ratio of omega-6/omega-3 essential fatty acids, Biomed Pharmacother., 2002 Oct;56(8):365-79.)
Muscle Cramps/Weakness – The process of weight loss occurs by burning fat into CO2 and water. We breathe the CO2 out, but the water produced has to follow salts out through the kidneys. Hence, we lose salts. This can cause weakness and muscle cramps. The solution? Stop restricting salt on a low carbohydrate diet. We are the only mammal that restricts salt and we do it because low-fat diets cause us to retain water. Low carbohydrate diets do the opposite. Use sea salt or sip beef or chicken bouillon broth with your dinner. The use of yellow mustard also helps (the small amount of quinine in yellow mustard stops the cramping). If you have congestive heart failure, talk to your doctor about monitoring your salt intake in balance with your diuretic or water pill.
Hypoglycemia – If you read the ketogenic diet research, most of it was done on epileptic children. The diets called for a period of starvation, then the use of a ketogenic liquid based on the John’s Hopkin’s protocol. It is a well-known fact in medicine that starvation in children can frequently cause hypoglycemia, especially in children with other genetic or congenital defects leading to forms of epilepsy. In clinical practice, with ketogenic diet use in adults, hypoglycemia is rare.
Low Platelet Count (Thrombocytopenia) – Again, this was seen in the epileptic children who were placed into starvation first, then introduced a liquid fat replacement shake to stop intractable seizures. These liquids or shakes were often nutrient deficient in other essentials. Folic acid, B12 and copper deficiency can occur when not eating “real food.” Low platelet counts are rarely seen on ketogenic diets based around “real food.” Many children in the ketogenic studies had been on or were concomitantly on valproic acid for their seizures. Valproic acid is commonly known to cause thrombocytopenia (Barry-Kravis E et al, Bruising and the ketogenic diet: evidence for diet-induced changes in platelet function. Ann Neurol. 2001 Jan;49(1):98-103.; Kraut E, Easy Bruising, http://www.uptodate.com, May 2015.)
Easy Bruising – This is usually due to inadequate protein supplementation as was the case in much of the ketogenic literature where protein levels were also restricted. (Kraut E, Easy Bruising, http://www.uptodate.com, May 2015.)
Pancreatitis – Patients who are insulin resistant or have impaired fasting glucose commonly have high triglycerides. Elevation in triglycerides itself is a cause of pancreatitis. Ketogenic diets lower the triglycerides. However, if a patient has not been following their diet as directed, spikes in the triglycerides can occur placing the person at risk for pancreatitis.
Long QT Intervals/Heart Arrhythmias – The list of things causing Long QT intervals and abnormal heart rhythms is long and variable (Acquired Long QT Syndrome. Berul C et al. www.uptodate.com, May 2015). It is well know that starvation, rapid weight loss and liquid protein diets can cause a delay in the conduction signal in the heart. Anyone wishing to start any diet should have an electrocardiogram (EKG) through their doctor to ensure that the diet (of any type) doesn’t exacerbate a prolonged QT interval.
Three year weight loss and metabolic improvement in a patient on a Low-Carb / Ketogenic diet. Note: Patient admits to not following ketogenic diet during holidays from Nov 2013 – Feb 2014 (see the dramatic changes to the body when cheating happens)
Cardiomyopathy – Prolonged QT intervals have been associated with cardiomyopathy and the former can stimulate the later. Any diet that has the potential to prolong a QT interval has the potential to cause cardiomyopathy. Hence the need for regular EKG monitoring on any diet (Acquired Long QT Syndrome. Berul C et al. www.uptodate.com, May 2015).
Lipid/Cholesterol Changes – In the 8 years I have been applying ketogenic diets to patients, I have seen dramatic improvement in the triglycerides and HDL levels. The only time triglycerides rise over 100 is if the patient is using artificial sweeteners or is cheating on the carbohydrate restriction. Total cholesterol commonly rises, however, this is indicative of the fact that there is a shift in the LDL particle size and this affects the calculation of both total cholesterol and LDL-C. In light of this, most of my patients have dramatic improvement in triglycerides and small dense LDL particle number. I’ve included the common cholesterol changes I seen in my office as a few case reports to demonstrate the effectiveness of a ketogenic diet:
2 year ketogenic dietary labs and weight loss
Myocardial Infarction – It is interesting that one blogger includes this on the list of adverse reactions, however, when you actually read the study, the author of the paper make an “assumption” that there was potential for heart attack due to an elevated total cholesterol, however, a correlation was never made. Again, in the 8 years I have been using ketogenic diets, I have seen dramatic improvement in cholesterol profiles, inflammatory markers, atherosclerosis and carotid intimal studies (Shai I et al, Circulation 2010; 121:1200-1208).
