I hear this all the time. “I can’t eat keto because. . . ”
What is your excuse?
I am amazed at how tightly people cling to these excuses. They are just that excuses. In the 16 years I’ve been training people how to use these diets to treat disease, I have yet to find one that is not just an excuse that covers up the real reason . . .
One of the common complaints that I see in my office is chronic numbness and tingling of the hands, fingers, feet & toes. There are multiple causes of these symptoms, but by far the most common cause in my practice is polyneuropathy caused by insulin resistance (hyperinsulinemia).
Before we dive into this particular type of nephropathy, it is important that we define a few terms. The terms “polyneuropathy,” “peripheral neuropathy,” and “neuropathy” are frequently used interchangeably, and although they can be easily confused, they are distinctly different.
Definitions
Polyneuropathy is a specific term that refers to a generalized sensation of tingling or numbness that uniformly affects many nerves at the peripheral sites (ends of the extremities like hands, fingers, lower legs, feet and toes).
Peripheral neuropathy is a less precise term. It is frequently used synonymously with polyneuropathy, but can also refer to any disorder of the peripheral nervous system. However, this term includes pain or numbness that radiates from nerve roots like “sciatica” of the leg and “brachial plexopathy” causing symptoms in one hand and/or arm (mononeuropathies).
Neuropathy, which again is frequently used interchangeably with peripheral neuropathy and/or polyneuropathy, can refer even more generally to disorders of the central (brain & spinal cord) and peripheral nervous system (nerves of the arms and legs) and their connections to sensory organs, such as the eye and ear, and to other organs of the body, muscles, blood vessels, and glands.
Why spend time defining all this? Because, neuropathy can be very confusing, even for the experienced physician. And, because I am seeing, more and more frequently, cases of insulin resistance induced polyneuropathy. The polyneuropathies must be distinguished from other diseases of the peripheral nervous system, including the mononeuropathies and mononeuropathy multiplex (multifocal neuropathy), and from disorders of the central nervous system.
Mononeuropathy refers to focused involvement of a single nerve, usually due to a localized trauma, compression, or nerve entrapment. Carpal tunnel syndrome is a common example of a mononeuropathy. Sciatica due to a lumbar disc bulge is another form of mononeuropathy.
Mononeuropathy multiplex refers to simultaneous involvement of non-adjoining sections of nerve trunks. Used loosely, this term can refer to multiple compressive mononeuropathies. However, in its more specific meaning, it identifies trauma, infection, auto-immunity or damage to multiple nerves outside the central nervous system. This is often due to lack of blood supply due to disease based inflammation of blood vessels supplying blood to these peripheral nerves.
Diseases of the central nervous system such as a brain tumor, stroke, or spinal cord lesion occasionally present with symptoms that are difficult to distinguish from polyneuropathy.
Insulin Resistance and Neuropathy
Insulin resistance, or better defined hyperinsulinemia, begins 10-15 years before a person is considered “pre-diabetic” and 20 years before the onset of type II diabetes. This “over production of insulin” in response to carbohydrates, starches and sugars causes a subtle and progressive form of inflammation. This excessive production of insulin will damage the smallest arteries (capillaries) carrying oxygen and fuel to the back of the eyes, the kidneys and the peripheral nerves of the hands, fingers, lower legs, feet and toes.
Often not identified until a person is actually diabetic, the mechanism underlying the development of this type of neuropathy is extremely complex. It is driven by years of subtle and progressive damage to the blood vessels, and inability of the nerves to use essential B vitamins damaging the genetics of the cell. This leads to inflammatory, metabolic, and ischemic effects causing the nerves to function poorly over time.
What Causes Polyneuropathy?
The mechanism of polyneuropathy damage in the patient with hyperinsulinemia three-fold.
The presence of high insulin stimulates increased fat storage. As fat cells begin to get filled, they begin to over-produce a number of inflammatory hormones including TNF-alpha, IL-6, IL-1, Adiponectin, Leptin and Resistin. These inflammatory hormones turn on auto-immunities and abnormal immune system function.
At the same time, the high insulin levels suppress appropriate testosterone and estrogen production causing microscopic damage to the lining of the smallest arteries and capillaries of the body (found predominantly at the extremities, kidneys and back of the eyes).
65% of patients with insulin resistance (hyperinsulinemia) have a malformation of one or both genes that encode the MTHFR enzyme (methylenetetrahydrofolate reductase) that uses folic acid (Vitamin B9) inside the cells of the body. Because this is genetic and is a process occurring inside the cell, it has been difficult to identify until recent advances in measuring genetic SNPs. Single nucleotide polymorphisms, frequently called SNPs (pronounced “snips”), are the most common type of genetic variation among people.
Interestingly, MTHFR deficiencies are also strongly correlated with depression, anxiety and other forms of mental illness. MTHFR is a SNP that can easily be tested through a simple blood sample at your local lab or doctors office. And, nerve testing can be done through a simple sudomotor function test in the doctors office. In fact, Medicare encourages this testing yearly through part of the Annual Wellness Exam.
The polyneuropathy that I see most commonly in my office can and will improve. In fact, polyneuropathy will completely resolve if you catch it early enough. We treat it in two ways.
What Can I Do To Treat Polyneuropathy?
First, restrict carbohydrate intake. A ketogenic or carnivore diet is the perfect approach to this. If you don’t have a copy of my book, The KetoCure, please pick one up on my website or on Amazon. if you are just looking to fine tune the nuts and bolts of your diet, you can get a copy of my diet recommendations here. Carbohydrate restriction corrects the high insulin levels. Within a few weeks, people start seeing improvement in inflammation, testosterone, estrogen and leptin resistance.
Second, get your MTHFR SNPs tested. This can be ordered through a simple blood test through your doctor or nearby lab. If you have one or both MTHFR mutations, treatment is simple. A mutation of the MTHFR SNP directly causes polyneuropathy, anxiety, depression and in severe cases, schizophrenia. It can also cause significant problems with homocysteine metabolism and is a significant risk factor in heart disease.
Third, use the correct form of folic acid. If you have the MTHFR mutation, regular folic acid is ineffective. Instead of using regular folic acid (Vitamin B9), 1000-5000mcg per day of L-methyl folate (premethylated Vitamin B9) solves the problem. Within 90 days, over 50% of my patients feel dramatic improvement in their neuropathy and many have compete resolution of the numbness and tingling. I see this so frequently, that a few years ago I had my multivitamins designed to include L-methyl folate instead of regular folic acid. You can find them here at Ketoliving. com. If you want more information on why I designed my own vitamin supplement a few years ago, you can read about them here.
So, restrict your carbs, use the appropriate form of folic acid for you, and pass the bacon!
If you are interested in getting more help on this issue, schedule an appointment with me in my office. Or, consider one of my membership options if seeing me in my office isn’t convenient for you. Sign up today!
References:
Yigit, Serbulent et al. “Association of MTHFR gene C677T mutation with diabetic peripheral neuropathy and diabetic retinopathy.” Molecular vision 19 1626-30. 25 Jul. 2013.
Wan, Lin et al. “Methylenetetrahydrofolate reductase and psychiatric diseases.” Translational psychiatry 8,1 242. 5 Nov. 2018, doi:10.1038/s41398-018-0276-6.
Shelton, Richard C et al. “Assessing Effects of l-Methylfolate in Depression Management: Results of a Real-World Patient Experience Trial.” The primary care companion for CNS disorders 15,4 (2013): PCC.13m01520. doi:10.4088/PCC.13m01520.
Hughes R. Investigation of peripheral neuropathy. BMJ 2010; 341:c6100.
Morrison B, Chaudhry V. Medication, toxic, and vitamin-related neuropathies. Continuum (Minneap Minn) 2012; 18:139.
Pareyson D, Piscosquito G, Moroni I, et al. Peripheral neuropathy in mitochondrial disorders. Lancet Neurol 2013; 12:1011.
Rutkove SB, et al., Overview of Polyneuropathy. UpToDate.com. Online Jan 2020, https://www.uptodate.com/contents/overview-of-polyneuropathy?search=neuropathy&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1
Will a ketogenic diet or very low carbohydrate diet kill you? Will it increase your likelyhood of death? That’s what the media and the dietary world is saying this week. Is it really true? How do you know? That’s the question that I ponder as I smoke my brisket while reading the headlines this week.
My inbox has exploded with patients and acquaintances suddenly worried that my very low-carb lifestyle is bad. This all revolves around the publishing of a study in the Lancet this week, and the interpretative spin that has been placed on it by “those in the know.” To quote one of the NHS dietitians, Catherine Collins, RD FBDA, “In summary, this paper will disappoint those who, from professional experience, will continue to defend their low-carb cult, but contributes to the overwhelming body of evidence that supports a balanced approach to calorie intake recommended globally by public health bodies.” Either she didn’t actually read the paper, or she clearly doesn’t understand the low-carbohydrate/ketogenic dietary world. Before you go throwing out your bacon, turning off my smoker and buying bags of rice, let’s talk about some principles that seem to be completely misunderstood by the “low-fat, calorie restricting” nutritional aristocracy.
Ketogenic Diets are Powerfully Effective
First, ketogenic diets are powerfully effective. They are effective in weight loss, reduction of blood sugar, reversal of diabetes, decreasing cardiovascular risk and reduction in blood pressure. These are just a few of the powerful effects of a ketogenic lifestyle. (I wrote a whole book on the 16 different diseases dramatically improved by carbohydrate restriction.) It’s why I’ve been using carbohydrate restriction for over 14 years both personally and in my clinical practice. 85% of the people in my practice don’t respond effectively to anything other than carbohydrate restriction. This is because their insulin levels are 2-20 times normal. The question the Lancet should be asking is “why do 85% of people fail calorie restriction?” But, that is for another article.
Few Diets Keep the Weight Off Long-Term
Does the ketogenic diet keep weight off in the long term? All diets seem to fail in this regard, even the ketogenic diet will show rebounding of weight after 1-2 years. Yes, I hate to be the bearer of sour news, but as an obesity specialist, this is what I do for a living. The Lancet article implies that the low-carb diet is singular in the issue of weight rebound, but that is not the case. The only diet I have found to effectively keep the weight off long-term is a ketogenic diet, combined with pulsed eating and the correct type of physical activity.
Definition of a Very Low-Carbohydrate Diet
Third, commentary, and the researchers themselves, extrapolate that based on the results, very low carbohydrate diets increase the risk of mortality. However, this study wasn’t even “low-carb.” It was Paleolithic at best. The lowest calorie intake group was just under 1600 kcal per day and the carbohydrate restriction was only 120 grams per day. A low-carb diet is defined as less than 100 grams per day. A very low-carbohydrate diet is defined as less than 50 grams per day, and a ketogenic diet is defined as less than 20 grams per day. This study and the cohort studies involved in it weren’t even low-carb!!!
Only Two Data Gathering Points in 25 Years?
Fourth, although people were followed for 25 years, there were only two data gathering points consisting of 66 questions spaced 5-7 years apart asking the 15,428 participants to “remember what they ate” over previous 3-5-year intervals. Seriously?! I can barely remember what I ate last week and I take pictures of my food and journal my meals frequently. How can you publish an article with only two data collection points over 25 years? And, how can extrapolated data over 25 years be accepted as valid in a premier medical journal? It is beyond my understanding.
You Gotta Lower Insulin to Reduce Mortality
Fifth, insulin must be lowered to a “baseline level.” Increasing fat intake in the presence of abnormally elevated insulin will actually increase risk of cardiovascular disease, peripheral vascular disease, diabetes, hypertension, gout, kidney stones, and death by multiple causes. This cohort of people only partially lowered carbohydrate intake, and raised fat and or protein intake. Those of us who’ve been treating obesity and practicing in the trenches are well aware that if you don’t bring the insulin levels under control, raising fat and protein is just a ticking time bomb. Of course, the all-cause mortality went up in this group. I’d expect nothing less. This is what I saw with a large portion of my Paleolithic dietary patients.
