I will be starting a twice weekly exclusive live-stream here for my amazing online followers and patient who are participating in the KetoClan Group on the following sixteen topics next week. Will be sharing the basics and my 22 years of clinical experience with each of these topics as it relates to health and weight management. These topics will take 10-30 minutes, then giving the remainder of the hour to you to ask questions.
The topics we will cover over the next 8 weeks are listed below: 1. Insulin 2. Monitoring Glucose – CGMs 3. Fat Adaptation 4. Things that make insulin go “bump in the night (or the day)” – (sweeteners, creamers, teas, Resveratrol, nuts, etc) 5. Protein 6. Basic Thyroid Function 7. Female Hormones 8. Male Hormones 9. Testing Ketones in Urine, Breath, Blood 10. Ketoacidosis 11. Medications and ketogenic diets (Metformin, DPP4s, GLP-1, SLT-2s, sulfonoureas, Berberine) 12. Stress – Cortisol & DHEA 13. Exercise – Cardiovascular and Resistance Exercise 14. Sleep 15. Food Cravings and the Subconscious Mind 16. Keto, Carnivore or Fasting – What should I be doing?
The most common complaint that I get in my office when someone has started a ketogenic diet is, “Doc, I feel fatigued. Will this ever go away?”
That feeling of fatigue, some refer to as the “keto-flu,” is usually due to a couple of things. First, you may not be eating enough fat (I recommend a 1 gram to 1 gram ratio of protein to fat when getting started). Second, you’re not taking in enough salt (specifically sodium, potassium, magnesium and/or zinc). These four salts are essential electrolytes our body requires for proper function.
If salt is the problem, the you will be experiencing leg cramps. Cramps during daytime activity are usually due to low sodium or potassium levels. Cramps that wake you up at night are usually due to low magnesium or zinc. Leg cramps can also be due to hypothyroidism or significant blood sugar swings. Dr. Nally will usually check for this during your visit with him.
“But isn’t too much salt bad for you?” I am frequently asked.
Too much salt is only bad for you if you’re eating a “low-fat” diet.
What if increasing salt intake actually lowered your blood pressure?
Did you know that increasing your salt intake can actually improve your diabetic blood sugar if you are following a correct diet? Could it be that easy?
Almost every patient that I see in the office has a significant worry about salt intake, some greater than others. In fact, some people are so fearful about salt that when I initially began encouraging its use, they told me that I was crazy, and they left my practice.
Has restricting salt over the last 50 years really worked, or is it doing more damage than we think?
That was the question that was asked by Dr. Ames in the American Journal of Hypertension 17 years ago. However, his answer never got a mention. In fact, I’ve been in practice for almost 20 years, and incidentally stumbled upon this article when it was mentioned by a colleague of mine. Granted, the study is a small sample size of people, only twenty-one. However, the results are profound.
Twenty-one patients with hypertension were randomized to periods of no salt (placebo) and periods of 2 grams (2000 mg) of sodium chloride four times a day (a total of 8 grams of salt per day). Glucose tolerance tests were completed with insulin levels at the end of each intervention period.
Insulin Resistance and Hypertension Improve by Adding Salt
Three very noteworthy results happened. First, those patients with insulin resistance and diabetes had improvement in their glucose levels while on 2 grams of sodium supplementation.
Second, those with hypertension also, shockingly, showed improvement in their blood pressure while on the 2 grams of sodium supplementation.
Third, those with insulin resistance had a lowering of their insulin levels during the period of increased sodium intake. These findings fly in the face of the dogma that’s been drilled into our heads that “salt is bad!”
“But, Dr. Nally, you can’t base your findings on a small group of 21 people,” the experts say.
Yes, it is a small study group. However, these findings are identical to what I, also, see clinically every day in my practice for over 20 years.
We know that the average human needs at a minimum 3 grams of sodium per day and 3 grams of potassium per day. The standard American diet (SAD diet) including processed foods contains 2-3 grams per day of sodium and potassium. In fact, the CDC claims the worst salt containing meals for you are:
Bread
Processed chicken dinners
Pizza
Pasta
Insulin also stimulates additional retention of sodium at the kidney level. If you are insulin resistant, producing excess insulin in response to starches or sugars, you retain notably larger amounts of salt when eating the standard American diet (SAD diet) or a “low-fat” diet. However, if your following a low-carbohydrate or ketogenic lifestyle, you won’t be eating the meals above and you’re probably not getting near enough salt.
Salts, or electrolytes, are essential in normal cellular function. Low salt in the body is like running your car without oil. It will run, but not very efficiently and over the long term will cause problems. This is the cause of the keto-flu I wrote about previously. And, according to the study above, it is a potential driver of our persisting insulin resistance, diabetes and hypertension.
How Much Salt Should I Use?
In my office, I encourage use of 3-4 grams of sodium and 3-4 grams of potassium daily when using a ketogenic lifestyle. That’s approximately 1 ½ – 2 teaspoons of salt per day. I like the Redmond’s RealSalt or pink Himalayan salt because these products contains all four types of salt (sodium, potassium, magnesium and zinc).
It is probably that your salt restrictions is making your insulin resistance and blood pressure worse. That’s what the clinical evidences are pointing toward, and it is what I see every day in my office.
Want to know more about a ketogenic life-style? Click the KetoLife link to get some basics.
If you’re already following a ketogenic lifestyle, then let me help you navigate the bumps and turns by going to the KetoKart and checking out the products I recommend to jump-start ketosis DocMuscles-style!
Until then, I’ll have another piece of bacon, please . . . and, oh, pass the salt!
Pre-order your copy of my new book that will be available on September 26, 2017.
The ketogenic diet isn’t just a great tool for helping people lose weight and feel their best; it’s also an extremely effective method for treating the common “diseases of civilization.” The Keto Cure will give readers the prescription they need to heal their bodies by eating plenty of fat and moderating protein and carbs.
I’ve been advocating a low-carb, high-fat diet in my clinical practice for over fifteen years, helping people address their health problems by making better food choices. I teamed up with bestselling low-carb author and podcaster Jimmy Moore to create a top-50 health podcast espousing the benefits of eating keto. Now, for the first time, I’ve taken my years of clinical experience, put everything down on paper, and create a how-to guide that details all the ways in which the ketogenic diet can help remedy common ailments.
The Keto Cure details the science behind the keto diet’s effectiveness at treating a wide range of diseases, including:
Alzheimer’s
Epilepsy
Fatty liver disease
Hypercholesterolemia
Hypertension
Parkinson’s disease
Thyroiditis
Type 2 diabetes
and many more
The Keto Cure also outlines practical tips gleaned from Dr. Nally’s fifteen-plus years in medical practice, as well as Moore’s ten-plus years as a health and wellness podcaster, on overcoming the common pitfalls that people experience when adapting to a high-fat way of eating, including fatigue and keto flu. This helpful information, combined with a wide variety of delicious keto recipes from international bestselling cookbook author Maria Emmerich, makes The Keto Cure a complete resource for healing oneself with the ketogenic diet.