Three year metabolic history of a Low-Carbohydrate / Ketogenic diet
Menstrual Irregularities / Amenorrhea – It is well known that any diet causing protein or other nutritional deficiency will affect the menstrual cycle first and growth second. The only time menstrual irregularities occur with a ketogenic or Low-Carb diet is when a patient is not taking in enough protein or is not eating real food. What amazes me is that a properly applied ketogenic diet causes normalization of the menstrual cycle, and in my practice, I’ve had a number of women successfully be able to conceive after making a ketogenic dietary change.
For more details on the nutrient content of a ketogenic diet, see the recent article by a friend of mine, Maria Emmerich. She’s been creating ketogenic diets for years and has a number of fantastic books my wife and I have been using in our home over the last nine years. She is one among many that can give you some direction on how to devise a healthy, real food based ketogenic diet. See the page on my website here that will give you some direction in formulating your Ketogenic Lifestyle.
Nally Family Low-Carb / Ketogenic Cheese Cake
So, to celebrate Mother’s Day, today, with my family, I am going to indulge in some Low-Carb / Ketogenic Cheese Cake!! Happy Mother’s Day, to all of you and especially to all you mothers out there making a healthy difference in the lives of your families! (You can find the recipe for this delicious cheese cake here)
In the words of Sir William Ostler, “If it were not for the great variability among individuals, medicine might well be a science and not an art.”
I have multiple patients that come to my office that we follow and treat for weight loss and metabolic syndrome. They are discouraged that their weight loss has stopped or is very, very slow. The most frequent problem I find when they bring in their food journals is the “healthy chicken salad.”
“What?! But, Doc, Chicken Salad is healthy?! RIGHT?”
The chicken salad shows up on their journal almost daily. Somehow, we’ve been indoctrinated that the chicken salad is good for us. I want you to look closely at the image that was recently shared on the internet below. How is the nutrient value of your chicken salad any different than the Big Mac?
Why is this unhealthy? The carbohydrate content greater than 20-30 grams will cause a spike in insulin. When insulin spikes, the body is told to store fat (and it will store fat for up to 12 hours) . . . Yes, the 24 grams of fat in the salad now become dangerous in the presence of an insulin spike. In my patients with metabolic syndrome, they will produce between two and ten times the insulin and store two to ten times the fat. (Ten Big Macs would have tasted better . . . )
There is actually more carbohydrate in your salad than in the big mac. Why not add a strawberry shake just to finish putting the nail in the coffin? And we wonder why we are having trouble with weight loss?
The other issue, and probably of even greater importance, is that chicken breast has the second highest content of lysine & argenine (two of the 10 essential amino acids) count of all the poultry family. This is second only to turkey breast, which also contains a large amount of tryptophan (a third essential amino acid that spikes insulin). Why is this a problem? Because argenine, tryptophan and lysine all stimulate an insulin response on their own, separate from glucose. We need these amino acids, however, when our meals contain a predominance of these amino acids, it rasies insulin significantly in those who are insulin resistant (pre-diabetic).
Those 43 carbohydrates, plus the stimulus from a meat high in argenine, lysine and tryptophan, spike your insulin, kick you out of nutritional ketosis and slow weight loss for up to 48 hours.
Please, if you are following a low-carb or ketogenic diet, get rid of the chicken salad.