This is also why caloric restriction doesn’t work. These participants had average calorie restriction of 1600-1800 kcal per day. Yet their risk for all-cause mortality (death by all causes) increased.
Weight Gain Continued
Sixth, all of the groups continued to gain weight. Body mass index increased by almost a full point ever 6 years. Carbohydrates were NOT restricted enough to be effective. It also, demonstrates another example of calorie restriction failure in 15,000 plus people.
That’s what I’d call successful – not really!
Smokers Not Excluded
To make matters worse, 60-70% of the population were smokers or former smokers and this study did not specifically eliminate this as a risk factor for all-cause mortality. We know that smoking dramatically increases risk of heart disease, peripheral vascular disease, hypertension, stroke, lung cancer, chronic obstructive pulmonary disease, etc. The contribution of tobacco in this cohort was not adequately isolated.
The World Health Organization has developed sixteen goals as their “Call to Arms.” Goals 12 and 13 specifically discuss “ensuring sustainable food consumption patterns throughout the world.” These goals specifically outline a transformational vision of the world. This will occur by “doubling agricultural growth” and restricting food production that worsens the “carbon footprint.”
Really?!
Over the last ten years, multiple progressive groups and sites have made the claim that the greatest threat to Climate Change is the cattle industry. They link cattle, livestock and our consumption of red meats to global warming and have been preaching the politics of nutrition. They claim that the only real way to stop climate change and global warming is to “eat less red meat and dairy products.”
Low-carbohydrate and ketogenic diets are a threat to this transformational vision. Because of this, we will likely see more and more scientific research used as propaganda, let’s call it what it is, to sway the general populous in their buying and eating patterns.
So, if you’ll excuse me, my smoked brisket is ready to pull off the smoker. . .
I get asked this question all the time. And, my answer is that 85% of the people that walk through the doors of my clinic will not be fully successful in weight loss, reversal of diabetes, normalization of blood pressure and reversal of heart disease and/or vascular disease without it.
I am frequently asked, “Is Keto for everyone?” Does everyone need to follow a ketogenic lifestyle? The answer is “No.” 15% of the population will be able to maintain great health with calorie restriction and exercise. However, the principles that provide a successful ketogenic lifestyle are easily understood and incorporated by anyone looking for improved health, energy and weight control.
Principle #1 – Insulin is the Master Hormone
Insulin is the master hormone when it comes to weight loss and the diseases of civilization. Whether you are insulin resistant or not, insulin is essential for life and proper function of the cells of the body, but too much insulin production in response to sugars, starches or complex carbohydrates causes disease.
How do you know if you are insulin resistant (producing too much insulin)?
Skin tags are pathognomonic (a characteristic indicative of the presence of disease) for insulin resistance. If you have skin tags, you may want to focus your diet on increased carbohydrate restriction.
You may not need to completely remove carbohydrate from your diet, however, recognizing that not all carbohydrates are created equal and avoiding those with higher carbohydrate content will help many improve weight and halt the progression of disease. I have many patients that with just partial carbohydrate restriction they are able to lose 20-30 lbs, improve their cholesterol profiles and improve their blood pressure.
There are sixteen different diseases that respond very effectively to carbohydrate restriction. You can read about them and how the ketogenic lifestyle effectively reverses them in The Keto Cure.
Principle #2 – Saturated Fat & Cholesterol Aren’t the Demons We’ve Made Them Out to Be
Saturated Fat and cholesterol aren’t the demons we’ve made them out to be. Another way to put it is: “Don’t blame the butter for what the bread did.”
Since 1984, nutrition experts treat fat and cholesterol containing foods like the witches of Salem. Experts castigate their use as if they were the “Avada Kedavra“ curse of the fantasy world.
As an example, eggs, specifically the egg yolk (the part of the egg containing all the cholesterol and saturated fat), have been demonized by just about every health magazine I’ve ever read. (To this day, the chef at every breakfast bar I’ve ever visited asks if I want an ‘egg white only’ omelet.) Interestingly, there is actually no scientific data association between whole egg consumption and heart disease. The science simply does not exist. Seriously, check for yourself.
I personally eat 6-8 eggs a day and my cholesterol is perfect. Back 1000 years ago, only the aristocrats at the chickens. All laborers and serfs ate the eggs . . . who would be dumb enough to eat your food source? (Don’t answer that.)
For example, the MR-FIT study, the largest cholesterol study ever completed, is incessantly quoted as the study that demonstrates reduction in cholesterol leads to reduction in cardiovascular disease, but this trial was actually a failure and did not demonstrate improved risk by lowering cholesterol. In fact, the Director of the study, Dr. William Castelli stated, “. . . the more saturated fat one ate, the more cholesterol one ate, the more calories one ate, the lower people’s serum cholesterol…”
Researchers found that people who ate the most cholesterol, including the most saturated fat, weighed the least. They were also the most physically active. In fact, the British Medical Journal published a 2015 study demonstrating that saturated fat is NOT linked to vascular disease, diabetes or increased mortality (de Souza RJ et al., BMJ 2015,351:h3978).
In my clinic, the basis of appetite suppression is eating adequate protein that includes saturated fat and cholesterol. This is the most powerful tool in my clinical approach to the treatment of weight loss. I can use foods like red meat, bacon, butter and coconut oil without concern or worry of heart disease as long as you are keeping your carbohydrate intake less than 20 grams per day.
Baseline insulin levels allow for peace of mind about heart disease risk. Heart disease risk goes down when insulin levels are maintained at normal baseline levels. Increasing saturated fat, while at the same time lowering carbohydrate intake has been demonstrated to shift the cholesterol to a more heart protective form (Griffin BA et al., Clin Sci [Lond], 1999 Sep).
Principle #3 – Nutritional Ketosis Has Anti-Inflammatory & Age Slowing Effects On the Body
Ketones in the blood at a nutritional level (0.5-4 mmol/L) have tremendous anti-inflammatory and age slowing effects on the body. Even having them present intermittently has dramatic improvement on overall inflammatory changes and disease in the body.
Ketones are the usable fuel of the body when the liver breaks down fat for energy. They suppress the NLRP3 inflammasome in every cell in the body. This is important because it allows for more rapid recovery from exercise. It also dramatically decreases pain and fatigue that comes from diseases like arthritis, rheumatoid arthritis, multiple sclerosis and auto-immune disease (Y.H. Youm, et al., Nature Medicine, vol. 21, no. 3, pp. 263–269, 2015.)
If full blown ketosis isn’t for you, partially restrict starch and carbohydrates for a mild to moderate benefit. Even small amounts of ketones in the blood are helpful. This provides increased recovery time, and improved inflammation control.
So, even if you don’t follow a strict ketogenic lifestyle, the principles above are powerful. These three principles make this dietary approach universally effective for weight loss. They are also very powerful for disease management. Even partial application of carbohydrate restriction can benefit just about everyone.
You can learn much much more about the Ketogenic Lifestyle as a member of DocMuscles.com. Click the link and sign up now.
And, don’t forget to get your signed copy of my book, The Keto Cure.
Listen in to Ketotalk Podcast #19 where we talk about inflammatory foods, building muscle with a ketogenic diet & how ketosis affects the Baby Boomer Generation.
Keto Talk is cohosted by 10-year veteran health podcaster and international bestselling author Jimmy Moore from “Livin’ La Vida Low-Carb” and Arizona Osteopath and Board Certified Obesity Medicine physician Dr. Adam Nally from “Doc Muscles” who thoroughly share from their wealth of experience on the ketogenic lifestyle each and every Thursday.
We love hearing from our fabulous Ketonian listeners with new questions–send an email to Jimmy at livinlowcarbman@charter.net. And if you’re not already subscribed to the podcast on iTunes and listened to the past episodes, then you can do that and leave a review HERE. Listen in today as Jimmy and Adam answer more engaging questions about nutritional ketosis from you the listeners.
On this evenings PeriScope video we talked about cholesterol. And, and you can see an updated, in depth discussion about cholesterol on my YouTube channel here. Please go check it out and if you find it helpful, please follow me here and on YouTube. The is the burning question on everyone’s mind who starts a Low-Carb, High Fat or Ketogenic Diet: “What will happen to my cholesterol if I lower my carbohydrates and eat more fat?”
The answer . . . it will improve!
How do I know this? I’m an obesity specialist. I specialize in FAT or lipids (to put it kinder scientific terms). To specialize in fat, one must know where it came from, what it’s made of and where it is going. And, this has been the case with every single patient I have used this dietary change with for the last ten years, myself included.
Lets start with the contents of the standard cholesterol or “Lipid Panel”:
Total Cholesterol
HDL-C (the calculated number for “good” cholesterol)
LDL-C (the calculated number for “bad” cholesterol).
Triglycerides
The first problem with this panel is that it makes you believe that there are four different forms of cholesterol. NOT TRUE! Actually cholesterol is cholesterol, but it comes in different sizes based on what it’s function is at that moment in time. Think of cholesterol as a bus. There are bigger busses and smaller busses. Second, triglyceride is actually the passenger inside the HDL and the LDL busses. And third, Total Cholesterol is the sum of the HDL, LDL, as well as ILDL & VLDL which aren’t reported in the “Lipid Panel” above.
The fourth thing that this panel doesn’t tell you is that HDL & LDL are actually made up of sub-types or sub-particles and are further differentiated by weight and size.
For our conversation, we need to know that the number of LDL particles (LDL-P) can actually be measured in four different ways and these measurements have identifed that there are three sub-types: “Big fluffy” large dense LDL, medium dense LDL, and small-dense LDL. Research has identified that increased numbers of small-dense LDL correlates closely with risk for inflammation, heart disease and vascular disease (1).
If you’ve been a follower of my blog for a while, you’ve seen this picture before. This picture illustrates why an LDL-C (the bad cholesterol measurement) can be misleading. Both sides of the scale reflect an LDL-C of 130 mg./dl. However, the LEFT side is made up of only a few large fluffy LDL particles (this is the person with reduced risk for heart disease) called Pattern A or a LDL healthy cholesterol level. Even though the LDL-C is elevate above the recommended level of 100 mg/dl, the patient on the left has much less risk for vascular disease (this is why you CAN’T trust LDL-C as a risk factor).
The RIGHT side of the scale shows that the same 130 mg/dl of LDL-C is made up of man more small dense LDL particles (called “sd LDL-P”) with a Pattern B type that is as increased risk for heart or vascular disease. This is where the standard Lipid Panel above, fails to identify heart disease and it’s progression.
Research tells us that the small dense LDL particle levels increase as the triglycerides increase. And we know that Triglyceride levels increase in the presence of higher levels of insulin leading to a cascade of inflammatory changes. Insulin is directly increased by the ingestion of simple and complex carbohydrates. Insulin also increases with the ingestion of too much protein. So, that chicken salad or the oatmeal you ate, thinking it was good for you, actually just raised your cholesterol. If you are insulin resistant, your cholesterol just increased by 2-10 times the normal level (see my article here on how insulin resistance causes this.)
“Ok, but Dr. Nally, there are four different companies out in the market measuring these fractional forms of cholesterol. Which one should I choose?”
There are actually five different ways you can check your risk.
Apolipoprotein levels. This can be done through most labs; however, this test doesn’t give you additional information on insulin resistance that the other tests can.
Berkley Heart Lab’s Gradient Gel Electrophoresis – This test gives a differentiation based on particle estimation between Pattern A and Pattern B
Vertical Auto Profile (VAP-II) test by Arthrotec – This test determines predominant LDL size but does not give a quantifiable lipoprotein particle number which I find very useful in monitoring progression of insulin resistance and inflammation.
NMR Spectroscopy from LipoScience – This test measures actual lipoprotein particle number as well as insulin resistance scores and will add the Lp(a) if requested. I find the NMR to be the most user friendly test and useful clinically in monitoring cholesterol, vascular risk, insulin resistance progression and control of the inflammation caused by diabetes. This test has the least variation based on collection methods if frozen storage is used.