Listen and watch as we talk about how ketosis, or the absence thereof plays a role in the formation of the Diseases of Civilization (It’s not rocket science, or maybe it is?)
We touch on non-alcoholic fatty liver disease, carbohydrate restriction, the use of protein and even exercise (Did you say “eggs are sides . . .” or exercise?). So pull up a piece of string cheese and spend 20 minutes that may just change your life.
You can find the vitamin supplements that Dr Nally developed and uses himself and with his patients at KetoLiving.com.
You can find exogenous ketones referenced in the video at DynamicKetones.com
Stomach Pain & Swelling with Hereditary Angio-Edema (HAE)
Listen to KetoTalk Podcast #32 where we talk about hereditary angio-edema, adequate ketone ranges, statin use while in ketosis and healthy keto questions. You can listen in by going to KetoTalk.com or you can listen in on iTunes.
“About 40 percent of my older patient population who take statins while eating ketogenic experience some form of myalgia they didn’t have before. And there’s an amplified side effect profile: muscle ache, joint pain, generalized fatigue, liver enzyme elevation, and cloudy headed.” — Dr. Adam Nally
I am frequently asked about the sweeteners that can be used with a low carbohydrate diet. There are a number of sweeteners available that are used in “LowCarb” pre-processed foods like shakes or bars, or in cooking as alternatives to sugar. However, most of them raise insulin levels without raising blood sugar and are not appropriate for use with a true low-carbohydrate/ketogenic diet. You can see and print the article I published clarifying which sweeteners you can use and which ones to avoid here:
Of recent note, I’ve been asked about the insulin response that occurs in the study found here quoted by Dr. Jason Fung in his wonderful book, The Obesity Code.
First, it is essential to note that both the crystalline form of Stevia and the aspartame used in the form of Equal, also a crystal, contain either dextrose or malto-dextrin as the crystallizing agent. Both dextrose and malto-dextrin have a known insulin spike equal to table sugar. You can see that in my article link above. Watch the video and we’ll discuss which forms of Stevia and aspartame don’t raise insulin in myself or my patients.
Aspartame has been effective in appetite suppression in many obesity patients clinically. However, recent studies have demonstrated that aspartame does have a negative effect on gut flora, has potential to cause insulin resistance to persist when used long term (seen in animal studies) and has been shown to damage the mitochondria of brain cells (also animal studies). I now caution my patients with its use. We will keep a very close eye on all these sweeteners.
KEY QUOTE: “Children are born in ketosis, so ketones are perfect for babies. The level of fat in breast-milk is essential for them to maintain their health and their growth.” — Dr. Adam Nally
Here’s are the 12 questions Jimmy and Adam answered in this special Keto Talk Mailbox Blitz extended podcast today:
– Testimonial from someone who learned his lesson why it’s important to stay ketogenic all the time
– Three-decade study confirms saturated fats are bad for health
– Is increased testosterone from a ketogenic diet a bad thing for women?
– Why am I still struggling with low energy and low ketones after months of being in ketosis?
– Can being in nutritional ketosis above 1.0 mmol cause painful headaches?
– Do artificial sweeteners and stevia raise insulin?
– Is my ketogenic diet causing me to cramp up before and during my half marathon racing?
– Is MCT oil a better fat to use on a ketogenic diet than other fats like coconut oil, cream, or butter?
– Why do I have a constant stomachache while I’m on a ketogenic diet?
– Do you have to be in ketosis to burn fat?
– Does being in ketosis lead to daily spotting and extended periods?
– Are ketones in my baby’s breastmilk safe for her to consume? And why did my milk supply drop when I went keto?
– What is the impact of the supplement creatine on ketones, blood sugar, and insulin levels?
– Can I ease into ketosis as a way to avoid the dreaded “keto flu?”
KEY QUOTE: “If you’re not feeling energy after that adaptation period of 2-4 weeks at the very most, then you’re doing something wrong. Let that be your wakeup call to change something.” — Jimmy Moore
A patient recently asked me how bad being in nutritional ketosis was for her. I responded that the worse problem I’ve seen recently is the patient that broke his toe when he slipped on bacon grease. Are there risks with a ketogenic diet? Yes, but these usually only occur when you cheat or fall off the wagon. What problems can arise? Lets talk about them individually.
First, as I stated above, make sure you don’t slip on bacon the grease. It really can be an issue if you’re not used to using increased amounts of fat in your kitchen. So, be prepared for how to cook and use fat. Grandma understood this well, we could learn a great deal from her if you ask her about using bacon grease.
Second, let’s define the difference between ketosis and keto-acidosis and try to clarify the misinformation that is being spread around the blogosphere.
A ketone is a molecule the body produces from the breakdown of fat (specifically triglycerides) and some proteins (amino acids). There are specifically three types of ketones: beta-hydroxybutyric acid, acetoacetic acid and acetone. If ketosis was “bad,” then why would our bodies produce these molecules? They are not bad, and in fact, multiple studies show that the body is often more efficient in weight loss, inflammatory reduction, bowel function, epigenetic influence and maintenance of lean body mass more effectivly when it functions on ketones rather than glucose as its primary fuel source. You can see these studies here, here, here and here.
The body can only supply a limited amount of sugar or glucose for fuel. If you talk to runners, marathoners or triathletes, they will tell you that after about 45-90 minutes of continuous endurance exercise the glucose supply runs out and they will experience what is termed a “bonk” (have a low-blood sugar or hypoglycemic episode). Unfortunately, our bodies can only store about 18-24 hours of glucose.
However, the body can store days upon days of fat in the form of triglyceride in the fat cells. Triglyceride is broken down into ketones. If glucose is the “unleaded” fuel, you can think of ketones as the “diesel fuel” that is easier to store and runs longer.
The average body functioning on ketones as the primary fuel will have a ketone level measured in the blood somewhere between 0.4 and 4 mmol/L. Because of a balance that is created by the use of ketones and a feedback mechanism that kicks in when the ketone level rises, the body will maintain a pH of around 7.4.
Ketoacidosis is dramatically different. If you are a type I diabetic, you don’t produce any insulin. The feedback mechanism regulating ketone use is broken and the ketone levels and triglyceride breakdown speeds up because the body can’t access glucose and can’t produce insulin. The ketone levels spike and the level can rise to > 25 mmol/L. In the presence of a high blood sugar and high ketone level, the acid level in the blood shifts to a pH of less than 7.3. This is referred to as metabolic acidosis and can be life threatening as the low pH shuts down the bodies’ enzymatic processes and a person becomes critically ill and without treatment, can die. Further information on ketoacidosis can be found here.
If you’re not a type I diabetic, you have nothing to worry about. Regardless of what the “ketogenic nay-sayers” blog about, your liver makes approximately 240g of glucose per day, 24 hours a day, 7 days per week, this stimulates a basal release of insulin which keeps the pH in check. It’s also what keeps weight loss at a consistent pace of around 2-10 lbs per month.
