“I’ve tried your low-carb diet, Dr. Nally, and it didn’t work.”
“Hmm . . . really?” If you’re mumbling this to yourself, or you’ve said it to me in my office, then lets have a little talk. You’ve probably been subjected to the common ketosis killers.
 I’ve heard this statement before. It’s not a new statement, but it’s a statement that tells me we need to address a number of items. If you’ve failed a low carbohydrate diet, I’d suspect you are pretty severely insulin resistant or hyperinsulinemic. You probably never really reached true ketosis. I’d want to have you checked out by your doctor to rule out underlying disease like hypothyroidism, diabetes, other hormone imbalance, etc.
I’ve heard this statement before. It’s not a new statement, but it’s a statement that tells me we need to address a number of items. If you’ve failed a low carbohydrate diet, I’d suspect you are pretty severely insulin resistant or hyperinsulinemic. You probably never really reached true ketosis. I’d want to have you checked out by your doctor to rule out underlying disease like hypothyroidism, diabetes, other hormone imbalance, etc.
Nutritional Ketosis is Most Effective as a Lifestyle Change
Next, switching to a low-carbohydrate lifestyle is literally a “lifestyle change.” It requires that you understand a few basic ketosis principles. And, it takes the average person 3-6 months to really wrap their head around what this lifestyle means . . . and, some people, up to a year before they are really comfortable with how to eat and function in any situation.
I assume, if you are reading this article, that you’ve already read about ketosis and understand the science behind it. If not, please start your reading with my article The Principle Based Ketogenic Lifestyle – Part I and Ketogenic Principles – Part II. If this is the case, then please proceed forward, “full steam ahead!”
There are usually a few areas that are inadvertently inhibiting your body transformation, so let’s get a little personal.
Nutritional Ketosis is a Very Low Carbohydrate Diet
First, this is a low carbohydrate diet. For weight loss, I usually ask people to lower their carbohydrate intake to less than 2o grams per day. How do you do that? (A copy of my diet is accessible through my membership site HERE.) You’ve got to begin by restricting all carbohydrates to less than 20 grams per day. Any more than 20 to 30 grams per day will cause an insulin release from the pancreas and stimulate fat storage of both carbohydrate and fat for the next 10-12 hours, commonly killing ketosis. Keep a dietary journal to record your progress, your cravings, your successes and failures. I’m going to want to see it and review it with you if you see me.
No, I don’t believe in “Net Carbs.” Net Carbs are a sales gimmick to get you to buy “artificial food” that keeps you coming back for “artificial food” and halts your weight loss (you’ll see why shortly). You’re going to lose the most weight and feel your best when you eat real food. I do allow for the subtraction of real fiber, specifically non-cooked, non-blended, non-juiced leafy greens (If you cook, blend or juice a leafy green, it activates more carbohydrate availability). Leafy greens are real fiber. You can subtract them. In fact, I recommend eating 1-3 cups of leafy greens per day to help bowel function & provide necessary folic acid, but, everything else is “carbage.” Avoid it.
Yes, cottage cheese and yogurt contain carbohydrates. Be very cautious with them.
No, oatmeal and Cream of Wheat™ are not helpful. See my article on Why Your Oatmeal is Killing Your Libedo.
Alcohol also halts your weight loss. It’s not the sugar in the alcohol I’m worried about, the distilling process changes the sugar to alcohol, however, alcohol stimulates an insulin response after the alcohol is metabolized in the liver with a SIMILAR RESPONSE to regular sugar.
To Effectively Maintain Nutritional Ketosis, You MUST get adequate Protein
Second, this is a low carbohydrate, moderate protein, high fat lifestyle. N0 . . . it is NOT a high protein diet! However, so many of my patients don’t eat enough protein that they feel like it is a “high protein diet.”
Protein is essential for the building and maintaining of muscle, connective tissue and a number of other enzymatic reactions in your body. However, in patients who are morbidly obese [people with a body mass index (BMI) over 50], excess protein intake can cause fat to be stored by producing an excessive insulin response. In these patients we initially moderate protein. Excess sugars and a number of proteins, in the presence of a high insulin response, are converted to triglyceride (the soft squishy stuff inside the fat cells that make them plump) and stocked away inside your adipose tissue. Excessive protein, especially the amino acids argenine, leucine and tryptophan are common ketosis killers, not because they are converted to sugar, but because they stimulate and insulin response all by themselves.
If you don’t fall into the morbidly obese category (BMI over 50). Then, I encourage you to use the protein levels below.