There are a number of recipes for “Fat Bombs” on the internet, but this one is my wife’s version. These have been a lifesaver for starting and maintaining a Low-Carbohydrate or Ketogenic diet over the last few years. They are fantastic mid-meal or anytime Low-Carb snacks, full of satiating fat, that really help during the holidays. I mentioned Fat Bombs to my patients in my Low-Carb Group Visit Class today and I promised to post them here:
Fat Bombs:
1 stick of real Butter softened
1 cup Coconut Oil
1/2-2/3 cup Erythritol
1 tsp liquid Stevia
1/3 cup Cocoa Powder
1 cup Peanut Butter or Almond Butter
2 cups chopped Macadamia Nuts or slivered Almonds
1-2 cups of Coconut
Mix together and place 1-2 table spoon sized scoops in small muffin tin or on wax paper. Must be kept refrigerated to remain firm.
“You want me to eat WHAT?! But that’s . . . ,it’s . . . FAT, really?”
” Yes, it is.”
Every day, instruction to my patients is initially seen as Food Pyramid heresy and My Plate iconoclasm. Yes, I want you to flip the Food Pyramid on its head, and push everything off My Plate and fill it with fat. . . Really. . . Yes, I do.
I was counseled by many school professors over the years that there are two things you should avoid talking about: Religion & Politics. The ketogenic or low carbohydrate dietary conversation involves both. “Fat Phobia” is a Religion. We have demonized fat and sainted the treadmill. You see, fat got a bad wrap when the bomb calorimeter was invented. We realized that there was twice as much energy found in fat that there was in carbohydrate or protein. Early nutritionists, understanding that heat is a form of energy, and realizing that energy is conserved, found that food substrates contain a set amount of energy that can be measured in a closed environment. Naturally, the Law of Thermodynamics got applied to lend understanding in how people gain or loose weight. We coined the term “you are what you eat” based upon our understanding of the Laws of Thermodynamics. The calorie became “king.”
1 gram of carbohydrate = 4 kcal
1 gram of protein = 4 kcal
1 gram of fat = 9 kcal
For the last sixty years (an entire generation of humans) we have based our diet around the calorimetry of food and have labeled them as good or bad based upon calories. To loose weight, we are taught, you either have to eat food containing fewer calories (fat has the most calories per volume so it must be bad!) or burn it off faster than you take it in (did you go exercise at that new gym next door), right? Wrong.
First, you and I are not bomb calorimeters. We are not closed systems. We harbor variable levels of symbiotic bacteria (these also burn fuel at variable rates) and our body temperatures fluctuate to regulate other enzymatic and hormonal processes.
Second, bomb calorimetery functions on the premise that volumes are also held at a constant. Human volume and density change daily. Simple chemistry tells us that volume = mass / density. The average human mass fluctuates by 5lbs every day and our density changes based upon our hydration status (the amount of water we drink). Because these two variables are not constant in a human being, it is impossible to correctly apply the Laws of Thermodynamics to the human body and accurately predict weight gain or loss.
Third, hormones! (Anyone married to a pregnant female understands that nothing is as it seems when hormones are involved.) We have a plethora of hormones that change the rate in which fuels are burned or stored in the human body. Our GI flora (symbiotic bacteria in the human gastrointestinal tract) are also affected by hormones and do not have set rates of fuel use or breakdown. What this means is that you and I process food at different rates and derive different levels of energy and fuel from the same donut. Genetics plays a leading role in how these hormones are used and turned on and off. Fat is burned or stored in the body based on a hormonal mechanism I described in a previous post you can read here.
Asking patients to reduce carbohydrate intake to less than 20 grams per day and increasing fat intake to up to 70% of total caloric intake is essentially 20th century nutritional apostasy.
The dietary concepts from the Food Pyramid and My Plate have been embraced by our country for over sixty years. Changing our views on these as a country will be for many like changing religions. For those of us “with eyes to see and ears to hear” our work is cut out for us.
Does your job limit interaction with people and/or do you spend most of your time with a computer screen?
Have you become cynical or critical at work?
Do you drag yourself to work and have trouble getting started once you arrive?
Have you become irritable or impatient with co-workers, customers or clients?
Do you lack the energy to be consistently productive?
Do you lack satisfaction from your achievements?
Do you feel disillusioned about your job?
Are you using food, drugs or alcohol to feel better or to simply not feel?
Have your sleep habits or appetite changed?
Are you troubled by unexplained headaches, backaches or other physical complaints?