If you are a type I diabetic, don’t fret. Carbohydrate restriction can still be used very effectively. It just takes some balancing and understanding of your individual metabolism. It does require close blood sugar and insulin monitoring. If you are a Type I diabetic, please talk to your physician, obesity specialist and/or bariatrician about how to follow a carbohydrate restricted diet while using insulin. It can be done and it can be done very effectively, but monitoring is essential.
What are the other potential problems that can arise when you follow a ketogenic diet?
Gastrointestinal (GI) Disturbances – Yes. Any time you change your diet you may experience diarrhea, constipation or gassiness. Most of the time, this is because you are either 1) not eating enough leafy greens (fiber) or 2) you’re using a supplement that contains an artificial sweetener. Most of the studies on ketogenic diets did not incorporate fiber and the studies used to make this point were on children who used a ketogenic fat supplement shake or liquid preparations containing these artificial sweeteners to make them palatable. If you have spoken to any obesity specialist, they will tell you, the best way to follow a ketogenic diet is to eat real food. If you want to read about the anecdotal GI effects of sweeteners, read the comment section in Amazon about the Haribo Sugar Free Gummy Bears.
Oh, by the way, 65% of patients in my practice following ketogenic diet see improvement in gastroesophageal reflux (GERD) symptoms. This was seen in a 2006 study looking at ketogenic diets and reflux.
Hair Loss/Thinning– Yes. This does happen initially and if you are not eating enough fat. It is important to note that hair loss/thinning can occur with any form of weight loss. You can see data on this here. Hair loss is very common if you are restricting calories, which was occurring in a number of the ketogenic dietary studies previously published. You do not, and should not, need to “restrict calories” if you are following a ketogenic diet correctly, and in fact, most people take in more than 1800 calories on a ketogenic diet.
Inflammation Risk– In every patient that I have placed on a ketogenic diet in the last 10 years, all inflammatory markers including CRP, Sedimentation Rate, Apo B, HOMA-IR and Uric Acid have all decreased. Inflammation gets better on an appropriately formulated ketogenic diet. The older studies of ketogenic diets in children contain most of their fat from Omega-6 fatty acids from vegetable oil which will increase inflammation and oxidative stress, spike the cortisol levels and have the secondary effect of actually raising the triglycerides. You can find more information on this here & here.
Kidney Stones/Gout – These (kidney stones & gout) are both commonly caused by spikes in uric acid. As noted above, I’ve seen multiple cases in my practice where a ketogenic diet lowers uric acid. Only a small clinical trial has been published in the literature (and it wasn’t truely ketogenic), but the results point to the potential for ketogenic diets to lower uric acid. Ketogenic diets also have the capacity to lower the formation of calcium oxalate stones through a secondary mechanism where calcium oxalate formation is driven by uric acid formation. Older small case reports in the pediatric seizure literature identify calcium oxalate stones, however, dehydration (too little fluid/water intake) is the primary cause of kidney stones.
So, are ketogenic dietary patients at risk? Only if you cheat on your carbohydrate restriction and you let yourself get dehydrated. So, I warn patients. Don’t cheat and make sure your drinking adequate amounts of water.
Muscle Cramps/Weakness– The process of weight loss occurs by burning fat into CO2 and water. We breathe the CO2 out, but the water produced has to follow salts out through the kidneys. Hence, we lose water and salts. This can cause weakness and muscle cramps. The solution? Stop restricting salt on a low carbohydrate diet. We are the only mammal that restricts salt and we do it because low-fat diets cause us to retain water. Low carbohydrate diets do the opposite. Use sea salt or sip beef or chicken bouillon broth with your dinner. You may consider adding magnesium to your diet. The use of yellow mustard also helps (the small amount of quinine in yellow mustard stops the cramping). If you have congestive heart failure, talk to your doctor about monitoring your salt intake in balance with your diuretic or water pill.
Hypoglycemia– If you read the ketogenic diet research, most of it was done on epileptic children. The diets called for a period of starvation, and then the introduction of a ketogenic liquid based shake following the John’s Hopkin’s protocol. It is a well-known fact in medicine that starvation in children can frequently cause hypoglycemia, especially in children with other genetic or congenital defects leading to forms of epilepsy. In clinical practice, with ketogenic diet use in adults, hypoglycemia is rare. The only time I see hypoglycemia is when patient’s with significant insulin resistance or diabetes cheat on a large amount of carbohydrate and get a secondary insulin surge leading to hypoglycemia 3-5 hours after cheating.
Low Platelet Count (Thrombocytopenia)– Again, this was seen in epileptic children who were placed into starvation first, then introduced a liquid fat replacement shake to stop intractable seizures. These liquids or shakes were often nutrient deficient in other essentials. Folic acid, B12 and copper deficiency can occur when not eating “real food.” Low platelet counts are rarely seen on ketogenic diets based around “real food.” Many children in the ketogenic studies had been on or were concomitantly on valproic acid for their seizures. Valproic acid is commonly known to cause thrombocytopenia and this is another reason that thrombocytopenia was seen in this population. (Barry-Kravis E et al, Bruising and the ketogenic diet: evidence for diet-induced changes in platelet function. Ann Neurol. 2001 Jan;49(1):98-103.; Kraut E, Easy Bruising, http://www.uptodate.com, May 2015.)
Impaired Concentration/Mood– A number of patients starting carbohydrate restriction will go through 2-4 weeks of carbohydrate withdrawal. This carbohydrate withdrawl can be experienced just as powerfully as morphine withdrawal in some patients. Sugar is a drug and has a powerful effect on the same hedonic receptors that morphine does in the brain. Some patients will experience headache, tremor and decreased concentration while “withdrawing” off of starches and carbohydrates. Studies show that after the 4-8 week period of keto-adaptation, cognitive function dramatically improves.
Easy Bruising – This is usually due to inadequate protein supplementation as was the case in much of the ketogenic literature where protein levels were also restricted. (Kraut E, Easy Bruising, http://www.uptodate.com, May 2015.)
Pancreatitis – Patients who are insulin resistant or have impaired fasting glucose commonly have high triglycerides. Elevation in triglycerides itself is a cause of pancreatitis. Ketogenic diets lower the triglycerides. However, if a patient has not been following their diet as directed, spikes in the triglycerides can occur placing the person at risk for pancreatitis.
Long QT Intervals/Heart Arrhythmias – The list of things causing Long QT intervals and abnormal heart rhythms is long and variable (Acquired Long QT Syndrome. Berul C et al. www.uptodate.com, May 2015). It is well know that starvation, rapid weight loss and liquid protein diets can cause a delay in the conduction signal in the heart. Anyone wishing to start any diet should have an electrocardiogram (EKG) through their doctor to ensure that the diet (of any type) doesn’t exacerbate a prolonged QT interval.
Cardiomyopathy– Prolonged QT intervals have been associated with cardiomyopathy and the former can stimulate the later. Any diet that has the potential to prolong a QT interval has the potential to cause cardiomyopathy. Hence the need for regular EKG monitoring on any diet (Acquired Long QT Syndrome. Berul C et al. www.uptodate.com, May 2015).