Ion-Mobility from Quest – This test also measures lipoprotein particle number but does not include insulin resistance risk or scoring. Because the test is done through a gas-phase electric differential, the reference ranges for normal are slightly different from the NMR.
In regards to screening for cardiovascular risk, the use of all five approaches are more effective than the standard lipid panel. However, I have found that clinically the NMR Lipo-profile or the Cardio I-Q Ion-Mobility tests are the most useful in additionally monitoring insulin resistance, inflammation, and disease progression.
It is was the use of these tests that demonstrated to me the profound effect of carbohydrate restriction and ketogenic lifestyles on vascular and metabolic risk. We talk more about these tests on my YouTube video .
Hope this helps.
References:
Williams PT, et al. Comparison of four methods of analysis of lipoprotein particle subfractions for their association with angiographic progression of coronary artery disease. Atherosclerosis. 2014 April; 233(2): 713-720.
Ketogenic Lifestyle Rule #2: Life Begins at the Edge of Your Comfort Zone
We have been taught for over 50 years that the minimum carbohydrate intake necessary to maintain health is 130 grams per day, with the average diet of 2000 calories per day containing around 300 grams per day based on 1977 recommendations that 55-60% of are dietary intake should come from carbohydrates. This value was initially established during World War II by a committee of scientists tasked with determining dietary changes that might effect national defense (1). These “guidelines,” originally called the Recommended Daily Allowances (RDA) and accepted by many as the gospel truth, have been modified every ten years and in 1997 changed to the Dietary Reference Intake (DRI). However, the recommended carbohydrate values have not changed other than “avoiding added sugars” in the most recent 2015 recommendations.
In light of the fact that there are NO actual diseases caused by lack of carbohydrate intake, most dietitians and physicians still preach the carbohydrate dogma originally outlined by the RDA. I say dogma, because these recommendations are based on a diet that vilifies fat, particularly animal fat like red meat. Say the words “red meat” around a dietician these days you’d think Voldemort (“He Who Shall Not Be Named”) had returned.
I bring up the carbohydrate quandary because it is a question that I am asked every single day. The question that seems to be asked of me, more and more, is what exactly is a carbohydrate?
Let’s make it simple. There are really only three types of carbohydrates:
Sugar
Starch (known as complex carbohydrates)
Fiber
Let’s start with Sugar. The simple form of carbohydrates, and the form that spikes your blood sugar and insulin rapidly, are called mono-saccharides (glucose, galactose, fructose & xylose). When two of these mono-saccharides are bound together they form disaccharides like sucrose, also known as “table sugar” (glucose + fructose), lactose found in milk (glucose + galactose), and maltose found in cereals and sweet potatoes (glucose + glucose).
Milk Sugar or Lactose (glucose + glucose)
The simple monosaccharides or disaccharides are easy broken into their mono-saccharide form in the blood stream and require the body to produce insulin to be used. The person with insulin resistance, impaired fasting glucose or type II diabetes often produces 2-10 times the normal amount of insulin to correctly use these mono-saccharides (see why this is a problem in: The Dreaded Seven: Seven Detrimental Things Caused By High Insulin Levels). Remember, fruit is also simple sugar containing the mono-saccharide fructose . . . which we call “natures candy” in my office.
“Yea, I know sugar is bad for me, but Dr. Nally, I just eat the good starches.”
If I had a nickel for every time I’ve herd that phrase . . .
We’ve become comfortable with shunning fat and “simple sugar,” but in the process we’ve been eating more “good starch.” But the “good starches” are also saccharides – just in longer chains of more than three glucose molecules bound together. Our gut easily breaks the bonds between the glucose links and turns these starches into mono-saccharides to be used as fuel. It takes a bit longer than the simple sugars above, so the release of insulin is slower (which is why it has a better glycemic index score), but whether you produce the insulin in the first hour or the second hour after eating it, insulin is still insulin. In the case of insulin resistance, the damage is still done.
These good starches make up “comfort food” like bread, rice, pasta, potatoes, corn, grains & oats. To the patient with insulin resistance, impaired fasting glucose or type II diabetes, the higher insulin response stimulates increased weight gain, rise in cholesterol, shift in hormone function and progression of atherosclerosis (vascular and heart disease). See the recent article on Why Your Oatmeal is Killing Your Libedo.
What about “resistance starches?” These are still starches and I am finding clinically that they still cause a rise in insulin and push people out of ketosis (See Common Ketosis Killers).
Finally, Fiber. Fiber is a carbohydrate, however, it is the indigestible part of the plant. Fiber has double bonds between the saccharides that human gastrointestinal tracts cannot digest. In most cases, fiber passes right through the intestines without being digested. It actually acts like a broom for your colon, helping the intestines to move nutrients through the system. This is why I recommend 1-2 leafy green salads a day for most patient’s following ketogenic diet. Fiber does help to promote bowel function.
The Leafy Greens
Fruit, non-green vegetables, pasta, grains and breads do contain good sources of fiber, however, these foods also have absorbable starches making them problematic as noted above.
The take home message is this, the use of starch or simple carbohydrate will be problematic for weight loss, cholesterol control, blood sugar control or blood pressure control in a patient with insulin resistance.
Therefore, the ketogenic lifestyle truly begins at the end of your comfort zone.
I am frequently asked about the sweeteners that can be used with a low carbohydrate diet. There are a number of sweeteners available that are used in “LowCarb” pre-processed foods like shakes or bars, or in cooking as alternatives to sugar; however, many of them raise insulin levels without raising blood sugar and are not appropriate for use with a true low-carbohydrate/ketogenic diet. You can see and print the article I published clarifying which sweeteners you can use and which ones to avoid in the menu bar above “Sour Truth About Sweeteners” and you can watch last night’s periscope below:
Good morning from Arizona. I’ve had a few people ask about how gut health relates to a ketogenic diet. This is a great question and one that I think can be answered best by taking a closer look at my natural koi pond and learning a little about pond scum.
So, sit back and look at the similaries between your gut and how nature balances a pond system: Katch.me
Or you can watch the video below:
The four tenets of health that we touch on above that are essential to understand before you can understand gut health:
The body is a unit and works as such with all parts enhancing the whole
The body is capable of self-regulation, self-healing, and health-maintenance
Structure & function are reciprocally interrelated
Rational treatment of the body must be based upon understanding the principles above and assisting or augmenting those principles
Keys to gut health and pond balancing that we touch on:
Remove the toxins from entering the system like:
Antibiotic overuse
Caffeine
Artificial Fat
Artificial Sweeteners
Repair the system and it’s ability to balance the system
Takes time
Provide structure for the bacteria to which it can bind
Provide essential vitamins and minerals like KetoEnhance & Omega-3 fatty acids
Periodic Fasting
Restore the bacteria or flora of the system
Prebiotics (fermented foods like sauerkraut, kimchi, Japanese natto, etc.)
Probiotics like Dietary KetoBalance (can be purchased in the office)
Replace the salts and pH balance where necessary
Replace electrolytes
Limit things that shift the pH balance
Hope this gives you a starting point for your New Year!!
Let me answer that question with the following questions:
Do you find yourself longing for the apocalypse?
Do you find yourself looking for a reason to live?
Are you feeling tired, irritable, stressed out?
Do you or you family find yourself to be overly cynical, jaded or emotionally numb?
If you can answer “yes” to any of the questions above, then I highly recommend prescription strength nature . . .
All parody and humor aside, full strength prescription nature is one of the very best treatments for stress.
I find that sitting outside with my animals, watching the birds, dogs, horses and ducks dramatically helps with lowering my stress levels and helps me re-focus. You can see my favorite place to sit on my farm and watch nature . . . here on Katch.me
You may find the following posts very insightful in explaining how stress wreaks havoc on your weight loss, mood & emotions and how to go about fixing it:
For someone like me, who spends 14-18 hours a day taking care of illness and sickness, I have found that spending time in nature is often more therapeutic than any pill available in the pharmacy. So, this afternoon, if your looking for me, I’ll be taking my own medicine, a prescription of Nature Rx on my horse.
Today’s Periscope was an exciting one. Do you really need a pre- or post-workout shake or meal? How much protein do you need? What’s the difference between ketosis and ketoacidosis? Is Dr. Nally a ketogenic cheerleader? Get your answers to these and many more questions asked by some wonderful viewers this evening on today’s PeriScope.
Be sure to check out Dr. Nally’s new podcast called “KetoTalk with Jimmy and the Doc” with the veteran podcaster Jimmy Moore on KetoTalk.com. The first podcast will be available on December 31, 2015. KetoTalk with Jimmy and the Doc will be available for download for free on iTunes.
I’ve been looking for the answer for quite some time. . . what role does caffeine play in your and my weight management journey? The answer gave me a headache. . . literally and figuratively.
As many of you, including my office staff, know, I love my Diet Dr. Pepper (and my bacon). I found that being able to sip on a little soda throughout the day significantly helped the carbohydrate cravings and munchies during a busy and stressful day at the office. Diet Dr. Pepper contains caffeine, however, I wasn’t really worried. Caffeine has been well know to have a thermogenic effect which increases your metabolism and has been thought for many years to help with weight loss among the weight loss community.
Diet Dr. Pepper is, also, one of only four diet sodas on the grocery store shelves that doesn’t contain acesulfame potassium (click here to see why most artificial sweeteners cause weight gain). The four diet sodas that I have been comfortable with my patients using are Diet Dr. Pepper, Diet Coke, Diet Mug Root-beer and Diet A&W Cream Soda. These are the last four hold out diet sodas that still use NutraSweet (aspartame) as the sweetener. Most of the soda companies have switched the sweetener in their diet sodas to the insulinogenic acesulfame potassium because it tastes more natural and aspartame has been given a media black eye of late. However, NutraSweet (aspartame) is the only sweetener that doesn’t spike your insulin or raise blood sugar (click here to find out why that is important).
Yes, I know. The ingestion of 600 times the approved amount of aspartame causes blindness in lab rats (but we’re not lab rats, and . . . have you ever met someone that drinks 600 Diet Dr. Peppers in a day? The lethal dose of bananas, which are high in potassium that will stop your heart, is 400). Aspartame can also exacerbate headaches in some (about 5% of people) and I’ve had a few patients with amplified fibromyalgia symptoms when they use aspartame. But for most of us, its a useful sweetener that doesn’t spike your insulin response, halting or causing weight gain.
But, over the last few years, I’ve noticed that increased amounts of Diet Dr. Pepper & Diet Coke seem to cause plateauing of weight and decreasing the ability to shift into ketosis, especially mine. I’ve also noticed (in my personal n=1 experimentation) that my ability to fast after using caffeine regularly seems to be less tolerable, causing headaches and fatigue 8-10 hours into the fast, symptoms that don’t seem to let up until eating. Through the process of elimination, caffeine seems to be the culprit.
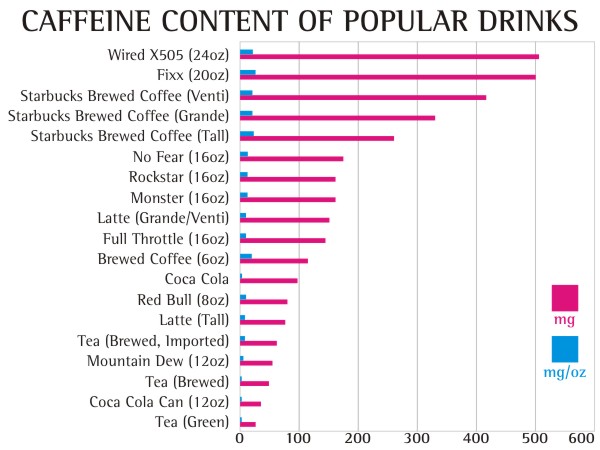
After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the August 2004 Diabetes Care Journal screamed for my attention.
It appears that caffeine actually stimulates a glucose and insulin response through a secondary mechanism. The insulin surge and glucose response is dramatically amplified in patients who are insulin resistant. Caffeine doesn’t effect glucose or insulin if taken while fasting; however, when taken with a meal, glucose responses are 21% higher than normal, and insulin responses are 48% higher in the insulin resistant patient. Caffeine seems to only effect the postprandial (2 hours after a meal) glucose and insulin levels. The literature shows mixed responses in patients when caffeine is in coffee or tea, probably due to the effect of other organic compounds (1).