These are the ten most common signs of “burnout.” 46% of respondents in surveys indicate at least one of the above symptoms of burnout. Two or more of these imply that you are suffering from some degree of “burnout.” The classic triad of burnout is:
Exhaustion
Cynicism
Questioning the quality of your work, or questioning whether you are making a difference in the world any longer
What is burnout? It is defined by “Mr. Webster” as “physical or mental collapse caused by overwork or stress.” But, that definition doesn’t seem to do it justice, and many people experiencing burnout don’t actually “collapse.” They do, however, become significantly less productive, depressed, and loose the enjoyment of life. Work begins to feel like slavery, exercise becomes a chore, food begins to have associations with guilt, friendships are seen as obligations and love looses its luster and looks more like a social construct.
Burnout is often likened to discontent, however, these are two very different emotional feelings. Discontent can be defined as dissatisfaction with ones circumstances. There are two kinds of discontent in this world: the discontent that works and the discontent that wrings its hands. The first kind often gets what it wants and the second looses what it has.
Burnout differs from discontent, in that continued work toward a goal brings on the triad of emotional exhaustion, depersonalization and the feeling of reduced personal accomplishment. Burnout is, in reality, the sum total of hundreds of thousands of tiny betrayals of purpose.
Burnout can occur in any field of work, however, a study published in the 2012 issue of JAMA reveals that over 40% of the ~800,000 U.S. physicians are experiencing burnout and are more prone to burnout than any other worker in the United States. The journal Academic Medicine recently reported that medical students, when compared to age-matched fellow college graduates, reported significantly higher rates of burnout.
So, how do you overcome burnout?
I’m an Osteopath. I see disease in the context and inter-relationship of the mind, body & spirit. Overcoming burnout requires one to restore balance in these three areas. I am impressed by the work of Charlie Hoehn in his book, Play it away: A workaholic’s cure for anxiety. Charlie does a wonderful job of describing the broken inter-relationship of the mind, body and spirit in a person experiencing burnout.
The first step to repairing the broken inter-relationship is to recognize and remove those anchors keeping you tethered to the feelings of burnout. The anchors are the stressors that cause you to worry on a daily and weekly basis. Journaling these stressors, writing them down in 3-5 word sentences is the start. Identify which of these stressors is the biggest or causes the most angst, then write out the following question. “How can I eliminate [stressor] from my life? Do this with the largest two or three stressors. Then write out a solution that is small and uncomplicated to each stressor. Put the solution to work immediately. If your solution has not improved your feelings of stress and anxiety within a week, then drop the first and try to find a second stressor, or otherwise switch to a second solution. Journaling these thoughts, questions, feelings and answers allows your mind to change from a self-centered focus to an action based focus. It clears the mind to move into action. Nothing is more important in reducing burnout, than nourishing the imagination. Using a journal helps stimulate thought and the imagination.
The second technique is scheduling some real play. Write down the five most fun activity involved with play that you did as a child. Then, set aside dedicated time for your favorite activity of play. It is essential that you actually schedule this play time into your daily activities. There are a couple of rules associated with play time.
Disconnect from all social media
Harmony of the playtime is more important than winning
Have some serious fun
Shoot for 30 minutes of play time per day
This should ideally be done outside in the fresh air and sunlight
“A lack of play should be treated like malnutrition: it’s a health risk to your body and your mind.” (Stuart Brown)
“Play is the highest form of research.” (Albert Einstein)
Technique number three is related to sleep. It is essential that you have a consistent bedtime and give yourself the opportunity to take an afternoon nap. You can optimize your sleep by turning off electronics before getting into bed, going to bed at the same time each night, decreasing the room temperature to 68-70 degrees Fahrenheit, draw the curtains to make the room dark, and use a relaxing loop of quite background sound like ocean waves, or the sound of a trickling stream to ease your mind (can be found on a number of apps).
It may take up to a week for your body to unwind and get used to this schedule. Also, schedule a 20 minute afternoon nap.
Meditation and/or prayer is the fourth technique. Sit or kneel, close your eyes and observe the thoughts that enter your mind for 10-15 minutes. Listen to and keep your breathing calm and deep. Pay attention to the rhythm of your breathing. Reading can also be a form of meditation and has become an important refreshing part of alleviating burnout. We can only be as good as the books that we read. Read, ponder over and talk about good books.