Lipid/Cholesterol Changes – In the 10 years I have been prescribing ketogenic diets to patients, I have seen dramatic improvement in the triglycerides, small dense LDL particle and HDL levels. The only time triglycerides rise over 100 is if the patient is using artificial sweeteners, is cheating on the carbohydrate restriction, or is taking in too much protein. Total cholesterol commonly rises, however, this is indicative of the fact that there is a shift in the LDL particle size and this affects the calculation of both total cholesterol and LDL-C. In light of this, most of my patients have dramatic improvement in triglycerides and small dense LDL particle number.
Myocardial Infarction – In older papers, elevated total cholesterol was noted and the authors made the “assumption” that myocardial infarction “could” be a risk. We now recognize that elevated Total Cholesterol is NOT a causitive risk for heart disease.
These previous assumptions have been interpreted by the blogosphere ketogenic “nay-sayers” as actual risk. However, a correlation and causation was never made. Again, in the 10 years I have been using and prescribing ketogenic diets, I have seen dramatic improvement in cholesterol profiles, inflammatory markers, atherosclerosis and carotid intimal studies (Shai I et al, Circulation 2010; 121:1200-1208).
Menstrual Irregularities / Amenorrhea– It is well known that any diet causing protein or other nutritional deficiency will affect the menstrual cycle first and growth in stature second. The only time menstrual irregularities occur with a ketogenic or Low-Carb diet is when a patient is not taking in enough protein and/or fat, and is not eating real food. What amazes me is that a properly applied ketogenic diet actually causes normalization of the menstrual cycle, and in my practice, I’ve had a number of women successfully be able to conceive after making a ketogenic dietary change.
Is a ketogenic diet bad for you? You be the judge.
If you are following a ketogenic diet correctly and with real food, the only thing you really need to worry about is slipping on bacon grease.
In an era where over 70% of us (35.7% obesity & 34% overweight in 2015 according to the CDC) have started to resemble the food pyramid, seeing the effect of a carbohydrate heavy diet should give a clue.
Our bodies were meant to burn ketones. We have a parallel system within us designed to use ketones as an energy source. Ketones are faster and more efficient than the way our bodies use glucose. Ketones give you 38% more energy than you can get from glucose. We as a society are following a deceptive food pyramid.
When we limit or remove carbohydrate from our diet, we are left with ketones as a primary fuel. It is time that we recognize what Dr. Yudkin was trying to tell us in 1970’s, that our carbohydrate and sugar intake is the driver for heart disease, diabetes and the diseases of civilization. (Yudkin, John. Sweet and dangerous: the new facts about the sugar you eat as a cause of heart disease, diabetes, and other killers. PH Wyden, 1972.)
We’ve never really seen a man or an elephant in long term ketosis before . . .
“It’s a snake.”
“It’s a wall.”
“It’s a rope.”
“It’s a fan.”
“It’s a tree.”
“It’s insulin resistance.”
I’ve always been fascinated by those describing a “new finding” in medicine. I am reminded of the story of 5 men who, never having seen an elephant before, were blindfolded and asked to describe what he discovered. However, each man was introduced to a different part of the elephant. Each of them had a dramatically different description of the elephant and each made a conclusion that was very different from the others.
What is fascinating, is that we usually make our “blindfolded comparisons” to those things we have seen or about which we have some descriptive understanding. Observing and describing human physiology is much like examining an elephant while blindfolded for the first time.
This week’s “blind-folded finding” is what has been interpreted by some as “insulin resistance” made worse by a ketogenic diet. Really? This perked my curiosity, because I’ve personally been following a low-carbohydrate/ketogenic diet for years and have thousands of patients doing the same. To this day, I’ve never seen insulin resistance “get worse.” In fact, it gets better. Clinically, it seems to take about 18-24 months to improve, but, it usually gets better.
THE QUESTION –
I’ve had three people from around the world contact me this week and ask why, after being on a ketogenic diet and “in ketosis,” they suddenly get a notably large blood glucose spike when they cheat. By notably large, I mean that their blood sugars rise to over 200 mg/dl within 2 hours of a carbohydrate containing meal. Now, they admit to rapid glucose recovery within an hour or two, and their hemoglobin A1c levels are subjectively normal (less than 5.6%). The worry is “am I becoming diabetic?” They also complain that after having been in ketosis for longer than 3-4 months, they cannot get their fasting blood sugars below 100 mg/dl.
Those asking me the question about this anomalous “physiological insulin resistance” referred to a couple of off-the-cuff blogger’s posts from 2-3 years ago referencing a few small studies (some of which were very poorly designed) [here, here, here & here] in the journals from 10-20 years ago. These articles describe a physiologic response interpreted as worsening “insulin resistance.” However, if you understand what is actually occurring in the Ketonian (yes, I made that term up – there will soon be a whole village of us), I see it as a normal physiologic response. It is misinterpreted by those who’ve never actually seen long term ketogenic physiology, as anomalous, in the average human.
THE ANSWER –
I’ve been seeing this slight elevation in fasting blood sugar with normal or low normal HbA1c in myself and many of my patients for quite some time. However, I never saw it as “insulin resistance” worsening. Clinically, when I tease out the food logs, it usually ends up being protein intake is too high, the person is using a sweetener or creamer causing rebound morning glucose elevation or, in those with low normal HbA1c’s (4.3-5.6%), it is in actuality a protective mechanism of “physiologic glucose sparing” in the keto-adapted individual (1, 2).
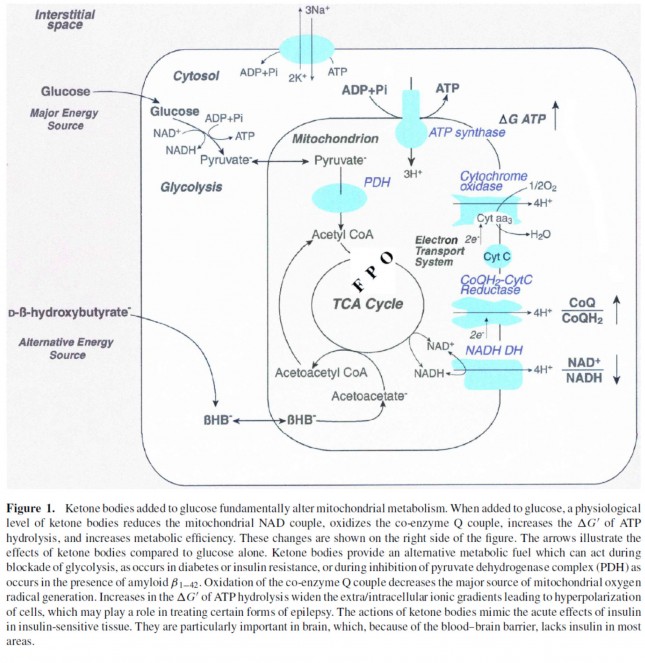
It can very easily be explained when one understands how ketones are actually used in the keto-adapted individual. First, a wonderful figure below (Thank you for pointing me to this one, Dr. Peter Attia) found in Dr. Veech et. al.’s paper (3) gives us an overview of how ketones skirt the TCA cycle within the mitochondria of the cell, causing inhibition of pyruvate dehydrogenase leading to glucose sparing by the cells of the brain that still require it’s availability (Oh, by the way, this is how we survived harsh winters and famines).
