I’m not sure what it is about this time of year . . . maybe the post-holiday weight gain, or the fear of pulling out a swimming suit in a few months. But I have had a number of people, both men and women, in the office with excessive estrogen levels.
Estrogen excess and estrogen dominance are two hormone abnormalities I find commonly in both men and women in my practice. These two issues are frequently complicating factors that make feeling good and weight loss difficult. They are, also, often the main reasons people don’t see dramatic improvement in a person’s symptoms of energy, fatigue and mental clarity when they’ve already changed their diet and lifestyle.
IMPORTANT NOTE BEFORE WE GO ON: This information applies to patient who already have normal thyroid function and corrected insulin resistance. If your thyroid is off or if you are still significantly insulin resistant, it will affect estrogen and other male and female hormones, so follow a ketogenic diet and get your thyroid balanced FIRST!
What is Estrogen Dominance?
I’ve addressed estrogen dominance in a previous blog post. You can find it here. Estrogen dominance is a condition where there is an abnormal estrogen/progesterone ratio. The estrogen/progesterone ratio MUST be balanced. Normal estrogen levels with low progesterone (this can commonly occur with the use of a synthetic progestin (HRT) in female patients) is a common scenario that falls into the estrogen dominance pattern.
What is Estrogen Excess?
Estrogen excess is a situation where progesterone levels may be normal but estrogen is elevated (an abnormal ratio can also be present in this condition).
The symptoms of excess estrogen can be:
Depression
Fatigue
Poor Concentration
Irregular menstrual bleeding in women
Breast tenderness
Fibrocystic Breast Changes
PMS
Decreased Libido
Uterine Fibroids
Endometriosis
Water Retention/Bloating
Fat Gain around the hips and thighs
Breast and Uterine Cancers
Why is too much estrogen a problem?
Estrogen naturally stimulates cells to grow and multiply. Natural estrogens are essential. But, too much estrogen increases thyroid binding globulin, inactivating the thyroid function causing abdominal weight gain. Too much estrogen changes the body’s ability to remodel bone.
Estrogen is essential to stabilize the inner lining of arteries, however, excessive estrogen doubles one’s risk for stroke and increases the risk of coronary atherosclerosis and heart attack. Too much estrogen increases the size of the prostate, increases risk of prostate cancer and increases the risk of rheumatoid arthritis.
Estrogen excess is an elusive condition. Measuring estrogen levels is not frequently done, and most doctors were never trained to look at the three separate forms of estrogen in men and women. I had no idea this was an issue until about five years ago.
What causes excess estrogen?
The eleven most common causes of estrogen excess are:
Commercially raised meat & dairy products from animals dosed with high levels of bovine growth hormone.
Insecticide or pesticide residues on fruits and vegetables.
Tap water with petroleum derivatives
Paraben containing shampoo, lotion, soap, toothpaste, & cosmetics. Paraben is absorbed through the skin. There is a 100% absorption that misses first pass liver detoxification
Pthalates – soft plastic containing material or plastic wrapped food heated in the microwave releasing xenostrogens into the food.
Artificial sweeteners including MSG (propyl-gallate and 4-hexylresorcinol are the two most common). Canned foods that have been lined with a plastic coating called BPA (bisphenol-A). Most processed foods have some additive that you will want to avoid.
Foods containing soy or soy protein isolate contain unnaturally high amounts of plant estrogens (phytoestrogens).
Red dye #3 (erythrosine and phenosulfothiasize) found in food
Dryer Sheets containing high levels of xenoestrogens. Chronic skin exposure leads to permeation of the xenoestrogens into the skin.
Birth control pills (conventional synthetic estrogen containing hormone replacement)
Tampons and sanitary napkins containing dioxins, chlorine, fragrance, wax, surfactant, and rayon play a role in significant xenoestrogen absorption.
Other diseases can cause estrogen ratio’s to be elevated. These include liver disease, zinc deficiency, excessive alcohol intake, obesity, calcium deficiency, insulin resistance, diabetes, and excessive testosterone therapy.
How does a person naturally decrease excess estrogen if it is present?
Decrease xenoestrogen exposures:
Reduce use of plastics where possible
Do not microwave food in plastic containers
Avoid the use of plastic wrap to cover or microwave the food
Use glass or ceramic containers where possible
Do not leave plastic water containers, especially drinking water, in the sun
If a plastic water container was heated up significantly (like a water bottle being left in the car in the Arizona sun), throw it away.