Initially, I ask my patients to focus on lowering their carbohydrate intake and I don’t really worry about protein. (It is often hard enough to figure out what the difference between a carbohydrate and a protein in the first month or two if you’ve never had any nutrition background.) Most people begin losing weight just by lowering carbohydrates over the first few months. Once you figure out how to lower your carbohydrates, if your weight loss is not moving and your pants are not getting looser, then you’re probably eating too much protein.
How much protein do you need? It’s pretty easy to calculate and is based on your height and gender. Your basic protein needs to maintain muscle, skin and hair growth are as follows:
- 70 grams or higher for women per day
- 120 grams or higher for men per day.
However, these levels are WAY TOO LOW for weight loss and maintaining good health. Because we now know that protein acts as a hormone in a number of ways, in my office I recommend women get 80-90 grams of protein per day, and men should get > 150 grams of protein per day.
 If you’re still a little confused about protein, read my article on Why Your Chicken Salad Stops Your Weight Loss.
If you’re still a little confused about protein, read my article on Why Your Chicken Salad Stops Your Weight Loss.
This also goes for protein powders and protein shakes. Many of these have 25-40 grams of protein in them per serving, so be careful with their use.
Nutritional Ketosis is a High Fat Diet
Third, this is a high fat lifestyle. Yes, I want you to INCREASE your fat intake. I’m going to repeat that, again, just for clarity, . . . . INCREASE your fat intake. Increase it to around 50% of your total calories, . . . 70% of your total calories if you can do it. Not enough fat is a common ketosis killer.
“What?! Won’t that cause heart disease and stroke and make my cholesterol worse?!!!”
I know, take a big deep breath . . . (you may even need to breath into a paper bag for a minute if you begin hyperventilating).
No, it will not raise your cholesterol, cause heart disease, or cause a stroke. If you have lowered your carbohydrate intake to less than 20 grams per day, then there is NO hormonal signal for you to make more bad cholesterol, worsen heart disease, or cause a stroke. In fact, there is great data showing that increasing your fat and lowering your carbohydrates reverses the blockage in the arteries. I see this reversal every single day in my clinic through the application of ketogenic diets.

If we remove carbohydrate as your primary fuel, you must replace it with something else. That something else should be fat. Protein must be moderated, as it will also be stored as fat if you eat too much. So, if the carbohydrates are kept low, fat intake can be increased and the body will pick the fat it wants and essentially throw the rest out without raising cholesterol, causing weight gain or causing heart disease. This is why we want you to use good natural animal fats like butter, hard cheese, olive oil, coconut oil, avocado, etc. Look for fats highest in omega-3 fatty acids as these decrease inflammation and improved weight loss. Look for meats highest in fat like red meat (55% fat) and pork (45% fat). Take the food pyramid and flip it over.
That something else should be fat. Protein must be moderated, as it will also be stored as fat if you eat too much. So, if the carbohydrates are kept low, fat intake can be increased and the body will pick the fat it wants and essentially throw the rest out without raising cholesterol, causing weight gain or causing heart disease. This is why we want you to use good natural animal fats like butter, hard cheese, olive oil, coconut oil, avocado, etc. Look for fats highest in omega-3 fatty acids as these decrease inflammation and improved weight loss. Look for meats highest in fat like red meat (55% fat) and pork (45% fat). Take the food pyramid and flip it over.
Check Your Sweeteners At the Door
The fourth common ketosis killer and culprit in halting your weight loss is artificial sweeteners. There are quite a few of them. Most of them WILL cause an insulin response (exactly what we don’t want for weight loss) with minimal to no rise in blood sugar. Raising blood sugar doesn’t matter, if the insulin is being stimulated . . . “you’re gonna gain weight for the next 10-12 hours.” I wrote an article for you to print off and hang on your fridge, upload it to your iPhone or carry it with you in your purse to the grocery store. (If you’re a man and you’re carrying a purse, please don’t tell me about it.) You can find the article here: The Skinny About Sweeteners. The short list of those sweeteners that are OK to use and cook with, and do not increase insulin response, can be found here in my Amazon Store.
Don’t Even Start with Coffee Creamers
 Fifth on my list is coffee creamer. Coffee creamer contains corn syrup solids (another very special name for . . . SUGAR!!) and/or maltodextrin (SUGAR’s married name!). If you must put something in your coffee, then use real heavy cream (pure tasty fat) or real butter. It will taste much better (I’m told – I don’t drink coffee personally) and you won’t get an insulin spike 2-3 hours later and begin craving more coffee and donuts.
Fifth on my list is coffee creamer. Coffee creamer contains corn syrup solids (another very special name for . . . SUGAR!!) and/or maltodextrin (SUGAR’s married name!). If you must put something in your coffee, then use real heavy cream (pure tasty fat) or real butter. It will taste much better (I’m told – I don’t drink coffee personally) and you won’t get an insulin spike 2-3 hours later and begin craving more coffee and donuts.