From the Figure 1 above, you can see that beta-hydroxybuterate [BHB (a ketone)] is converted to acetoacetyl CoA leading to the production of pyruvate, block-aiding additional glycolysis or inhibiting further glucose production at the liver level. Because the muscle tissues become more adept at using BHB, GLUT receptors are down-regulated at the muscle level as a person becomes more keto-adapted. Although we still have much to learn about the keto-adapted state, we know that this occurs more prominently in the muscle tissues than in the gut and brain. This fascinating glucose sparing phenomenon, has been interpreted by some as “worsening insulin resistance.”
Not to worry, glucose sparing is rapidly reversible and transitory within 1-3 days of increasing carbohydrate intake above 100-150 grams per day (1). It is also why those who become keto-adapted get a carbohydrate hangover including headache, stomach cramps, diarrhea, and malaise lasting 8-24 hours after cheating.
Is this bad? Absolutely not! It is NORMAL! (It’s just that most people, physicians included don’t know what the normal physiology of the Ketonian should look like.) Is it going to kill you, cause a stroke or give you a heart attack? Absolutely not. The elevated BHB actually increases production of adiponectin, leucine & glutathione that have antioxidant properties protecting one from transient inflammatory rises in blood sugar, enhancing insulin’s effect on the muscle, and preserving muscle mass while allowing for fat metabolism (4, 5, 6).
THE TAKE-HOME MESSAGE –
First, don’t cheat if you don’t want to see transient rises in blood sugar and experience the wonders of a carbohydrate hangover and some mild reactive hypoglycemia (low blood sugar) after the fact.
Second, if you’ve been in ketosis for longer than 3-4 months, and you absolutely must get another two or three hour oral glucose tolerance test (OGTT), you might want to increase your carbohydrate intake to 50-100 grams per day 1-3 days before the test to avoid an anomalous spike in blood glucose. (One OGTT was enough for me . . . but hey, some of us are gluttons for punishment.)
Third, enjoy your eggs, pass the bacon and stir me up some Keto//OS.
KetoOS – Drinkable Exogenous Ketones
References:
Kinzig KP, Honors MA, Hargrave SL. Insulin sensitivity and glucose tolerance are altered by maintenance on a ketogenic diet. Endocrinology 151: 3105–3114, 2010.
Oliveira Caminhotto R, Lima FB. Impaired glucose tollerance in low-carbohydrate diet: maybe only a physiological state. American Journal of Physiology – Endocrinology and Metabolism Published 15 December 2013 Vol. 305 no. 12, E1521 DOI: 10.1152/ajpendo.00580.2013
Veech RL, Chance B, Kashiwaya Y, Lardy HA, Cahill GF Jr. Ketone bodies, potential therapeutic uses. IUBMB Life. 2001 Apr;51(4):241-7.
I thought that over the next few weeks I’d address a number of Ketogenic Lifestyle Rules that I have adopted. These seem to help and bring a little clarity to one following a Ketogenic Lifestyle or someone on the road to becoming a true “Ketonian.”
The first of these rules is that there should ALWAYS be bacon in the fridge!
We address this rule and some interesting facts around having bacon in the fridge in this evening’s Persicope below. We also address the benefits of journaling, how to help stop binge eating, what are your real protein needs, and red-meat fear-mongering. We even discuss whether or not pigs like bacon. Enjoy!
(Just a note: I love Katch.me’s service; however, due to the contract language allowing Katch.me to have unlimited rights to my Periscope Videos, I have withdrawn from Katch and my videos are no longer available on this medium until the contract usage can be modified.)
The image above has nine dots within a square. Your task, using only four lines is to connect ALL nine dots WITHOUT ever raising your pen, pencil or finger (Please don’t use a sharpie on your computer screen . . . it doesn’t come off).
You may have seen this puzzle previously . . . it’s made its rounds in corporate training circles. But the underlying principle remains true. The solution requires you to expand your thinking or to “think outside the box.”
Whenever you find yourself on the side of the majority, it is time to pause and reflect. (Mark Twain)
Why should we limit ourselves to thinking outside the box. Can’t we just get rid of the box?
True discovery consists in seeing what everyone has seen . . . then, thinking what no one has thought.
The answer can be found when those four lines are used beyond the box our mind creates:
What good has the box done us? People were burned at the stake because they refused to believe the Earth was not the center of the universe. People were beheaded because they had a sneaking suspicion that the world was not flat.
Why is it so very hard to accept that our weight gain and diabetes are driven by a hormonal signal, and not by gluttony or caloric intake of fat? The definition of insanity is doing the same thing repetitively and expecting a different outcome. How long have you been restricting calories and fat with only minimal or no improvement in your weight, blood sugar, cholesterol or general feeling of health?
The main problem with the current thought model, or dogma, on the obesity’s cause is that it does not account for metabolic syndrome. Metabolic syndrome is insulin resistance. It is an over production of insulin in the presence of ANY form of carbohydrate (sugar or starch).
In the practice of medicine over the last 15 years, I noticed that a very interesting pattern emerged. There was always a spike in fasting and postprandial insulin levels 5-10 years prior to the first abnormal fasting and postprandial blood sugars. These patients were exercising regularly and eating a diet low in fat. But they saw continued weight gain and progressed down the path of metabolic syndrome. 10-15 years later, they fall into the classification of type II diabetes. What I now lovingly refer to as stage IV insulin resistance.
The only thing that seems to halt this progressive process with any degree of success is carbohydrate restriction. Fasting insulin levels return to normal, weight falls off, and the diseases of civilizations seem to disappear as insidiously as they arose.
So you tell me, is the world flat? Is the Earth the center of the universe?
What is a low carbohydrate or ketogenic diet? 15 years of practical in the trenches experience have helped me develop a very simple program to help you lose and maintain your weight. Access to this program, video help and access to blog articles at your fingertips are offered through my online membership site.
You can also hear me each week a I discuss low carbohydrate, paleolithic and ketogenic diets with the Legendary Jimmy Moore on KetoTalk.com
Good morning from Arizona. I’ve had a few people ask about how gut health relates to a ketogenic diet. This is a great question and one that I think can be answered best by taking a closer look at my natural koi pond and learning a little about pond scum.
So, sit back and look at the similaries between your gut and how nature balances a pond system: Katch.me
Or you can watch the video below:
The four tenets of health that we touch on above that are essential to understand before you can understand gut health:
The body is a unit and works as such with all parts enhancing the whole
The body is capable of self-regulation, self-healing, and health-maintenance
Structure & function are reciprocally interrelated
Rational treatment of the body must be based upon understanding the principles above and assisting or augmenting those principles
Keys to gut health and pond balancing that we touch on:
Remove the toxins from entering the system like:
Antibiotic overuse
Caffeine
Artificial Fat
Artificial Sweeteners
Repair the system and it’s ability to balance the system
Takes time
Provide structure for the bacteria to which it can bind
Provide essential vitamins and minerals like KetoEnhance & Omega-3 fatty acids
Periodic Fasting
Restore the bacteria or flora of the system
Prebiotics (fermented foods like sauerkraut, kimchi, Japanese natto, etc.)