Don’t refill plastic water bottles
Avoid freezing water in plastic bottles for drinking later
Avoid butylated hydroxyanisole (BHA) as a food preservative
Limit skin care products containing xenoestrogenic substances
Use cruciferous vegetables like broccoli that contain indole-3carbiol (I3c).
Increase Omega-3 fat intake
Exercise
Use rosemary and turmeric (berberine)
Reduce weight
Use Vitamin D
Stop drinking alcohol
Stop smoking
These hormones, like estrogens, progesterone and testosterone can be easily checked by your doctor through blood or salivary testing. The key is a balance in the ratio between progesterone and estrogens.
The two estrogens that are essential to test are:
Estrone (E1)
Estradiol (E2)
These can be ordered through your doctor. Estrogens can take 2-3 months to balance out. It may take some time after making changes to see your levels normalize. Don’t fret.
What if natural methods don’t fix the problem?
When natural methods of lowering estrogen levels are ineffective, then your doctor will recommend treatment. A number of other effective medicinal approaches including:
In my clinical experience, a ketogenic lifestyle is foundational to balancing these hormones consistently and naturally. Carbohydrate restriction by itself corrects many of the diseases of civilization. I addressed this in my book The Keto Cure. For many, there are few more steps necessary to living a long, happy and healthy life.
In my office, in addition to the ketogenic or carnivorous diet, I add on Berberine Plus 500mg twice daily with meals. This has been shown to notably improve the insulin resistance, lower estrogen and improve progesterone naturally.
Years ago, this was hard to find, so I created my own supplement line and these can be found at Ketoliving.com. Go to Ketoliving. com and order your bottle of Berberine Plus right now, before it is too late. I designed my own pharmaceutical grade berberine so that my patients could make sure they are getting real berberine in the doses I want you to have.
The treatment of this issue isn’t difficult. There is much more to come on this subject. I will address each of the progesterone, testosterone, DHEA and sex hormone binding globulin abnormalities in my future blogs. So, keep an eye on my web page DocMuscles.com/blog/.
So, get your hormones checked by someone who understand this problem and knows how to treat it. Second, limit estrogen stimulating sources in your diet and environment. Third, control you diet and order a bottle of Berberine Plus right away.
Hair loss is an issue that I am asked about quite frequently. With any dietary change, transient hair loss can occur in the first 2-3 months but will usually resolve. Continued hair loss is a problem with any diet and if you are experiencing hair loss it could be due to one of five issues:
1. Medication
2. Lack of protein or caloric restriction
3. Hypothyroidism
4. Iron Deficiency
5. Hormone imbalance (especially estrogen dominance or poly-cystic ovarian syndrome)
Dr. Nally discusses these and how to address them in his most recent YouTube video. Check it out below.
What do you do when you hit a weight loss stall while living a ketogenic lifestyle? Find out below. Dr. Nally goes into detail on the multiple causes of stalling while following a low-carbohydrate or ketogenic lifestyle. He dispels the myths around counting calories and macros. And, he discussed the basics of overcoming a stall.
Watch as we discuss the important markers of heart disease and vascular disease risk. We will talk about how these markers can help you understand what your body is doing in the process of making or reversing atherosclerosis (plaque in the vessels). And, should you really be taking that STATIN (cholesterol lowering) drug? Get the scoop here as Dr. Nally very simply points out how the right diet can and will lower your cholesterol without the use of medications.
Research in the last 10 years points to the small-dense LDL particle as the atherogenic component of cholesterol (Hoogeveen RC et al., Arterioscler Thoromb Vasc Biol, 2014 May; Ivanova EA et al., Oxidative Med Cell Longevity, 2017 Apr). Studies in the last five years have identified that elevated small-dense LDL cholesterol correlates much more closely with risk for inflammation, heart disease and vascular disease (Williams PT, et al. Atherosclerosis. 2014 April; 233(2): 713-720.)
Recent research in the last three years demonstrates that small dense LDL cholesterol is a better marker for prediction of cardiovascular disease than total LDL-C (Hoogeveen RC et al., Arterioscler Thromb Vasc Biol. May 2014, 34(5): 1069-1077l; Ivanova EA et al., Oxidative Med Cell Longev. 2017).