Caffeine effect on plasma glucose and plasma insulin compared to placebo (1).
Caffeine also diminishes insulin sensitivity and impairs glucose tolerance in normal and already insulin resistant and/or obese patients. This is seen most prominently in patients with diabetes mellitus type II (stage IV insulin resistance). Caffeine causes alterations in glucose homeostasis by decreasing glucose uptake into skeletal muscle, thereby causing elevations in blood glucose concentration and causing an insulin release (2-6).
Studies show that caffeine causes a five fold increase in epinephrine and a smaller, but significant, norepinephrine release. The diminished insulin sensitivity and exaggerated insulin response appears to be mediated by a catacholamine (epinephrine, norepinephrine & dopamine) induced stress response (5). Caffeine has a half life of about 6 hours, that means the caffeine in your system could cause a catacholamine response for up to 72 hours depending upon the amount of caffeine you ingest (7).
The reason for my, and other patient’s, headaches and fatigue after a short fast was due to the exaggerated stress hormone response. Increased levels of insulin were induced by a catacholamine cascade after caffeine ingestion with a meal, dramatically more amplified in a person like me with insulin resistance. The caffeine with the last meal cause hypoglycemia 5-7 hours into the fasting, leading to headaches and fatigue that are only alleviated by eating.
Even when not fasting, the caffeine induced catacholamine cascade causes up to 48% more insulin release with a meal, halting weight loss and in some cases, causing weight gain.
Caffeine is not the “Wonder-Boy” we thought it was.
How much caffeine will cause these symptoms? 50 mg or more per day can have these effects.
10,000 mg (10 grams) – lethal dose (Yes, 25 cups of Starbucks Coffee can kill you)
The equivalent of 100 mg of in a human was given to a spider, you can see the very interesting effect on productivity. How often does the productivity of the day feel like the image below?
Normal Spider (9)Spider on caffeine (9)
Beware that caffeine is now being added to a number of skin care products including wrinkle creams and makeup. Yes, caffeine is absorbed through the skin, so check the ingredients on your skin care products.
Diet Dr. Pepper, my caffeine delivery system of choice, has slightly less caffeine (39 mg per 12 oz can or 3.25 mg per oz) than regular Dr. Pepper. I found myself drinking 2-3 liters of Diet Dr. Pepper per day (long 16-18 hour work days in the office). After doing my research, I realized that my caffeine tolerance had built up to quite a significant level (230-350 grams per day).
So, a few weeks ago, I quit . . . cold turkey.
Did I mention the 15 withdrawal symptoms of caffeine? (8)
Headache – behind the eyes to the back of the head
Sleepiness – can’t keep your eyes open kind of sleepiness
Irritability – everyone around you thinks you’ve become a bear
Lethargy – feels like your wearing a 70 lb lead vest
Constipation – do I really need to explain this one?
Depression – you may actually feel like giving up on life
Muscle Pain, Stiffness, Cramping – feel like you were run over by a train
Lack of Concentration – don’t plan on studying, doing your taxes or performing brain surgery during this period
Flu Like Illness – sinus pressure and stuffiness that just won’t clear
Insomnia – you feel sleepy, but you can’t sleep
Nausea & Vomiting – You may loose your appetite
Anxiety – amplified panic attacks or feeling like the sky is falling
Brain Fog – can’t hold coherent thoughts or difficulty with common tasks
I experienced 13 of the 15 that lasted for 4 days. I do not recommend quitting cold turkey unless you have a week off and someone to hold your hand, cook your meals and dose your Tylenol or Motrin. My wife thought I was dying. . . I thought I was dying on day two. I actually had a nightmare about buying and getting into my own coffin. It can take up to three weeks to completely recover from caffeine withdrawal.
The other way to quit is to decrease your caffeine intake by 50 mg every two days. That means decrease caffeine by:
1 can of soda every two days
1/4 cup of coffee every day
1/2 can of Energy Drinks every two days
1 cup of tea every two days
The benefit of this method is that withdrawal symptoms are much less severe without the caffeine headache and the ability to remain productive. It will take longer, but quitting cold turkey is not a pretty picture. Been there . . . done that, . . . and I’m not going back. I actually lost another half inch off my waistline by day 5 of caffeine discontinuation.
What is the take home message here? If you have any degree of insulin resistance, caffeine makes it worse and will amplify your weight gain as well as decrease the productivity of your day.
See this evenings PeriScope about things to expect in the first few weeks of a ketogenic or low-carb dietary change. Questions answered about carbohydrate restriction.
Recent research from Cornell University, recently published in Nature, reveals that increasing obesity leads to poor uptake of Vitamin A in the organ tissues of mammals including humans. Vitamin A (Retinol) is a key vitamin that helps in gene expression and regulation. Vitamin A uptake has been shown to diminish in obese patients and patient with hepatic steatosis [fatty liver disease or non-alcoholic fatty liver disease (NAFTL)].
This is a key finding and gives further evidence of the genetic expression of obesity and it’s effect on both the parent and the child. What is even more fascinating is that this appears to lead to alteration in immune response and changes in cellular differentiation in the human organs. This means that the Vitamin A deficiencies within the organs are being driven by fatty liver infiltration that is driven by insulin resistance. This Vitamin A deficiency cannot be detected with a blood test as serum levels of Vitamin A remain normal and has significant roll in masking the cause of autoimmunity function we are seeing more and more of throughout the world.
Metabolic effects of vitamins on the Immune System
So how do you get your Vitamin A in a ketogenic diet? Vitamin A can be found in meats (specifically liver and organ meats), eggs, butter, and cod liver oil. It can also be found in leafy greens, squash and peppers. The reduction in insulin production that occurs in a low-carb, ketogenic and even paleolithic diet reduces the fatty liver infiltration that arises with the standard American diet (SAD diet). Clinically, I have seen people reverse the steatosis of the liver within 12 months in my practice through carbohydrate restriction.
More research is needed, of course, but the take home message is that the ketogenic lifestyle plays an even greater roll in genetics and immunity than we ever thought. More to come . . . I’m sure.
You can see today’s periscope on this subject below . . .
or you can watch it here on Katch: https://www.katch.me/docmuscles/v/0f7b9835-1ac2-378e-a844-5647e86b700d
Ketogenic Lifestyle – the Balance of Endocrinology & Psychology
Over the last few weeks, I’ve had the pleasure of talking to a number of patients and friends about what it means to live a ketogenic lifestyle. A low-carbohydrate or ketogenic lifestyle is different from a low-carb diet. It is different because the definition of lifestyle implies the way a person lives their life that reflects specific attitudes and values, not just how they eat. My recent posts, The Principle Based Ketogenic Lifestyle – Part I and Ketogenic Principles – Part II, focus on fundamental principles making the ketogenic lifestyle one in which balance and grounding in all aspects of life can occur. When the mind, the body or the spirit are out of balance or un-grounded, symptoms of metabolic inefficiency, sickness or disease result.
I have been fascinated, as a family practitioner, that the body produces “warning flags,” when there is dysfunction in one of these areas: mind, body & spirit. These warning flags are byproducts of inefficient inter-related functionality between the body’s systems and it is one of the foundation principles of osteopathic medicine. Prior to the advent of many of our diagnostic techniques today like MRI, CT scan, advanced laboratory evaluations, and ultrasound, these were the only indicators of disease that a physician could identify, and upon which diagnosis was made. These flags often show up on the skin, in the hair or nails, in the complexion, or in general appearance or mannerisms.
Skin Tags (fibroepitheial polyps) under the arm
For example,”skin tags” are now recognized as pathognomonic, specifically indicative, of insulin resistance and will often occur up to 20 years before impaired fasting glucose or diabetes is ever recognized.
Exopthalmos (bulging or protruding of the eyes) from hyperthyroidism
Exopthalmos, or protrusion of the eyes, is pathognomonnic for overactive thyroid function (hyperthyroidism), and spider angiomas occur as a somatic flag that cirrhosis of the liver is present.
Alligator Skin (severe dry skin) found in hypothyroidism
Hair loss and dry skin, or “alligator skin,” represents the exact opposite with an under-active thyroid (hypothyroidism).
Spider angioma seen with cirrhosis
When metabolic pathways get “clogged” or flow of blood, lymphatic fluid or hormones do not reach the destinations they were meant to reach, symptoms of accumulation or poor function begin to arise.
The osteopath is also trained to recognize a corollary Chapman’s Reflex Points that act as flags for dysfunction in specific organs or regions of the body. These points relate directly to what causes the pathognomonic flag. I frequently identify abdominal, adrenal, pancreatic and liver Chapman’s points present in those with insulin resistance, inflammatory diseases, pre-diabetes and diabetes. Understanding how to interpret and use these flags comprises four years of medical school and three to four years of residency and often years of clinical application.
Mental or spiritual pathways can often be bloc-aided by poor recognition of, or refusal to acknowledge, individual truths in our lives. Interestingly, the signs or warning flags of spiritual dysfunction are also expressed physically.
“Oh, no?! Dr. Nally are you going to get all religious on us?”
Maybe.
Over the last 15 years of my medical practice, I’ve witnessed the spiritual component of the “mind, body, spirit” unit, or lack thereof, have profound impact on the body’s ability to heal. Every one of us must defeat what Sigmund Freud called the pleasure principle – the human instinct to seek pleasure and avoid pain, including recollections or memories that are painful. Hiding from these memories because of pain is very common and is part of human nature. We often believe that thinking about or re-living the truth may cause us individual overwhelming un-survivable grief. So, we naturally bury the thoughts and emotions and feelings deep down into our subconscious minds.
In fact, we take irrational risks, busy ourselves, use food or drink for short term comfort and move from one distracting or debilitating relationship to another. We lose and then regain gain weight, become workaholics, hide behind thousands of texts, social media posts and emails in order to protect ourselves from the part of ourselves that we don’t want to think about.
However, when we step away from the distractions and courageously look at our individual history, our personal life story, honestly and completely, feelings of sadness, anxiety, regret and anger may often arise. These painful emotions bring with them essential insights into how experiences will help you and I individually grow, become a better people, and help others along the path. It takes faith to trust that these experiences will not destroy us, but were allowed to occur by a loving Father or Creator, understanding that for you and I to grow, we must each be given individual agency to chose. It takes faith to recognize that that Father has your individual best interest in mind. Hiding from these emotions clogs the mental and spiritual systems and fuels disabling depression, anxiety, insomnia and fatigue. These feelings, real as they are, persist when there is no other physical sign of illness. That’s because this illness is not physical. It is spiritual. When we are out of line with the truths that bring peace and balance to our lives, negative, self-limiting patterns of activity and fear stifle growth and development mentally.
It is fascinating to me that on more than one occasion, as an osteopath, when a patient suffering from these symptoms gets a massage or has an osteopathic or chiropractic manipulative treatment, they may suddenly become tearful or have unexpected release of emotion. Physical treatment over the areas of congestion can, and do, cause a reflex triggering of mental, emotional or spiritual release of tensions.
How do I know that it is truth we are hiding from? Take the words of the Buddhist teacher Sogyal Rinpoche found in The Tibetan Book of Living and Dying among many others throughout the ages:
“Saints and mystics throughout history have adorned their realizations with different names and given them different faces and interpretations, but what they are all fundamentally experiencing is the essential nature of the mind. Christians and Jews call it “God”; Hindus call it “the Self,” “Shiva,” “Brahman,” and “Vishnu”; Sufi mystics name it “the Hidden Essence”; and the Buddhists call it “buddha nature.” At the heart of all religions is the certainty that there is a fundamental truth, and that this life is a sacred opportunity to evolve and realize that truth.”
“Wait a minute, what does all this have to do with a ketogenic lifestyle?”