Probiotics like Dietary KetoBalance (can be purchased in the office)
Replace the salts and pH balance where necessary
Replace electrolytes
Limit things that shift the pH balance
Hope this gives you a starting point for your New Year!!
KetoTalk with Jimmy & the Doc (the legendary podcaster Jimmy Moore from Livin’ La Vita Low Carb and his newest co-host, your’s truly, Dr. Adam Nally) makes its debut this Thursday, December 31st, 2015 on iTunes. You can see the show notes at KetoTalk.com (will be up and live on January 1st, 2016).
Throughout the exciting month of January, we will be airing a brand new episode of this 20-minute show each Thursday and a special bonus episode available on Sundays just to wet your ketogenic appetite and to kick off the podcast in its first month. Then, in February we’ll settle in to our regular Thursday time slot each week.
New podcasts can take a few days to assimilate into #iTunes, so don’t get discouraged if you don’t immediately see it up on iTunes. However, you can always find them at KetoTalk.com. Jimmy and I look forward to being your go-to, Ketogenic Lifestyle source for the latest and greatest in treating the diseases of civilization!
Get a sneak peek of our new show on tomorrow’s (Wednesday, December 30th) episode of “The Livin’ La Vida Low-Carb Show” where you can hear my interview with Jimmy as a preview what is sure to be a big hit in the #keto community. Thanks in advance for supporting our new podcast!
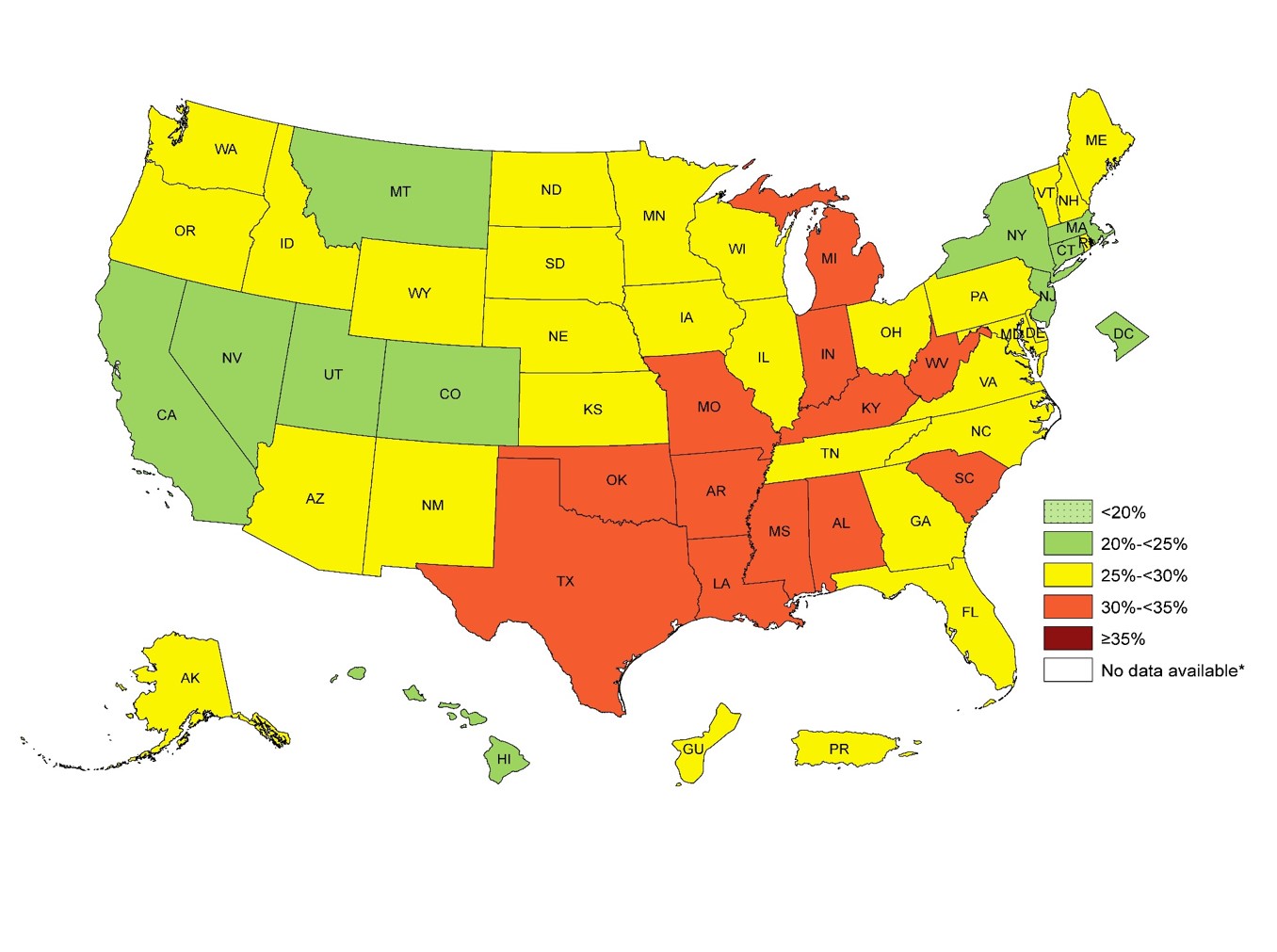
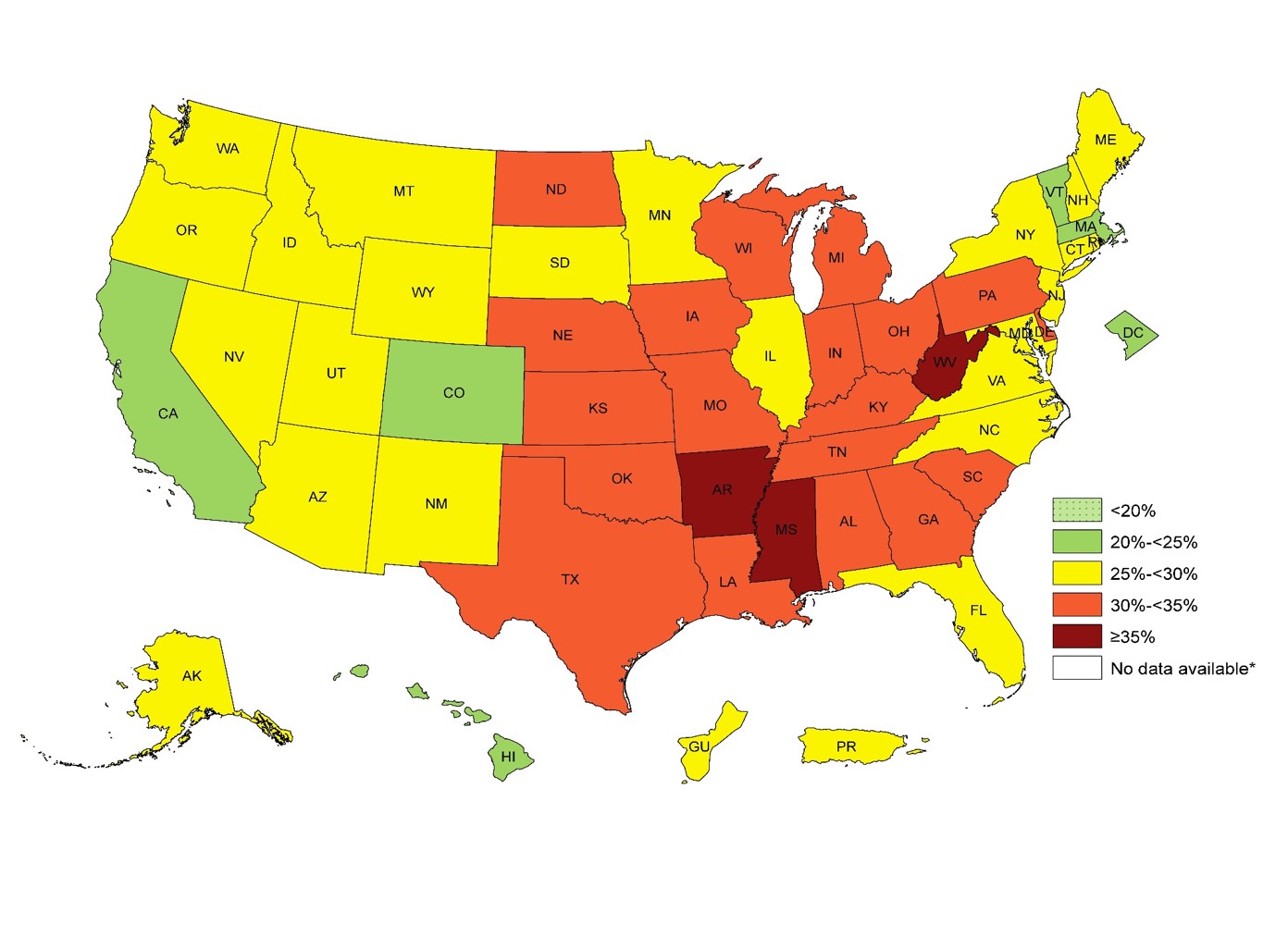
Today in the office I had the calorie conversation again . . . three times. We have an entire society with a very influential health and fitness industry built around the almighty calorie. Has it helped? Looking at our 5 year obesity outcomes. It hasn’t helped a bit. In fact, it is worse. In 1985 only 19% of U.S. adults were obese.
U.S. Obesity Adult 2011U.S. Adult Obesity 2014
In 2014, 34.5% of U.S. adults were obese. The numbers this year are approaching 35.6% You can see the dramatic increase in obesity by 1-3% every year for the last 5 years in the CDC images above.
For over 50 years we have been told that caloric restriction and fat restriction is the solution. But by the numbers above, the 58 million people in the U.S. utilize a gym or health club to burn off those calories aren’t seeing the success that they should be expecting.
Why? Because the calorie is NOT king. What do I mean by that? We don’t gain weight because of the thermogenic dogma we’ve been taught for the last 50 years. Our weight gain is driven by a hormone response to food. Hear more about why the calorie is NOT king on tonight’s PeriScope. You can Katch it here with all the live stream comments and hearts at Katch.me/docmuscles.
Or you can watch the video without the comments here:
Today’s Periscope was an exciting one. Do you really need a pre- or post-workout shake or meal? How much protein do you need? What’s the difference between ketosis and ketoacidosis? Is Dr. Nally a ketogenic cheerleader? Get your answers to these and many more questions asked by some wonderful viewers this evening on today’s PeriScope.