Fifth, eat healthy meals with healthy friends. Decrease the carbohydrates and increase the good omega 3 fats in your diet. The insulin response to carbohydrates stimulates the inflammatory and parasympathetic nervous system making you more fatigued and tired. Reduce the bread, rice, pasta, potatoes, carrots and corn intake in your diet.
Increasing the good fat in your diet (like Kerrygold Irish Butter, Coconut Oil, Olive Oil, and real animal fats) actually increases your bodies access to essential B vitamins and improves the use of Vitamin D. Making dietary changes become a habit is often easier when it is done with a friend. Schedule opportunities to eat healthy meals with family or friends attempting to do the same thing. You will help support each other and be more likely to succeed.
The last recommendation is spend time in nature. One weekend a month spend at least two hours out in nature. Take a hike, go on a nature walk, go camping, swim in the river, etc. Give yourself permission to unplug during these times. Then, pay close attention to how you feel when your in different environments.
In the words of Shakespeare, “Self-love, my liege, is not so vile a sin/As self-neglecting” (King Henry V, Act 2, scene 4).
I conclude with the rhetorical question, “If you work for a living, why do you kill yourself working?” (The Good, The Bad, and the Ugly)
Symptoms of Inflammation seen in Diabetes Mellitus
A recent study published in the Annals of Internal Medicine demonstrate significant improvement in overall inflammation in type II diabetic patients following a carbohydrate restricted diet versus a low fat calorie restricted diet. Another bit of proof demonstrating what I’ve been seeing in my office over the last 8 years. The study reveals significant improvement in glycemic (blood sugar) control in those following a low carbohydrate diet as well as significant lowering of C-reactive protein, IL-1 and IL-6 over those following a low fat diet. You can see the study here.
You know, Dr. Seuss was right, the whole egg is actually good for you.
A recent study from the University of Connecticut demonstrated that eating the whole egg actually decreases LDL (the bad cholesterol) sub-particles and insulin resistance in Metabolic Syndrome better than the egg white or the egg substitute.
I like green eggs and ham!
I do!! I like them, Sam-I-am!
And I would eat them in a boat!
And I would eat them with a goat…
And I will eat them in the rain.
And in the dark. And on a train.
And in a car. And in a tree.
They are so good so good you see!
As a medical bariatrician and family practitioner specializing in low-carbohydrate diets, I often see the panic stricken look on people’s faces when they look at their cholesterol profiles just after starting a carbohydrate restriction life-style.
First, it is very important to understand that if you check your cholesterol within the first 4-6 weeks of dietary changes, there will be a transient rise in the cholesterol profile as your adipose tissues (fat cells) release your new fuel source into the blood stream and the mitochondria in the one trillion cells in your body convert from the use of glucose to the use of ketones (derived from triglycerides) as the primary fuel source. This is not a problem as the body is designed to handle this increase in triglyceride and cholesterol. I explain to patient’s that we are essentially making the figurative change from “un-leaded fuel to diesel fuel.”
Second, the standard cholesterol profile does not give you a true picture of what is occurring at a cellular level. The standard cholesterol panel checks Total cholesterol (all the forms of cholesterol), HDL (the good stuff), LDL-C (the bad stuff) and triglycerides. It is important to recognize that the “-C” stands for a calculation usually completed by the lab.
Cholesterol Particle Sizes
Total cholesterol, HDL and triglycerides are usually measured and LDL-C is measured using the Friedewald equation [LDL = total cholesterol – HDL – (triglycerides/5)].
Third, it is also important to realize that HDL and LDL are actually transport molecules (the buses for the triglycerides (the passengers). HDL is taking triglycerides to the fat cells and LDL is taking triglycerides from the fat cells to the muscles and other organs for use as fuel.
When you being a low carbohydrate diet, your blood glucose availability as the primary fuel source drops and triglycerides become the primary source. It takes your body 4-6 weeks to increase the number of mitochondria necessary to effectively use triglycerides as the primary fuel. (This is why many athletes and patients who are active will feel slightly sluggish during their exercise for the first few weeks).
Once your body accommodation to the new fuel, there will be a notable drop in LDL-C and a rise in the HDL.
But this still doesn’t answer the question and relieve the panic seen above. A deep sigh and the look of relief occurs when I explain that LDL-C doesn’t give us the real story.