The ketogenic lifestyle is one that is based on values. A patient following a ketogenic diet recognizes that food has just as powerful effect on the hormones of the body as does prescription drugs. Understanding the value of hormone balance and the principles that effect weight, inflammation, blood pressure and cholesterol, the ketogenic lifestyle is one in which carbohydrates are restricted in an individually tailored way to obtain the end goal. How does a ketogenic lifestyle balance mind and spirit?
Step One –
Put down your force-field. This takes courage and it takes faith. Your force-field is any distraction that keeps you from thinking and feeling and identifying truth. These include excessive alcohol, illicit drugs, binge eating, smoking, gambling, working excessively or getting lost in repetitive dramatic romantic relationships .
Believe me, the force-field gets heavier every day. After my father passed away at age 58 from the major complications of diabetes and my sister committed suicide a few years later, I threw myself into work and church service. I worked 16-18 hour days, completed a second board certification in Obesity Management and a fellowship in Health Policy, all while serving as a bishop and counselor in my church. I found that I could raise my force-field of justification to hide from the pain and emotions of family illness and depression.
But the force-field saps your energy and cheats you out of seeing your full potential. I found that as long as I held up my force-field (and some of us care more than one), I couldn’t see the experiences that made me who I am and connect me with those I was trying to serve and help. As long as I was holding up my force-field, I was living in the fear of re-experiencing the pain of loss and the worry of future disease, . . . and people sense that.
You don’t have to drop the force-field all at once. You don’t have to quit work and become a hobbit. You just have to lower the field a little bit, enough to peek over and let the Eternal Truth shine on you. Truth is a funny and powerful thing. The more we overcome our reluctance, face the pain and the fear, the more we realize just how often things begin to go well for us. Living in the presence of great truth and eternal law and being guided by permanent values is what keeps a man patient when the world ignores him, and calm and unspoiled when the world praises him.
Step Two–
Identify emotional or behavioral patterns that you want to change. If you don’t know, ask a trusted friend, your spouse, or your relatives. As I think back over the years, I had a couple trusted friends pull me aside and identify a few of those patterns face to face. I appreciate that, and I’ve never forgotten it.
Make a list of the events in your life that you regret and wish you would have made a different decision.
Go over the list as many times as you need to to identify the pattern or theme that seems to tie the regrets together.
Then actually write down the theme or reason that you identified as the cause. This allows you to identify and remove the corrupted soft-ware of your soul.
This process can take time and is often camouflaged by denial.
Major insight often comes as a knock on the door of denial, so listen carefully to what is being said. Listen to yourself listening. Psychiatrists say that if something said while listening to a patient makes them suddenly feel sad or irritable, then that may be a meaningful theme in the patient’s life. Listen to your gut feelings as you go through the day. Don’t ignore a prompting from your soul.
Step Three –
Realize that today’s negative emotional and behavioral patterns are connected with painful memories and unsolved past conflicts.
Do you get a gut feeling that you want to change the subject when someone brings up a financial setback? Do you want to reply with one liners like, “I’m sure it will all work out?” Are there other topics that make you uncomfortable? Ask yourself why that topic makes you uncomfortable . . . seriously, ask yourself, and then answer yourself. Do you suspect your spouse of cheating when there is no objective evidence to support the suspicions? Recognize these uncomfortable feelings are our subconscious waving flags to make us each aware of unresolved conflicts within our mind and spirit.
Remember, we attract the type of energy we give off.
Step Four–
Pray to whatever higher power you believe in. Meditation, prayer and “ponderizing” brings a reservoir of faith and courage to find and to face the truth. If you have the faith, get on your knees and sincerely ask God for help facing your truth and the challenges, fears and sadness that reflecting upon it may initially bring. I promise you that you will gain the strength to accomplish the task. It will bring the strength to overcome the hidden trauma in your earlier life and will give you the strength to resist the call of ice cream at 3 am.
Following these four simple steps, keeps you vigilant to the physical and spiritual warning flags that may arise on your ketogenic journey and will bring great confidence while modifying your diet to balance your body’s hormonal milieu. Confidence inspires courage. Those with courage and confidence in themselves, and faith that they are on the right path, are unstoppable. Good luck . . . I look forward to seeing you on my journey down the same path.
How much protein should you be using? Watch the periscope below . . . and good morning from Surprise, Arizona!!
I’ve included the calculations you will need to get a ballpark estimate on your protein intake from your ideal body weight
Ideal Body Weight (IBW):
These calculations are estimated ideal body weight in kilograms (kg). You can convert your weight in pounds (lbs) to kilograms (kg) with the following formula:
The average male needs 1.2 mg/kg protein per day. The average female needs 1.0 mg/kg protein per day.
Males:
IBW = 50 kg + 2.3 kg for each inch over 5 feet.
Females:
IBW = 45.5 kg + 2.3 kg for each inch over 5 feet.
Examples: If I am 6 feet tall, as a male, then I add 50 kg to 27.6 kg ( 6′ tall is 12 inches over 5′ x 2.3 kg) = 77.6 mg of protein requirement per day. That means that if I (a 6′ tall male) ate three times a day, then my protein requirements are 25.9 mg per meal.
The most exaggerated “frowney” face I get in the office seems to occur when patient’s find out that they cannot eat oatmeal or cereal any longer when following a low-carbohydrate dietary lifestyle. No, oatmeal is NOT good for you . . . I don’t care what WebMD recently said. No, steel-cut oats are even worse (1/4th cup of steel-cut oats is 27 grams of carbohydrate – Who only eats 1/4th cup of oatmeal? Most people eat at least 1/2 -1 cup at a sitting. You do the math . . .)
When I mentioned this to a disabled patient, even her service dog frowned.
Now, before you go running to Larry, the Quaker Oats Mascot (he’s been around for over 140 years), and ask his weight loss advise, I have the solution.
Larry, the Quaker Oats mascot loses 10 lbs for new 2012 cover (He finally figures it out after 137 years)
My angelic wife, Tiffini, the amazing homestead chef and animal husbandry specialist on our little farm, started making low-carb granola for our horseback trail rides. Prior to our discovery of a ketogenic lifestyle, granola was a staple in our pantry, on road trips and in the saddle bags on the trail. This has now replaced any craving either of us had for granola. It carries nicely all day in a Ziplock bag on horseback. It even tastes fantastic in a bowl with unsweetened almond milk as a breakfast alternative if you’re tired of eggs and bacon (but, who ever tires of eggs and bacon? I know . . . Right?!!)
I’ve been nibbling from this actual cookie-sheet of low-carb granola while writing this post. . . I wish you were here to share it with. Soooooo very good, and good for your ketogenic lifestyle. I think I’m going to eat another handful while I finish up Part II of the Principle Based Ketogenic Lifestyle post. Enjoy . . .
In a food processor, process the almonds and 1 cup of the pecans until it resembles coarse crumbs. Using a knife (preferably a sharp one – remember all bleeding stops eventually), chop the remaining 1/4 pecans coarsely.
Melt the butter and place it in mixing bowel or mixer (We use a Kitchen Aid Mixer). Pour the coarsely chopped nuts into the mixing bowl. Stir in flax seed meal, sunflower seeds, coconut flakes, pepitas and vanilla whey protein powder. Blend in the remaining wet mixture, egg whites and add a pinch of salt. Mix until it forms “clumps.”
Spread the mixture evenly on a large wax paper covered baking or cookie sheet and bake at 350 degrees F for 20-25 minutes or until golden brown. Let it cool on the baking sheet to crisp up for a few hours.
It can be stored in a Ziplock bag in the refrigerator.
It has been resoundingly clear to me over the last couple of weeks that there is a tremendous need for a principle based approach to a ketogenic diet. This approach, however, must be simple. So many of the approaches to weight loss I read about are complex and the questions that arise from these approaches are innumerable. Losing weight should not be as difficult as putting a man on the moon. To quote a patient recently, “If it ain’t simple, Doc, I ain’t doing it. . .”
I agree.
Any approach that requires the conversion of food to numbers or calories or exchanges becomes cumbersome, and I personally won’t follow it for more than a week. The principle based approach should be simple and is really based upon the mantra:
Give a man a fish and he will eat today. Teach a man to fish and he will eat for the rest of his life.
Ketogenic diets are wrongly referred to as diets. What I’m talking about is a ketogenic lifestyle. Simple lifestyle design should not be hard. So, what do you say? Shall we learn to fish?!
I assume that if you’re reading this article, you already understand that weight gain is not due to an over intake of calories. Weight gain is due to hormone signals throughout the body leading to the storage of fat . . . specifically, triglycerides being taken up into the fat cells. The hormone that independently controls uptake of fat into each fat cell is insulin. Insulin is an essential hormone, but too much of it stimulates the adipose (fat cells) to over-stock triglycerides or essentially “get fat.” It, actually, is that simple. There’s really only one rule to this lifestyle: If it raises your insulin it will halt or stall your weight loss. Write that on your hand or your forehead or in your planner, the lifestyle revolves around that one rule.
Most people start a ketogenic diet because they want to lose weight and have failed at multiple other dietary approaches. Reasons for weight control failure are often multi-faceted, but they all start with from a position of flawed understanding. The majority of approaches to weight management come from the false assumption that weight is gained because of an over-consumption of calories or a lack of physical activity to burn excess calories. People have faithfully been restricting calories and exercising to exhaustion since the early 1980’s to no avail. (Well, 1% of people succeed, but the rest of us failed this approach). The definition of insanity is repetitive completion of an ineffective action and expecting a different outcome each subsequent time around. If you still think that caloric restriction and exercise is successful, I’ll be shipping your drawstring white vest and your invitation to a padded cell shortly.
Let me put it clearly. We’ve been exercising and cutting our calories since 1975 and look at what it’s gotten us . . .
. . . . a country that is now recognized as the “United States of Corpulence.” Super-Size me has become literal. “Houston . . . we have a problem . . . !”
The rule above is based on foundational principles. Understanding of the principles allows one to successfully apply the rule above.
PRINCIPLE 1
The first principle in a ketogenic lifestyle is understanding that the problem is not caloric, but hormonal. Choices and actions from here on out must be based on this understanding. Anything that will raise insulin will thwart ketosis. Insulin stimulates lipoprotein lipase, the enzyme that pulls the triglycerides into the fat cells. Without insulin, we don’t gain weight. (That’s why type I diabetes are usually very slender and skinny).
The standard lab value for normal fasting insulin levels reflect 10-22 uIU/L as the normal. However, in my office, glucose tolerance tests and postprandial glucose tests consistent with impaired fasting glucose are routinely positive when the fasting insulin level is >5 uIU/L.
Point of Focus: If your having trouble, look at the hormones. Food stimulates hormone responses. Focus on the hormone response to your diet.
PRINCIPLE 2
A ketogenic diet is one where the body uses fatty acids as the primary fuel. Those triglycerides mentioned above are made up of three fatty acids linked to a glycerol molecule. To use the triglycerides, the three fatty acids must be broken away from the glycerol by hormone sensitive lipase (HSL). Insulin directly inhibits HSL. Keeping insulin levels low is the first step in shifting to a ketogenic metabolism. Lowering insulin allows access to the fatty acids in your fat cells. Triglycerides are not water soluble and the rate by which they can be taken up and burned in the mitochondria limits the speed by which triglycerides can be used as fuel. The by product of triglyceride burning is ketones. Ketones themselves can be used as fuel and over 4-6 weeks, the body can enhance its ability to use ketones when fat is the primary fuel. This is called “Keto-Adaptation.”
Point of Focus: Too much carbohydrate in the diet shifts the body from it’s use of fat and triglycerides back to glucose. In general, to become “keto-adapted,” limit carbohydrate to < 20 grams per day. Keep protein at around 0.8 to 1 gram of protein per pound of body weight.
KetoOS – Drinkable Exogenous Ketones
PRINCIPLE 3
Wait a minute!? Where do the ketones come in? When fatty acids are burned or oxidized in the mitochondria of cells within the liver, they are converted into Acetyl-CoA. The Acetyl-CoA is used to form ATP for energy in the Citric Acid Cycle.