Be sure to check out Dr. Nally’s new podcast called “KetoTalk with Jimmy and the Doc” with the veteran podcaster Jimmy Moore on KetoTalk.com. The first podcast will be available on December 31, 2015. KetoTalk with Jimmy and the Doc will be available for download for free on iTunes.
What are the three things you need to successfully weather the holidays with your ketosis lifestyle? What does a raindeer on a motorcycle look like? How does insulin resistance effect kidney stones and gout? How do you get back on track if you fall off the ketosis wagon? These and many more questions are answered by Dr. Adam Nally on tonight’s PeriScope.
You can see the video stream including the comment roll here at katch.me/docmuscles. Or you can watch the video below:
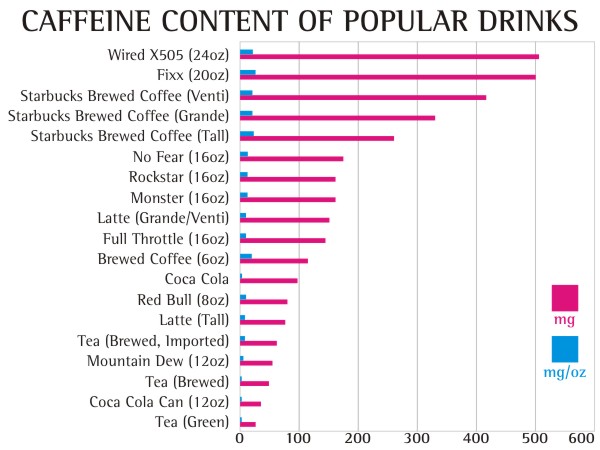
I’ve been looking for the answer for quite some time. . . what role does caffeine play in your and my weight management journey? The answer gave me a headache. . . literally and figuratively.
As many of you, including my office staff, know, I love my Diet Dr. Pepper (and my bacon). I found that being able to sip on a little soda throughout the day significantly helped the carbohydrate cravings and munchies during a busy and stressful day at the office. Diet Dr. Pepper contains caffeine, however, I wasn’t really worried. Caffeine has been well know to have a thermogenic effect which increases your metabolism and has been thought for many years to help with weight loss among the weight loss community.
Diet Dr. Pepper is, also, one of only four diet sodas on the grocery store shelves that doesn’t contain acesulfame potassium (click here to see why most artificial sweeteners cause weight gain). The four diet sodas that I have been comfortable with my patients using are Diet Dr. Pepper, Diet Coke, Diet Mug Root-beer and Diet A&W Cream Soda. These are the last four hold out diet sodas that still use NutraSweet (aspartame) as the sweetener. Most of the soda companies have switched the sweetener in their diet sodas to the insulinogenic acesulfame potassium because it tastes more natural and aspartame has been given a media black eye of late. However, NutraSweet (aspartame) is the only sweetener that doesn’t spike your insulin or raise blood sugar (click here to find out why that is important).
Yes, I know. The ingestion of 600 times the approved amount of aspartame causes blindness in lab rats (but we’re not lab rats, and . . . have you ever met someone that drinks 600 Diet Dr. Peppers in a day? The lethal dose of bananas, which are high in potassium that will stop your heart, is 400). Aspartame can also exacerbate headaches in some (about 5% of people) and I’ve had a few patients with amplified fibromyalgia symptoms when they use aspartame. But for most of us, its a useful sweetener that doesn’t spike your insulin response, halting or causing weight gain.