To make it simple and understandable, LDL is made up of three main sub-types big fluffy ones, medium sized ones, and small dense ones. It’s the small dense ones that contain lipoprotien A [Lp(a)] found in increased vascular risk. Recent studies reveal that heart disease and atherosclerosis is caused by the small dense LDL molecules.
A low carbohydrate diet causes the small dense cholesterol to drop and there is a rise in the two other sub-types This shift in sub-types can actually elevate the Total Cholesterol number and occasionally the LDL-C.
If you are following a low carbohydrate diet, get your cholesterol levels checked. It is more ideal to get an NMR Lipoprofile or VAP Cholesterol test that will give you an LDL particle number and this can be explained more fully by your doctor.
Now, off to the fridge . . . where did I put that package of bacon . . . ?











 the underlying cause. I see this problem in a very large majority of the people in my office and I am seeing people younger and younger show up with continually increasing blood pressure.
the underlying cause. I see this problem in a very large majority of the people in my office and I am seeing people younger and younger show up with continually increasing blood pressure.

 begin to back down their blood pressure medications, they would experience symptoms of dizziness, light-headedness, headache and a few patient’s nearly passing out. On a low-carbohydrate, high-fat (ketogenic) diet you need salt (sodium, potassium, & magnesium).
begin to back down their blood pressure medications, they would experience symptoms of dizziness, light-headedness, headache and a few patient’s nearly passing out. On a low-carbohydrate, high-fat (ketogenic) diet you need salt (sodium, potassium, & magnesium).










 After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the
After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the 
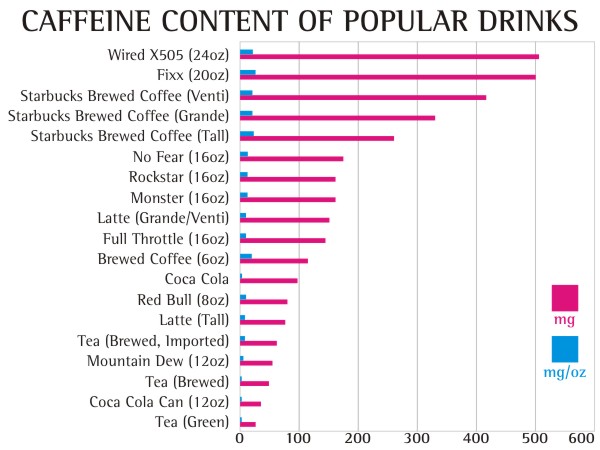
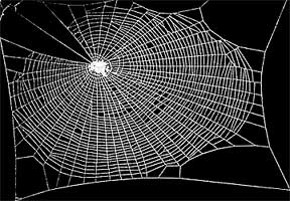


 People with significant stressors in their life have been show to have an increased corsiol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing a daily, cyclic over production of cortisol and then normalization of cortisol after resolution of the stressor. This cortisol response is not high enough to lead to a true
People with significant stressors in their life have been show to have an increased corsiol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing a daily, cyclic over production of cortisol and then normalization of cortisol after resolution of the stressor. This cortisol response is not high enough to lead to a true  Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids or proteins into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues (by stimulating insulin production) and turns on the maturation process of adipocytes (it makes your fat cells age – nothing like having old fat cells, right?!) In the process, cortisol suppresses the immune system through an inhibitory effect designed to decrease inflammation during times of stress (7,8,9). If this was only occurring once in a while, this cascade of hormones acts as an important process. However, when cortisol production is chronically turned up, it leads to abnormal deposition of fat (weight gain), increased risk of infection, impotence, abnormal blood sugars, brain fog, head
Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids or proteins into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues (by stimulating insulin production) and turns on the maturation process of adipocytes (it makes your fat cells age – nothing like having old fat cells, right?!) In the process, cortisol suppresses the immune system through an inhibitory effect designed to decrease inflammation during times of stress (7,8,9). If this was only occurring once in a while, this cascade of hormones acts as an important process. However, when cortisol production is chronically turned up, it leads to abnormal deposition of fat (weight gain), increased risk of infection, impotence, abnormal blood sugars, brain fog, head
