IF excess Acetyl-CoA production occurs or if inadequate oxaloacetate is present, the extra Acetyl-CoA is transformed into ketone bodies – specifically beta-hydroxybutyric acid and acetoacetic acid. Fat can be oxidized or burned for fuel while ketones are being produced. Ketones are much smaller molecules and can more easily be transported in the blood than triglycerides, as they are water soluble. The ketones themselves can also be used or burned as fuel as the body upregulates the mitochondria’s ability to use the ketones as fuel as well. As I mentioned above, this process of “keto-adaptation” can take 4-6 weeks. Keto-adaptation results in humans having a greater desire to be physically active – the miraculous conversion of the couch-potato into the bacon-burning triathlete.
Point of Focus: Sugar is a drug. Its byproduct has the same hedonic effect on the brain as morphine. Sugar withdrawal can commonly cause headache, anxiousness, insomnia, dizziness, fatigue and moodiness within the first week of carbohydrate restriction on the road to keto-adaptation.
PRINCIPILE 4
For the average person to become “ketotic” or reach a state of ketosis, it takes lowering the carbohydrates to less than 20 grams per day (and sometimes less than 10 grams per day) for at least 3-7 days. Yes, it can actually take a week to reach ketosis. I have a few patient’s that are so insulin resistant that it takes longer. This means that to reach that fat burning state, one must maintain a low insulin response by restricting starch or carbohydrate intake to less than 20 grams per day for a minimum of a week. For your body to efficiently use the fuel it can take up to 6 weeks. This is why many people state that they “don’t feel good” or “can’t maintain their exercise levels” when starting a ketogenic diet. For most people, once they reach the 6 week mark, mitochondria have been unregulated and “fine tuned” to burn ketones, fat burning becomes efficient and energy levels begin to increase. In fact, for many like myself, you’ll finally feel like exercising for the first time in you life.
Point of Focus: If you’re already exercising, don’t be surprised if you feel more sluggish for the first four weeks. If you’re not exercising, I don’t recommend starting until after you pass through the Keto-Adaptive phase.
PRINCIPLE 5
Clinically, the average patient in my office will lose 5-15 lbs each month for the first three months. Then the weight loss will slow to 2-5 lbs per month. However, 1/2-1 inch continues to disappear off the waist circumference measurement every month. THIS IS NORMAL. Continued weight loss of 15 lbs a month will leave you looking like the Michelin Tire Man – rolls of skin without fat. The body slows the weight loss to keep up with skin and connective tissue remodeling. As long as ketosis is maintained, the fat will continue to melt away. At this point, I’m not so worried about scale weight as I am your waist circumference.
Point of Focus: Successful ketosis does not always affect the scale, but usually causes your pants to fall down.
PRINCIPLE 6
It has been my experience that it takes about 18 months for the average patient to reverse the insulin resistance while following a carbohydrate-restricted, high-fat ketogenic lifestyle. There is no quick fix for this. If there was, I’d be sitting on a beautiful beach in the Caribbean.
Point of Focus: The Ketogenic dietary lifestyle is actually the antidote to insulin resistance, diabetes and the diseases of civilization.
PRINCIPLE 7
Improvement in insulin resistance has also been demonstrated with mild to moderate intensity resistance exercise. Moderate intensity resistance exercise is 20-30 minutes of exercise like walking, easy jogging, cycling, lifting weights, yoga or Pilates with speeds or weight heavy enough to break a sweat, but not so fast or heavy that you cannot carry on a conversation with your exercise partner. Exercise improvesinsulin resistance – BUT IT DOESN’T CAUSE WEIGHT LOSS! Yes, I know, Jack LaLanne just rolled over in his grave. But, let me say that again. Exercise improves insulin resistance, but it does not improve weight loss!! The three largest and most intensive studies of exercise involving over 67,000 people demonstrate that you can exercise till the cows come home and you’ll average about 1% weight loss. If you exercise, realize it WILL make you hungry. Eating the wrong food (carbohydrate containing foods) will stimulate insulin release causing your exercise to be fruitless (Actually, your diet should be “fruit-less” anyway)
Point of Focus: Exercise because you feel like it, it improves insulin sensitivity and it decreases stress, not for weight loss.
PRINCIPLE 8
If you are eating enough fat, you won’t be hungry. Although this doesn’t always hold true in the case of patient’s with lepin resistance. 40-60% of patients with insulin resistance have a concomitant leptin resistance (see the article on lepin resistance here). A ketogenic diet is one in which 50% or more of total calories come from fat. No, you don’t have to count calories, just pick foods that contain 45% fat or more. Look for grass fed products as they will be higher in Omega 3 fatty acids. Red meat is 55% fat. Pork is 45% fat. This is where the chicken salad or turkey wrap fails (see Why Does Your Chicken Salad Stop Weight Loss). Look for alternatives to replace your basic meals and snacks. If you love chips, try pork rinds or make chips from fried cheese or pepperoni. Guacamole is a great replacement for bean dip.
Point of Focus: There is no need to eat 3-6 times per day. As you increase the fat in your diet you will feel more full. Eat when you are hungry, whether that is 3 times a day or once day, listen to your body.
PRINCIPLE 9
I’ve been following a ketogenic diet for over 10 years. The most common complaint I hear is, “Dr. Nally, I’m tired of eating eggs.” Ketogenic diets don’t have to be boring. There are hundreds of resources on the web for spicing up your ketogenic diet. See the Recommended Sites page above for some ideas to start. The Ketogenic Cookbook by Jimmy Moore and Maria Emmerich is a recent edition to the literature and a fantastic resource. Check out Franziska Spritzler’s Low Carb Dietitian website and new book as well. If you live in the UK, you should see Emily Maguire’s website and blog. She just completed a world tour, sampling all the low carbohydrate foods and restaurants around the world. If you are a picture person, check out the Best Keto Meals of 2015 Pinterest page followed by almost 16,000 people. If you haven’t takent the time, you should visit Dr. Andreas Eenfeldt’s website. He is one of Sweden’s premier ketogenic doctors has an immense number of resources at his website, Diet Doctor. Finding someone that can help you fine tune your diet is also essential. You can find a list of doctors that use ketogenic diets here.
Point of Focus: This lifestyle will require you to use real, whole food and cook like your grandmother or great grandmother did in the past. Unfortunately, we’ve lost a great deal of the art of cooking that needs to be re-discovered. If your lifestyle is too busy to cook and prepare real food, that busyness is probably causing you stress, another culprit in the weight gain cycle. The truth will set you free, but it will probably make you miserable first.
PRINCIPLE 10
WARNING! A very sweet patient of mine was given these instructions to treat her weight and blood sugar abnormalities. She applied these principles and they worked marvelously. She called me a few weeks later, however, mad as a wet hen. She placed her husband (not my patient at the time) on the same dietary changes. Her husband, who had significant blood pressure problems and was on four different blood pressure medications I later found out, had a sudden drop in his blood pressure and passed out. As happens to many of my patients, blood pressure, ejection fraction of the heart and blood sugars quickly begin to normalize. However, he never saw his doctor and never had is blood pressure medications adjusted. Because of the normalization that can occur in as rapidly as 1-2 weeks, the medications became much too strong, he passed out and ended up in the emergency room. These dietary principles are effective. They are often just as powerful as a number of the medications that we routinely prescribe.
Point of Focus: Please see your doctor before beginning any of these dietary recommendations, especially if you have any underlying medical conditions including Hypertension, Diabetes, Congestive Heart Failure, Coronary Artery Disease, Gout, Kidney Stones, etc., please do not try the dietary changes alone. Find a physician trained in the use of this type of dietary lifestyle in combination with close monitoring of your blood pressure, blood sugar and other key vital signs.
Stay tuned for Ketogenic Principles . . . Part II in the series where we’ll address Food Psychology, To Cheat or Not to Cheat, and Keeping it Real . . .
I have found, over time, that happiness in life seems to be the greatest when I strive for balance in the three basic aspects of life: Mind, Body & Spirit. Yes, I am a physician, and I spend the majority of my day applying advise and treatment plans that have been demonstrated to be effective through the tried and true scientific method. However, I know from personal experience, and from working closely with patients for over 15 years, that science alone, does not bring fullness and happiness to life. Truth and learning can be found through study and also by faith. Finding balance and peace physically is important, but finding that balance emotionally and spiritually are often essential. Being able to follow a Ketogenic Lifestyle effectively over the long term (longer than 6 months) actually requires understanding of some basic principles. This is the first in a series of articles regarding The Principle Based Ketogenic Lifestyle.
I treat patients with obesity, one of the most difficult diseases to address in the medical office. I find that just applying diet alone doesn’t always solve the problem. If the patient’s life is out of balance emotionally or spiritually, the stress this causes often halts effective weight loss and metabolic healing. You may disagree with me on political or religious issues, but healing is not about politics nor is it about religious doctrine – it is about understanding where we are, the path forward, and our potential to get there. The mind, body and spirit are deeply interconnected. Often, until we recognize and treat those connections, true healing cannot occur.
The first step in treating any illness, including weight, is recognition of the problem. The Medical Community has recognized Obesity as a disease, but obesity is also a symptom of underlying physical metabolic dysfunction that may be tied to the mind and spirit. Daily journaling is the tool that lets one see if the dysfunction is tied to mind or spirit. I ask my patients to keep a daily food journal. This is very important in looking at the patterns of macro-nutrient intake. But the more powerful effect of journaling allows one to see how food is tied to emotion – mentally and spiritually.
Simply writing down what you eat each day, when you eat it, and how you felt after you at it is actually quite profound. The patterns that emerge are usually seen and identified by the patient long before I ever see them. In fact, patient’s often bring those patterns up before ever showing me their food journals.
I’ve found, in keeping a food journal myself, that combining my journaling with other other daily goals, uplifting thoughts and reminders was even more helpful and powerful. This can be done on paper, a notebook, a planner or even on the computer. (I have a few patients who are accountants or engineers – they bring in complex spread sheets). What is important is daily consistency. It takes about 3-4 weeks of journaling to begin to see patterns.
I have taken the advise of one of the leaders of my church to “ponderize” a scripture, meaningful poetic verse or truth filled quote each week as part of the journaling process. He defined “ponderizing” as the act of pondering and memorizing a scripture or a favorite uplifting poem or verse each week. This is done by writing the verse on a written card or note in a place that you will see it frequently each day during the week. When you see it, read it and ponder it. Just the process of frequently reading it will lead to memorization each week. I have found that reading and pondering a verse 3-4 times a day for a week, lends itself to easy memorization. Each time you read the verse, think about it and ponder it for a moment, then go on with your day. This will give you a brief opportunity to elevate your thoughts each day, and will give you a place your mind can go and think when you don’t have to think. It gives your subconscious mind the ability to solve complex patterns at a higher level.
Said David O. McKay, “Tell me what you think about when you don’t have to think, and I’ll tell you what you are.” “As a man thinketh in his heart, so is he . . . ” (Proverbs 23:7).
For some reason, with all the cares of the day, work, family and the challenges of life, I have fallen out of this habit for some time. When this leader mentioned this process in his comments, I was reminded of the peace and balance I used to feel each week when doing this simple activity. I have recommitted myself to restart this activity and I invite you to do the same. This time to ponder opens your mind and allows you access the deeper worries and fears holding you from what you what to accomplish. It takes great courage to make permanent lifestyle and dietary changes. When someone can’t clearly see what lies ahead, it fills them with fear, doubt or both. But journaling, even in its simplest form, gives a person the ability to resist and then master the patterns that have kept them from change. As Mark Twain said, “Courage is resistance to fear, mastery of fear – not absence of fear.”