Yes, “Half & Half” is half fat and half sugar. . . avoid it too!!
Ketosis Killing Medications
The sixth culprit in halting weight loss is medications. Please talk to your doctor before making ANY changes in your medications as suddently stopping them can be hazardous to your health. Those highest on my list for stopping your weight loss are Glyburide (glipizide), insulin, & steroids like prednisone. A more complete list of medications that will halt your weight loss can be found on my on my ketogenic diet plan. If you are on any prescription medications, please talk to your doctor or to a physician board certified in obesity medicine treatment about how to adjust or wean these medications in a way that is safe and appropriate for your individual needs.
Estrogen
The seventh common culprit in halting weight loss is a lack of estrogen in menopausal or post-menopausal women. About  20% of women that I see in my practice who are over 55 years old, need some degree of estrogen replacement before they are able to lose weight. Estrogen plays a very large role in regulation of the metabolism and when deficient, causes weight retention or weight gain. Talk to your doctor about the risks and benefits of estrogen for you individually in this situation.
20% of women that I see in my practice who are over 55 years old, need some degree of estrogen replacement before they are able to lose weight. Estrogen plays a very large role in regulation of the metabolism and when deficient, causes weight retention or weight gain. Talk to your doctor about the risks and benefits of estrogen for you individually in this situation.
Stress
The eighth reason for shifting out of ketosis is stress. Acute and chronic stress can be caused by a number of issues. The most common is lack of sleep. You can read about stress and ways to address it in two of my articles: How Does Stress Cause Weight Gain? and Adrenal Insufficiency, Adrenal Fatigue and PseudoCushing’s Syndrome – Oh My!
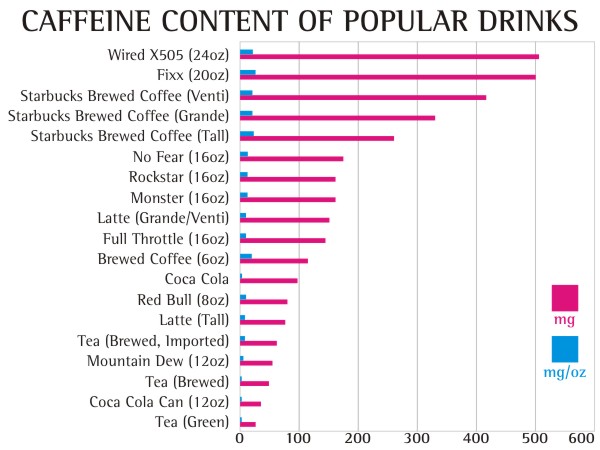
For many years, we’ve thought that caffeine was great for weight loss. However, we are finding, clinically, that too much caffeine can also cause a stress response by raising cortisol, releasing glycogen, thereby stimulating an insulin response and bringing your weight loss to a screeching halt. How much caffeine? . . . The jury is still out . . . and remains to be determined. But, I am currently under going an n=1 experiment on myself (as many of you know, I loved Diet Dr. Pepper. But I had to give it up). I’ll keep you posted . . .
Look closely at these eight issues. Correcting them usually solves most plateaus with weight loss and improves blood pressure, blood sugar and cholesterol control dramatically.














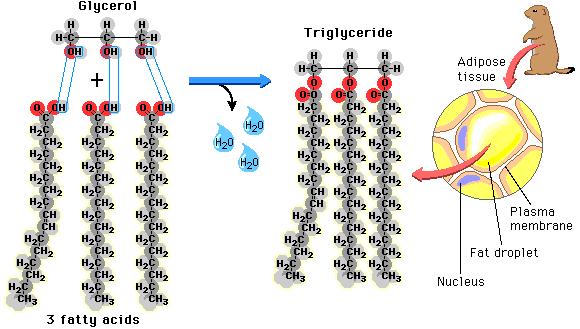 as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
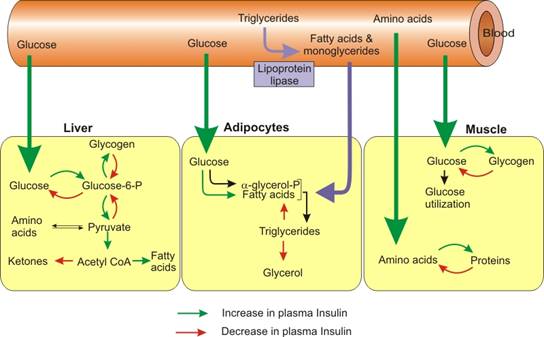 before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).
before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3). After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the
After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the 





















{kind=link}