But, over the last few years, I’ve noticed that increased amounts of Diet Dr. Pepper & Diet Coke seem to cause plateauing of weight and decreasing the ability to shift into ketosis, especially mine. I’ve also noticed (in my personal n=1 experimentation) that my ability to fast after using caffeine regularly seems to be less tolerable, causing headaches and fatigue 8-10 hours into the fast, symptoms that don’t seem to let up until eating. Through the process of elimination, caffeine seems to be the culprit.
After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the August 2004 Diabetes Care Journal screamed for my attention.
It appears that caffeine actually stimulates a glucose and insulin response through a secondary mechanism. The insulin surge and glucose response is dramatically amplified in patients who are insulin resistant. Caffeine doesn’t effect glucose or insulin if taken while fasting; however, when taken with a meal, glucose responses are 21% higher than normal, and insulin responses are 48% higher in the insulin resistant patient. Caffeine seems to only effect the postprandial (2 hours after a meal) glucose and insulin levels. The literature shows mixed responses in patients when caffeine is in coffee or tea, probably due to the effect of other organic compounds (1).
Caffeine effect on plasma glucose and plasma insulin compared to placebo (1).
Caffeine also diminishes insulin sensitivity and impairs glucose tolerance in normal and already insulin resistant and/or obese patients. This is seen most prominently in patients with diabetes mellitus type II (stage IV insulin resistance). Caffeine causes alterations in glucose homeostasis by decreasing glucose uptake into skeletal muscle, thereby causing elevations in blood glucose concentration and causing an insulin release (2-6).
Studies show that caffeine causes a five fold increase in epinephrine and a smaller, but significant, norepinephrine release. The diminished insulin sensitivity and exaggerated insulin response appears to be mediated by a catacholamine (epinephrine, norepinephrine & dopamine) induced stress response (5). Caffeine has a half life of about 6 hours, that means the caffeine in your system could cause a catacholamine response for up to 72 hours depending upon the amount of caffeine you ingest (7).
The reason for my, and other patient’s, headaches and fatigue after a short fast was due to the exaggerated stress hormone response. Increased levels of insulin were induced by a catacholamine cascade after caffeine ingestion with a meal, dramatically more amplified in a person like me with insulin resistance. The caffeine with the last meal cause hypoglycemia 5-7 hours into the fasting, leading to headaches and fatigue that are only alleviated by eating.
Even when not fasting, the caffeine induced catacholamine cascade causes up to 48% more insulin release with a meal, halting weight loss and in some cases, causing weight gain.
Caffeine is not the “Wonder-Boy” we thought it was.
How much caffeine will cause these symptoms? 50 mg or more per day can have these effects.
10,000 mg (10 grams) – lethal dose (Yes, 25 cups of Starbucks Coffee can kill you)
The equivalent of 100 mg of in a human was given to a spider, you can see the very interesting effect on productivity. How often does the productivity of the day feel like the image below?
Normal Spider (9)Spider on caffeine (9)
Beware that caffeine is now being added to a number of skin care products including wrinkle creams and makeup. Yes, caffeine is absorbed through the skin, so check the ingredients on your skin care products.
Diet Dr. Pepper, my caffeine delivery system of choice, has slightly less caffeine (39 mg per 12 oz can or 3.25 mg per oz) than regular Dr. Pepper. I found myself drinking 2-3 liters of Diet Dr. Pepper per day (long 16-18 hour work days in the office). After doing my research, I realized that my caffeine tolerance had built up to quite a significant level (230-350 grams per day).
So, a few weeks ago, I quit . . . cold turkey.
Did I mention the 15 withdrawal symptoms of caffeine? (8)
Headache – behind the eyes to the back of the head
Sleepiness – can’t keep your eyes open kind of sleepiness
Irritability – everyone around you thinks you’ve become a bear
Lethargy – feels like your wearing a 70 lb lead vest
Constipation – do I really need to explain this one?
Depression – you may actually feel like giving up on life
Muscle Pain, Stiffness, Cramping – feel like you were run over by a train
Lack of Concentration – don’t plan on studying, doing your taxes or performing brain surgery during this period
Flu Like Illness – sinus pressure and stuffiness that just won’t clear
Insomnia – you feel sleepy, but you can’t sleep
Nausea & Vomiting – You may loose your appetite
Anxiety – amplified panic attacks or feeling like the sky is falling
Brain Fog – can’t hold coherent thoughts or difficulty with common tasks
I experienced 13 of the 15 that lasted for 4 days. I do not recommend quitting cold turkey unless you have a week off and someone to hold your hand, cook your meals and dose your Tylenol or Motrin. My wife thought I was dying. . . I thought I was dying on day two. I actually had a nightmare about buying and getting into my own coffin. It can take up to three weeks to completely recover from caffeine withdrawal.
The other way to quit is to decrease your caffeine intake by 50 mg every two days. That means decrease caffeine by:
1 can of soda every two days
1/4 cup of coffee every day
1/2 can of Energy Drinks every two days
1 cup of tea every two days
The benefit of this method is that withdrawal symptoms are much less severe without the caffeine headache and the ability to remain productive. It will take longer, but quitting cold turkey is not a pretty picture. Been there . . . done that, . . . and I’m not going back. I actually lost another half inch off my waistline by day 5 of caffeine discontinuation.
What is the take home message here? If you have any degree of insulin resistance, caffeine makes it worse and will amplify your weight gain as well as decrease the productivity of your day.
How do you know if you're insulin resistant? What questions need to be asked? What should your numbers be? And, many other great ketosis questions. Also, why does Dr. Nally look like he has dirt on his chin? See it here . . .
This evening on PeriScope, we talked about the 10 things you can do to stay motivated on your low-carb lifestyle. A number of great questions were asked including:
How much carbohydrate should be restricted?
What labs should you be monitoring regularly?
What’s a normal blood sugar?
Why is Dr. Nally freezing in Denver?
Is fermented food good for you?
Why should you eat pickles and kimchi even when you’re not pregnant?
And, much much more . . . It’s like a college ketogenic course on overdrive . . . for FREE!!!
You can see the PeriScope with the comments rolling in real-time here: katch.me/docmuscles
Today’s Periscope with Jimmy was a teaser for what is to come. I will be joining Jimmy Moore to create a new weekly podcast to address “Keto Questions” you may have. Stay tuned for more information . . .









 raise insulin levels without raising blood sugar and are not appropriate for use with a true low-carbohydrate/ketogenic diet. You can see and print the article I published clarifying which sweeteners you can use and which ones to avoid here:
raise insulin levels without raising blood sugar and are not appropriate for use with a true low-carbohydrate/ketogenic diet. You can see and print the article I published clarifying which sweeteners you can use and which ones to avoid here:
















 After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the
After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the 

{kind=link}