Courage is tested when we purse difficult goals, fight against disease with unknown outcomes, or work to regain health. The testing can be painful. Journaling, and ponderizing in the process, gives courage to take small steps, one day at a time. Admitting to, journaling when we fail or make mistakes, fear of failure or feeling unsure actually increases our courage. Being given a week to ponderize an uplifting scripture or verse enhances that courage . Journaling successes and failures empowers us individually. The psychiatrist Carl Jung wrote:
“There appears to be a conscience in mankind which severely punishes the man who does not somehow and at some time, at whatever cost to his pride, cease to defend and assert himself, and instead confess himself fallible and human. Until he can do this, an impenetrable wall shuts him out from the living experience of felling himself a man among men. Here we find a key to the great significance of true unstereotyped confession – a significance known in all the initiation and mystery cults of the ancient world, as is shown by a saying from the Greek mysteries: ‘Give up what thou hast, and thou will receive.'”
Journaling and ponderizing allows one a form of confession and renewal. It gives one courage that you have survived today’s challenges and seen the pattern of fallibility in them. It is actually energizing. And, the path to healing begins to become clear.
Journaling also is a great way to outline side effects from carbohydrate withdrawl that will last for 2-4 weeks (That’s for another blog post, however).
Feel free to ask me about the verse that I am ponderizing each week. I will happily tell you which verse I am pondering and memorizing; but, I will in tern, ask you which verse you are ponderizing.
This week, the verse I am ponderizing comes from the Bible – Genesis 35:2-3:
“Then Jacob said unto his household, and to all that were with him, Put away the strange gods that are among you, and be clean, and change your garments: And let us arise, and go up to Beth-el; and I will make there an altar unto God, who answered me in the day of my distress, and was with me in the way which I went.”
Did you begin your food journal? And, what verse are you going to ponderize this week?
I found these charts to be very helpful when trying to calculate your fat intake with a meal. Fish can be challenging in calculating fat content. After reading these charts, I’m craving some sashimi’ed mackerel and salmon.
I’ve personally been following and prescribing ketogenic diets to my patients since 2005. When I started on my ketogenic journey, it was called a “Low Carbohydrate Diet.” Over the last 5-10 years, we’ve learned a thing or two about how the body processes carbohydrate, protein and fat. Specifically, it’s not just the restriction of the carbohydrates that leads to metabolic health, but appropriate protein intake and significant emphasis on the level and type of fat intake as well. The majority of people who cut out carbohydrates will initially see successful weight loss, but to maintain that weight loss and see significant metabolic changes that reverse the diseases of civilization, an understanding of protein and fat needs are essential.
It’s Not Necessarily a High Protein Diet
Most people, when they hear you’re following a “Low-Carb” diet . . . respond with, “Oh, you are on that high protein, Adkins’ thing, . . . right?!”
Well, not really. A true ketogenic diet is NOT a “high protein diet.” However, you must be ingesting enough protein to maintain muscle, hair growth and energy levels. Most people, having been brainwashed in grade school and middle school about the horrors of fat in the diet, assume that if you’re not eating carbohydrates, then you must be eating extra protein to stay satiated. (No one would ever intentionally increase the fat in their diet, right?!!) However, remember that protein and fat usually come together in the sources that the Good Lord put them in.
That’s the impression that most people in my office get when I mention the words “Low-Carb” or “Adkins.” And, before I have a chance to explain that I’m not recommending that you race home to eat three large turkey legs and a pound of turkey bacon, the vegetarians gather their things to leave and the former home economics teachers begin to get chest pain at the mental picture in their heads.
How Are Ketones Made?
A ketogenic diet is one which allows your body to use ketones as it’s primary fuel source. Ketones are produced from the breakdown of triglyceride and free fatty acids. Ketones are essentially produced by two distinctly different events:
1) Starvation caused by prolonged periods without food (which is essentially what happens to type I diabetics when they have no insulin at all in their systems)
2) When fat is ingested as the primary fuel, and very low levels of insulin are concurrently produced, primarily when the diet has minimal to no carbohydrate present (allowing the body to activate its free fatty acid reserves found within in the adipose cells).
The body is an amazing machine. It was designed to take any of the three main macro-nutrients (carbohydrate, protein or fat) as fuel and function quite well. It’s like a futuristic car that can run on unleaded gasoline, oil, or diesel fuel. It is able to recognize which fuel is present and run quite well off of any of the three. The amazing thing about the body is that we mix up all three fuel types and just pour them into the tank. Impressively, the body can separate them out and run very well in the short term on any combination of mixes. We don’t have cars or trucks that do that today . . . maybe in the future . . .?
We have Two Fuel Systems
I like to equate carbohydrates to unleaded fuel. These are clean burning, easy to access and cheap. However, the body requires the production of insulin to use this “unleaded” type of fuel. When carbohydrates are identified to be present in the liver and pancreas, insulin is released so that the rest of the cells throughout the body can “open the tank” and let the carbohydrate into the cell to be used as fuel. The challenge is that carbohydrates don’t store very well in the form they are supplied in, so, as a protective mechanism against starvation and famine, if excess carbohydrate is found in the system, it is converted into triglyceride. Insulin is required for this. Interestingly, when your insulin levels rise, the signal to the body is that “unleaded fuel” is in the system, so it stores any fats and excess carbohydrates in the form of free fatty acid and triglyceride. Carbohydrate stimulate an insulin response and cause fat storage. It is the same reason we give corn to cattle — to plump them up before taking them to market.
Fat then is the “diesel fuel” of macro-nutrients. It burns well, can be stored very easily, and provides over twice the energy to the body when measured in the form of k-cal per gram. Fat is used preferentially when there is limited or no insulin floating around the blood stream and is quickly and efficiency stored when other forms of fuel are available. (Insulin being the key hormone signaling that other fuel is around.)
Nutritional Ketosis is Using Fat as Your Optimum Fuel
So what is this “ketosis thing?” It is a method of dietary change (a lifestyle) that intentionally focuses the body’s metabolism to use fat (in the form of triglyceride & free fatty acid) as its primary fuel. Leading to weight loss, dramatically improved blood sugars, significantly improved cholesterol and triglyceride levels, and notably improved inflammatory markers.
“But don’t you end up eating a lot more protein on your weight loss program?” I frequently get asked.
Honestly, No.
Protein and fat are both very filling, and most people find that limiting the carbohydrates actually causes less hunger and diminishes the rebound carbohydrate cravings often stimulated by the two or three slices of bread, pasta or that potato often occurring 2-3 hours later. Interestingly, most people don’t eat that much more and the protein levels remain fairly constant. Because fat and protein come together in meats, eggs, fish, etc., satiation occurs with just minor increases in dietary intake real animal food. I don’t recommend increase the fat alone. I recommend increasing the amount of real animal protein until you are full. This is even more satiating and many people find themselves eating only twice a day when they are hungry.
Excessive protein in those who are morbidly obese with severe overproduction of insulin can experience a spike the insulin levels further with large amounts of protein. Protein can be equated to the oil you put in your car. Protein is a building block used for muscle, connective tissue and some essential metabolic functions. When too much protein, in this group is ingested, it spikes the insulin. (See my article on Why Your Chicken Salad is Making you Fat)
Most people have problems when they start supplementing with protein shakes. These often contain sweeteners that raise insulin and consequently halts your weight loss – or even causing weight gain.
I recently read a blog post decrying anyone that would recommend a low carbohydrate / ketogenic diet to their patients.
What?!
In fact, this particular blog outlined a number of “adverse reactions” to a ketogenic diet, and based upon these perceived reactions, the writer advised severe caution with its use in just about anyone. It is important to note at the outset that most of the data this blogger quotes are from older studies completed in children for the treatment of epilepsy with specific liquid ketogenic dietary meal replacements. (Not what you’d expect in a low-carb / ketogenic diet for the average obese adult today.)
Diet Confusion
Thanks to recent misinformation by a number of medical professionals, including the person writing the blog referenced above, a poor understanding of fatty acid metabolism by the general community, and a distinct lack of understanding of human adaptability recorded over the last 5,000-6,000 years, there is still significant confusion about ketogenic diets.
It is important to recognize the crucial fact that the human body is designed to function quite well when supplied any of three macronutrients: carbohydrates, proteins or fats. It does so through an amazing series of enzymatic reactions referred to as the Krebs (tricarboxylic acid) cycle, producing needed ATP (adenosine triphosphate) required for our muscles to contract, our heart to beat and our diaphragm to expand our lungs. What’s even more amazing that that the body was designed to recognize the season we are in based up on the food we eat. That is, until we invented refrigerators in 1913. (Now our bodies think it’s year round summer time . . . wait . . . I live in Arizona where it is year round summer time.)
No, this is not a post about unplugging your refrigerator, living on solar, getting off the grid and saving energy.
Our bodies recognize the seasons we are in based upon inherent hormone release. The key hormone is insulin. Insulin can be looked at as the seasonal indicator to our bodies. Insulin production rises and falls based on our intake of carbohydrates (sugar, starches, some fibers). Insulin, essentially, tells our bodies when it is a “time of plenty” and when it was a “time of famine.” Why? You ask. We didn’t have refrigerators 100 years ago and you were lucky if you had a root cellar. The body needs to know when to store for the famine (the winter) that was around the corner. Insulin is that signal.
During the summer, potatoes, carrots, corn and other fruits are readily available. These are all starchy carbohydrates and they all require the body to stimulate an insulin response so that they can be absorbed. Insulin stimulates fat storage (J Clin Invest. 2000;106(4):473-481. doi:10.1172/JCI10842). Just like bears, our bodies were designed to store for the winter.
If you think back in history, your grandparents probably used stored meats & cheeses that could be salted or smoked for preserving during this time of year. Those crossing the plains were commonly found with pemmican, a concentration of fat and protein used as a portable nutrition source in the absence of other food. (Chapter VIII. Narrative of the Life of David Crockett, of The State of Tennessee, Written by Himself, Sixth Edition [E.L. Carey and A. Hart:Philadelphia] 1834, 1837; Marcy, The Prairie Traveler, p. 31.) Think about conversations you may have had with your grandmother when she told you that for Christmas, she received an orange. A single orange for a gift?! Many of my patients drink 12-15 of them in a glass every morning. The winter diets of our grandparents were very low in starches and carbohydrates. When carbohydrate intake is low, little insulin is produced.
Again, insulin is the hormone that tells you that you’re in “a time of plenty” and stimulates weight gain and cholesterol production to prepare for winter. Those prescribing the use of ketogenic diets understand this innate human adaptive trait, and use it to effect changes in weight, cholesterol and other desired metabolic changes.
Three types of ketones. Uptodate.com, May 2015
Now, let’s define the difference between ketosis and keto-acidosis and try to clarify the misinformation that is being spread around the blogosphere.
A ketone is a molecule the body produces from the breakdown of fat and some proteins (amino acids). There are specifically three types of ketones: beta-hydroxybutyric acid, acetoacetic acid and acetone. If ketosis was “bad,” then why would our bodies produce these molecules? They are not bad, and in fact, multiple studies show that the body is often more efficient and effective when it functions on ketones rather than glucose as its primary fuel source. The body can only supply a limited amount of sugar or glucose for fuel. If you talk to runners, marathoners or triathletes, they will tell you that after about 45-90 minutes of continuous endurance exercise the glucose supply runs out and they will experience what is termed a “bonk” (have a low-blood sugar or hypoglycemic episode). Unfortunately, our bodies can only store about 18-24 hours of glucose.
Metobolic Changes of Ketogenic Diet (American Journal of Physiology – Endocrinology and Metabolism Published 1 June 2007 Vol. 292 no. 6, E1724-E1739 DOI: 10.1152/ajpendo.00717.2006)
However, the body can store days upon days of fat in the form of triglyceride in the fat cells. Triglyceride is broken down into ketones. If glucose is the “unleaded” fuel, you can think of ketones as the “diesel fuel” that is easier to store and runs longer.
The average body functioning on ketones as the primary fuel will have a ketone level measured in the blood somewhere between 0.4 and 4 mmol/L. Because of a balance that is created by the use of ketones and a feedback mechanism that kicks in when the ketone level rises, the body will maintain a pH of around 7.4.