Additionally, higher LDL-C is actually predictive of longer life and has been demonstrated to correlate with longevity (Ravnskov U et al., BMJ Open, 2016 Jun 12;6(6): e010401). And, a low LDL-C actually increases risk of early mortality (Schwartz I et al., Lancet 2001, 358: 351-55).
It is commonly understood that LDL-C will rise with increased saturated fat intake on a ketogenic diet. This has been know and reported in the scientific literature for over twenty years. This is to be expected, because LDL-C is really a measurement of three different LDL sub-particles (“big fluffy, medium, and small dense”). Increased saturated fat intake, while at the same time lowering carbohydrate intake, actually causes a shift in these low density particles to a bigger “fluffier” particle conformation (Griffin BA et al., Clin Sci (Lond), 1999 Sep).
The 2015 British Medical Journal, referenced above, analyzed the relevant 19 peer reviewed medical articles that included over 68,000 participants. This review showed that there is no association of high LDL-C with mortality (meaning that an elevated LDL-C does not lead to an increased risk of death from heart or vascular disease). I realize that, in stark opposition to the landmark review above, The American Heart Association’s Presidential Advisory published their position in the June 20, 2017 issue of Circulation. They stated that saturated fat is the cause of increased LDL-C and they further extrapolated that elevated LDL-C is associated with an increase in death by cardiovascular disease. This boldfaced claim is only based on one single small four year (2009-2013) literature review completed by the World Health Organization with a total of only 2353 participants, most of these studies only lasting 3-5 weeks (not nearly long enough to see fully effective cholesterol changes) and none of which had any focus on carbohydrate intake, insulin levels or LDL sub-particle measurement (Mensink RP, Geneva: WHO Library Cataloguing-in-Publication Data, 2016).
Based upon the most current scientific evidence above and my clinical experience, the large body of evidence above demonstrates the use of total cholesterol and LDL-C to determine vascular disease risk to be ineffective tools. A low carbohydrate/ketogenic diet lowers small dense LDL cholesterol, triglycerides and blood sugar and in many cases, the use of cholesterol drug (STATIN) therapy is not needed and ineffective in comparison with a ketogenic/carbohydrate restricted lifestyle.
Catch my new video. I go into depth regarding why the type of fat you eat is very important on a ketogenic lifestyle. I reviews the effects of short, medium and long chain fats and how they are absorbed and used. We talk about starting a ketogenic diet and answer multiple viewer questions. Check it out!
Over the last 18 years of my practice, I’ve seen tremendous success in helping people improve their health when low-carbohydrate dietary changes are anchored as the foundation of treatment. However, there is still a group of people that struggle with seeing success. Even with the most effective ketogenic dietary control, there are those that see abnormal weight gain, inability to lose weight, poor libido, fatigue, foggy thinking, mood swings, persisting depression, headaches, bloating, breast tenderness, fibro-cystic breast changes, hair loss, and hot flashes. They may not experience all these symptoms, however, many are often present. If you have been following a ketogenic lifestyle and are still experiencing any of these symptoms, you are probably suffering from estrogen dominance.
Estrogen dominance is a condition that elusively effects thousands of women (and men) and your doctor probably doesn’t even know about it. I didn’t know about it. I, like all of my physician colleagues, were trained in school that the symptoms above are related to fluctuations of estrogen as a woman ages (or dropping of testosterone as a man ages). We were, and still are, taught that they are fixed by giving more powerful doses of estrogen or testosterone.
Over the years of my clinical experience, giving more estrogen frequently didn’t work. And, giving men more testosterone didn’t work either. What I found very effective, for many, was changing the diet. And, for about 85% of people, the symptoms list above resolved. However, the cause of the symptoms above in that last 15% of patients I see was still elusive. Examinations, blood tests, and even psychological evaluations never revealed the answer. Giving synthetic estrogen, progestin or testosterone when the blood work showed abnormality partially alleviated some of the symptoms for a few months, but then the patients would end up back in my office with the symptoms having returned.
I’ve found a number of problems following the “standard” medical approach to using synthetic sex hormones.
The first problem is that estrogen, progesterone and testosterone are heavily bound to proteins in the blood. It is only the free component of the three forms of estrogen and progesterone in the body and the free testosterone that acts upon the delicate cells located throughout the body. Blood testing does not account for the levels of free estrogen forms and progesterone effectively. These can only be tested through salivary testing.