Ketoacidosis is dramatically different. If you are a type I diabetic, you don’t produce any insulin. The feedback mechanism regulating ketone use is broken and the ketone levels and triglyceride breakdown speeds up because the body can’t access glucose and can’t produce insulin. The ketone levels spike and the level can rise to > 25 mmol/L. In the presence of a high blood sugar and high ketone level, the acid level in the blood shifts to a pH of less than 7.3. This is referred to as metabolic acidosis and can be life threatening as the low pH shuts down the bodies’ enzymatic processes and a person becomes critically ill and without treatment, can die. (Kitabchi AE et al., Clinical features and diagnosis of diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults. www.uptodate.com, May 2015.)
If you’re not a type I diabetic, you have nothing to worry about. Regardless of what the “ketogenic nay-sayers” blog about, your liver makes approximately 240g of glucose per day, this stimulates a basal release of insulin which keeps the pH in check. It’s also what keeps weight loss at a consistent pace of around 2-10 lbs per month.
If you are a type I diabetic, don’t fret. Carbohydrate restriction can still be used very effectively. It just takes some balancing and understanding of your individual metabolism. Talk to your physician and/or medical bariatrician about how to follow a carbohydrate restricted diet while using insulin.
What about all the other “adverse effects” the blogosphere and other so-called experts claim about ketogenic diets?
Let’s take them on one by one. Are you ready?
Gastrointestinal (GI) disturbances – Yes. Any time you change your diet you may experience diarrhea, constipation or gassiness. Most of the time, this is because you are either 1) not eating enough leafy greens (fiber) or 2) you’re using a supplement that contains an artificial sweetener. Most of the studies on ketogenic diets did not incorporate fiber and the studies used to make this point were on children who used a ketogenic fat supplement shake or liquid preparations containing these artificial sweeteners to make them palatable. If you have spoken to any bariatrician, they will tell you, the best way to follow a ketogenic diet is to eat real food. If you want to read about the anecdotal GI effects of sweeteners, read the comment section in Amazon about the Haribo Sugar Free Gummy Bears.
Inflammation Risk – In every patient that I have placed on a ketogenic diet in the last 8 years, all inflammatory markers including CRP, Sedimentation Rate and Uric Acid have all decreased. Inflammation gets better on an appropriately formulated ketogenic diet. The older studies of ketogenic diets in children contain most of their fat from Omega-6 fatty acids from vegetable oil which will increase inflammation and oxidative stress, spike the cortisol levels and have the secondary effect of actually raising the triglycerides. (Simopoulos AP,The importance of the ratio of omega-6/omega-3 essential fatty acids, Biomed Pharmacother., 2002 Oct;56(8):365-79.)
Muscle Cramps/Weakness – The process of weight loss occurs by burning fat into CO2 and water. We breathe the CO2 out, but the water produced has to follow salts out through the kidneys. Hence, we lose salts. This can cause weakness and muscle cramps. The solution? Stop restricting salt on a low carbohydrate diet. We are the only mammal that restricts salt and we do it because low-fat diets cause us to retain water. Low carbohydrate diets do the opposite. Use sea salt or sip beef or chicken bouillon broth with your dinner. The use of yellow mustard also helps (the small amount of quinine in yellow mustard stops the cramping). If you have congestive heart failure, talk to your doctor about monitoring your salt intake in balance with your diuretic or water pill.
Hypoglycemia – If you read the ketogenic diet research, most of it was done on epileptic children. The diets called for a period of starvation, then the use of a ketogenic liquid based on the John’s Hopkin’s protocol. It is a well-known fact in medicine that starvation in children can frequently cause hypoglycemia, especially in children with other genetic or congenital defects leading to forms of epilepsy. In clinical practice, with ketogenic diet use in adults, hypoglycemia is rare.
Low Platelet Count (Thrombocytopenia) – Again, this was seen in the epileptic children who were placed into starvation first, then introduced a liquid fat replacement shake to stop intractable seizures. These liquids or shakes were often nutrient deficient in other essentials. Folic acid, B12 and copper deficiency can occur when not eating “real food.” Low platelet counts are rarely seen on ketogenic diets based around “real food.” Many children in the ketogenic studies had been on or were concomitantly on valproic acid for their seizures. Valproic acid is commonly known to cause thrombocytopenia (Barry-Kravis E et al, Bruising and the ketogenic diet: evidence for diet-induced changes in platelet function. Ann Neurol. 2001 Jan;49(1):98-103.; Kraut E, Easy Bruising, http://www.uptodate.com, May 2015.)
Easy Bruising – This is usually due to inadequate protein supplementation as was the case in much of the ketogenic literature where protein levels were also restricted. (Kraut E, Easy Bruising, http://www.uptodate.com, May 2015.)
Pancreatitis – Patients who are insulin resistant or have impaired fasting glucose commonly have high triglycerides. Elevation in triglycerides itself is a cause of pancreatitis. Ketogenic diets lower the triglycerides. However, if a patient has not been following their diet as directed, spikes in the triglycerides can occur placing the person at risk for pancreatitis.
Long QT Intervals/Heart Arrhythmias – The list of things causing Long QT intervals and abnormal heart rhythms is long and variable (Acquired Long QT Syndrome. Berul C et al. www.uptodate.com, May 2015). It is well know that starvation, rapid weight loss and liquid protein diets can cause a delay in the conduction signal in the heart. Anyone wishing to start any diet should have an electrocardiogram (EKG) through their doctor to ensure that the diet (of any type) doesn’t exacerbate a prolonged QT interval.
Three year weight loss and metabolic improvement in a patient on a Low-Carb / Ketogenic diet. Note: Patient admits to not following ketogenic diet during holidays from Nov 2013 – Feb 2014 (see the dramatic changes to the body when cheating happens)
Cardiomyopathy – Prolonged QT intervals have been associated with cardiomyopathy and the former can stimulate the later. Any diet that has the potential to prolong a QT interval has the potential to cause cardiomyopathy. Hence the need for regular EKG monitoring on any diet (Acquired Long QT Syndrome. Berul C et al. www.uptodate.com, May 2015).
Lipid/Cholesterol Changes – In the 8 years I have been applying ketogenic diets to patients, I have seen dramatic improvement in the triglycerides and HDL levels. The only time triglycerides rise over 100 is if the patient is using artificial sweeteners or is cheating on the carbohydrate restriction. Total cholesterol commonly rises, however, this is indicative of the fact that there is a shift in the LDL particle size and this affects the calculation of both total cholesterol and LDL-C. In light of this, most of my patients have dramatic improvement in triglycerides and small dense LDL particle number. I’ve included the common cholesterol changes I seen in my office as a few case reports to demonstrate the effectiveness of a ketogenic diet:
2 year ketogenic dietary labs and weight loss
Myocardial Infarction – It is interesting that one blogger includes this on the list of adverse reactions, however, when you actually read the study, the author of the paper make an “assumption” that there was potential for heart attack due to an elevated total cholesterol, however, a correlation was never made. Again, in the 8 years I have been using ketogenic diets, I have seen dramatic improvement in cholesterol profiles, inflammatory markers, atherosclerosis and carotid intimal studies (Shai I et al, Circulation 2010; 121:1200-1208).
Three year metabolic history of a Low-Carbohydrate / Ketogenic diet
Menstrual Irregularities / Amenorrhea – It is well known that any diet causing protein or other nutritional deficiency will affect the menstrual cycle first and growth second. The only time menstrual irregularities occur with a ketogenic or Low-Carb diet is when a patient is not taking in enough protein or is not eating real food. What amazes me is that a properly applied ketogenic diet causes normalization of the menstrual cycle, and in my practice, I’ve had a number of women successfully be able to conceive after making a ketogenic dietary change.
For more details on the nutrient content of a ketogenic diet, see the recent article by a friend of mine, Maria Emmerich. She’s been creating ketogenic diets for years and has a number of fantastic books my wife and I have been using in our home over the last nine years. She is one among many that can give you some direction on how to devise a healthy, real food based ketogenic diet. See the page on my website here that will give you some direction in formulating your Ketogenic Lifestyle.
Nally Family Low-Carb / Ketogenic Cheese Cake
So, to celebrate Mother’s Day, today, with my family, I am going to indulge in some Low-Carb / Ketogenic Cheese Cake!! Happy Mother’s Day, to all of you and especially to all you mothers out there making a healthy difference in the lives of your families! (You can find the recipe for this delicious cheese cake here)
In the words of Sir William Ostler, “If it were not for the great variability among individuals, medicine might well be a science and not an art.”
Have you noticed that there are a large number of advertisements in the media about checking your testosterone or “Low T” Syndrome? It seems like this is the new advertising trend on the radio and late night TV.
Suddenly, everyone’s testosterone is low and men are complaining about their libido, . . . or are they?
Benefits of Testosterone Optimization. (Image Credit: ArtOfManliness.com)
If you practice medicine long enough, you’ll see a trend that seems to have arisen as our waistlines have expanded. About half of the men in my office with insulin resistance, pre-diabetes or diabetes have low testosterone levels. But this shouldn’t be a surprise. Type II diabetes, metabolic syndrome and insulin resistance are all driven by an over production in insulin in response to a carbohydrate load in the meal. Patients with these conditions produce between two to ten times the normal insulin in response to a starchy meal. A number of studies both in animal and human models demonstrate that insulin has a direct correlation on testosterone suppression in the blood. This has been demonstrated in both men and women. In fact, glucose intake has been shown to suppress testosterone and LH in healthy men by suppressing the gonadal hormone axis and more predominant testosterone suppression is seen in patient with insulin resistance or metabolic syndrome.
In fact, to put it simply, insulin increases the conversion (aromitization) of testosterone to estrogen in men (it does the opposite in women). Interestingly, Leptin resistance has a similar effect. I tend to see the worst lowering of testosterone in men with both insulin and leptin resistance.
How to you improve your testosterone? Supplemental testosterone has been shown to help, but it comes with some risks, including prostate enlargement and stimulating growth of prostate cancer. The most natural way to improve your testosterone is to change your diet.
A low carbohydrate or ketogenic diet turns down the insulin production and allows the testosterone to be available for use by the body. A ketogenic diet has the effect of reducing leptin resistance as well through weight loss. A simple dietary change of this type is frequently seen in my office to increase testosterone by 100-150 points.
KetoOS – Drinkable Exogenous Ketones
What is a ketogenic diet? It is a diet that restricts carbohydrates to less than 50 grams per day, thereby causing the body to use ketones as the primary fuel source. So, for breakfast tomorrow morning, hold the oatmeal (1/2 cup of Quaker Instant Oatmeal is 31 grams of carbohydrates) and have the bacon and eggs. And, rather than have the cheesecake for desert this evening, have an extra slice of steak butter on your rib-eye and hold the potato.
A few of my patient’s have fallen off the carbohydrate restriction waggon this last year. In celebration of restarting your low-carb lifestyle and resolutions to improve your health, I propose the following celebration.
1) Go home right at 5pm
2) Pull out your favorite skillet (mine is a well used Lodge Cast Iron pan)
3) Remove your favorite full fat sausage from the freezer.
4) Look up your favorite cream cheese waffle recipe.
5) Make your self a Sausage Sanctuary, a Bacon Bungalow or a Low-Carb Cabin (whatever tickles your fancy) in celebration of restarting your carbohydrate restriction and removing the carbage from your life.
I suggest you use a Low-Carb cream cheese waffle you can find here for the roof.
Now you have to watch your salt ingredients too. Store bought salts are starting to add dextrose for flavor. Dextrose is just another word for SUGAR!! Aaarrrrhhhhh!! Why do you need to add sugar to your salt? You don’t. Throw out any salt that contains dextrose. It will raise your cholesterol and cause weight gain.
Never noticed this until it was pointed out by Maria Emmerich. Thanks, Maria.
Don’t fear the fat. If you haven’t seen the movie Cereal Killers, you should watch it by clicking here. D.J. O’Neill ditches wheat and sugar in a food plan consisting of 70% fat – under the guidance of legendary South African Sports Scientist Prof. Tim Noakes.


















 After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the
After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the