The second obstacle is that the synthetic forms of progesterone (progestin), cannot effectively enter the brain. When synthetic forms are used, a person only gets half the benefits of progesterone found in the human body. This is why so many women have depression, anxiety and foggy brain feelings when using the synthetic versions.
The third challenge is that pharmaceutical companies cannot patent a drug that is identical to your human hormones. The chemical structure of the synthetic estrogen, progestin or testosterone must be slightly different. Hormones effectively work on certain aspects of various cells throughout the body, however, progesterone and progestin (the synthetic version found in medroxyProgesterone) DO NOT have the same hormonal effect on each cell. Natural progesterone is broken down by the stomach when ingested. That’s why progestin was invented, however, it doesn’t act the same in the body and only does half the job.
The fourth dilema is that much of our food in the standard American Diet stimulates increased estrogen production or inhibits clearance of estrogen excess through the gut and digestive tract. This happens in men and women. We can get excess estrogen from animals treated with hormones in meats, milk and dairy products. Hydrogenated oils in processed foods change the way estrogen and progesterone are handled in the body. These unstable fats increase the effects of estrogen on the body and amplify the risk for cancers. Excessive omega-6 fatty acids in the diet magnify estrogen receptor response to estrogen.
Estrogen metabolism in the liver and removal in the gut are dependent on vitamins B & E, magnesium and idol-3-carbinol (IC3). Diets without adequate IC3 from glucobrassicin found in leafy green and crucirferous vegetables allow re-uptake of estrogen in the gut leading to high estrogen levels and estrogen dominance. This is where gut health is even more important, and where I see failure in the “carnivore” approach to a ketogenic lifestyle.
The fifth problem is that the more estrogen I give a person, the more estrogen receptors are unregulated to the surfaces of the cells in the body. When that happens, more estrogen is required. Excess estrogen can actually cause many of the same symptoms present in progesterone deficiency including:
Irregular or heavy bleeding
Breast tenderness
Depression
Fatigue
Poor concentration
Fibrocystic breast changes
Decreased libido
Fibroid growth on the uterus
Endometriosis
Water retention and bloating
Fat gain around hips and thighs
Bone mineral loss (osteoporosis)
Hair loss
Skin thinning
Disturbed sleep
Breast and uterine cancer
More estrogen isn’t needed. Balancing natural progesterone with the current estrogen the body is already making is the solution in most cases. This can only be effectively assessed through a salivary hormone test.
In my clinical experience, a ketogenic lifestyle is foundational to balancing these hormones consistently and naturally. Carbohydrate restriction by itself corrects many of the diseases of civilization. I addressed this in my book The Keto Cure. For many, there are few more steps necessary to living a long, happy and healthy life.
The treatment to this issue isn’t difficult. For that reason, much more is to come on this subject. I will address each of the points above in future blogs. However, the first step is get your hormones checked by someone who understand this problem. And, then knows how to interpret it and treat it.
In my last blog post about willpower, I described habits being neural impulse channels in our brain stimulated by a cue following a path leading to the same outcome each and every time – without exerting much effort. Researchers call the formation of these impulse channels habit-loop cycles. Much of the original obesity research of the 19th century was conducted by psychiatrists and psychologists recognizing that people had habitual eating patterns. Because of this, gluttony became the perceived influence of obesity. This underlying philosophy still permeates the obesity research, treatment and low-carb dietary world today. Yet, over the last 15 years, I’ve found that the habit-loop cycle is tied to powerful hormone responses. These responses to very subtle and often unknown triggers or cues powerfully drive weight gain, obesity and struggles with willpower. How does the habit-loop cycle effect you? Before we can change these habit-loop cycles, we have to understand what they are, and how they were created.
It’s All About That Basal Ganglia
Meghan Trainor tells us that “It’s all about that bass . . .” However, it’s really all about that basal ganglia. Deep inside our brains, close to the brain stem, at the location where the brain meets the spinal cord, is a little “nub” of neurological tissue called the basal ganglia. This little nubbin of tissues was identified by the really smart scientists at MIT in the 1990’s as the location where habits are formed and executed. The brain is – to take a quote from my favorite ogre, Shrek – “like an onion – it has layers!”
The Brain Is Like an Onion
If you picture the outer layers of the brain tissue, those closest to the hair and scalp, you can create a mental image of where our most complex thoughts occur. When you think up a new invention, create a new way to cook with bacon, laugh at a friend’s joke, or link two complex thoughts about how habits form, you are using these outer layers of the brain.
Like an Onion – It Has Layers! (DreamWork’s Shrek, 2001)
However, our interest today is deeper . . . much, much deeper. Deep within the center of the brain at the basal ganglia is the location where our automatic behavior originates. Swallowing, breathing and the startle responses are housed in this little nubbin of brain tissue. It is this area of the brain that learns to recall and record patterns of neurological thought and stimulating action. This part of the brain has the ability, like the water drops on the mound we discussed last week, to record neural pathways and tracks leading to reduced mental effort and habit. The basal ganglia even has the ability to store habits while the rest of the brain is asleep. It is in this location, the basal ganglia, where the habit-loop cycle occurs.
Habits Created by Chunking
The habit-loop cycle is the process where the brain converts a sequence of actions into an automatic routine. The really smart guys at MIT call this “chunking,” and it is the root of habit formation. There are hundreds of behavioral chunking activities that you and I rely upon every day. Some of these are as simple as the process you use to squirt toothpaste on your toothbrush before brushing your teeth. Others are more complex like getting dressed or making a lunch box for the kids.
The Habit-Loop Cycle in Your Car
A habit-loop cycle is performed by this little nubbin of tissue by millions of people every morning. Take, for example, backing your car out of the garage. When you first learned to do this, it required huge amounts of concentration – and for very good reason. You’re steering 3000-5000 lbs of steel between a 16 foot garage-door opening into oncoming traffic.
Safely backing your car requires you to open the garage door, unlock the car, adjust the seat, insert the key into the ignition, turn it clockwise, move the rear-view mirror and the side mirrors to visualize any obstacles, put your foot on the brake, put the car into reverse, gently remove your foot from the brake, mentally estimate the distance between the garage and the street while keeping the wheels straight and looking over your shoulder, applying a slight pressure between the gas pedal and the brake, and in some cases, slapping your teenagers hand while they fiddle with the radio dial.
But think about it . . . did you actually put any thought into these actions this morning? You and I probably did this once or twice today without any additional thought. It happened because the basal ganglia took over and created a habit-loop out of it. This routine, repeated hundreds of times, became a habit, requiring very little mental effort.
Your Basal Ganglia Makes You Fat
The habit-loop cycle occurs hundreds and maybe thousands of times throughout our day. It is the cycle that drives hundreds of our activities. In fact, it is this same cycle, in combination with 30 different hormones, that drives our weight gain or weight loss. Yes, I said it,your basal ganglia can make you fat.
Habits Make for a Smaller Brain
Your brain will try to turn any regular routine into a habit, because habits allow our minds to slow down and conserve effort, energy and fuel. The efficient brain allows us to stop thinking about basic behaviors like walking, breathing and eating. This effort-saving effect of the brain is a major advantage, otherwise our brains would be huge, requiring heads the size of watermelons, or even the size of a water tower, causing their own weather systems. Your wife will thank you for an efficient brain that is smaller and requires less room. Can you imaging giving birth to a watermelon or a small Chevy? (Did you notice the size of Shrek and the Donkey’s head? Just say’n . . . )
Habits Are The Root of Behavior
What all this leads to is this – habits, as much as memory and reason, are the root of our behavior. We often don’t remember the experiences that create our habits. However, once they are created, they influence our action without our own realization. Charles Duhigg’s book, The Power of Habit is a great resource for further information on how habits drive our behavior.
The Habit-Loop of Obesity
So, how does all this affect obesity and weight gain? Let’s, first, look at the habit-loop cycle. Researcher, Larry Squire, documented the habit-loop through three decades of research. He and others published numerous articles showing that habits have a cue or trigger that stimulates a routine. The routine leads to an outcome or reward. The reward usually satisfies a craving. Cue-> Routine -> Reward. What we learn through our studies in obesity is that the reward often stimulates a hormonal response of 1-30 different hormones in brain and body leading to repeat cues or triggers. The cravings are hormonally driven. I call it the Habit-Loop of Obesity.
The Craving is the Key
Human psychology and emotion is the key behind habit creation. First, there must be a trigger or cue. Second, the trigger is attached to a previously experienced emotion or craving tied to the cue. The key to habit formation is the craving. The craving is what stimulates the physical routine to occur. It is an emotion or craving that drives the brain to create the habit. Third, there must be a clearly defined outcome or reward that satisfy the emotion or the craving. The emotion or craving doesn’t have to be associated with hormones, however, in the relm of obesity, it is usually tied together.
I am all about making things easier. Your brain does it. We all do it. And, I’m all about trying to help you lose fat and get healthy more easily. Let food be your medicine, let medicine be your food. That’s my mantra and that is as easy and natural as it gets. But, in our day and age, we don’t always have access to growing and raising our own food. That’s why my second mantra is – better living through chemistry. So, I created the KetoKart. Over the last 15 years of medical practice, I’ve found products and supplements that aid in letting food be your medicine, changing triggers, modifying hormones, and help to satisfy cravings in a healthy way to make your decisions easier. Go to the KetoKart, see which package works for you and order it. You’ll thank me.
How do we change our obesity habits? Stay tuned for the third part in this series: Fixing the Habit-Loop of Obesity.
So, I want to know . . . which package did you choose?
How does ketosis help the diseases of civilization? Find out as Dr. Nally answers these and many other pertinent dietary questions this evening.
You can learn more about his multi-vitamin supplement he designed for insulin resistance/diabetic/weight management patients that he mentions in the video here at KetoLiving.com.
You can learn about exogenous ketones that he mentions helps to augment ketosis here at DymaicKetones.com.
Have you been cutting your calories and reducing fat and exercising your brains out and still not seeing the needle on the scale move that much? Persistently and repetitively performing an action that doesn’t produce the desired result is insanity. Cutting calories and reducing fat while expecting weight loss is akin to pouring water in the gas tank of your car and expecting it to run smoothly. Why do we do it? Are the 53, 000, 000 people with health club and gym memberships this year really insane?
This evening on PeriScope we touch on fat phobic insanity and the limiting step that actually turns weight gain on or off. (We knew about this in the 1960’s, we just ignored it.)
You can see tonight’s PeriScope with the rolling chat-box questions here at Katch.me/docmuscles. Or, you can watch the video stream below:
The only way to successfully loose weight is to modify or turn off the mechanisms that stimulate fat storage. For years we have been told that this was just a problem of thermodynamics, meaning the more calories you eat, the more calories you store. The solution was, thereby, eat less calories or exercise more, or both. We are taught in school that a 1 gram of carbohydrate contains 4 kcal, 1 gram of protein contains 4 kcal, and 1 gram of fat contains 9 kcal.
If you ascribe to the dogma that weight gain or loss is due to thermodynamics, then it’s easy to see that cutting out fat (the largest calorie containing macro-nutrient) would be the best way limit calories. For the last 65 years, we as a society have been doing just that, cutting out fat, exercising more (with the idea of burning off more calories) and eating fewer calories.
What has this dogma done for us? It’s actually made us fatter! (1)
Obesity Rates Around the World
Some may argue that we really aren’t eating fewer calories and exercising more. But most people I have seen in my office have tried and tried and tried and failed and failed and failed to loose weight with this methodology. In fact, the majority of my patients attempt caloric restriction, exercise and dieting multiple times each year with no success. The definition of insanity is “doing the same thing over and over and expecting a different result.”
Most of my patients are not insane, they recognize this and stop exercising and stop restricting calories . . . ’cause they realized, like I have, that it just doesn’t work!
If you’re one that is still preaching caloric restriction and cutting out fat, I refer you to the figure above and the definition of insanity . . . your straight-jacket is in the mail.
So, if reducing the calories in our diet and exercising more is not the mechanism for turning on and off the storage of fat, then what is?
Before I can explain this, it is very important that you appreciate the difference between triglycerides and free fatty acids. These are the two forms of fat found in the human body, but they have dramatically different functions. They are tied to how fat is oxidized and stored, and how carbohydrates are regulated.
Fat stored in the adipose cells (fat cells) as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
(“What! Fat comes from sugar?! How can this be?!!“)
De Novo Lipogenesis
We all know that glucose derived from sugar is taken up by the cells from the blood stream and used for fuel, however, when too much glucose is in the blood stream or the blood sugar increases above the body’s comfort zone (60-100 ng/dl), the body stores the excess. The process is called de novo lipogenesis, occurring in the liver and in the fat cells themselves, fancy Latin words for “new fat.” It occurs with up to 30% (possibly more if you just came from Krispy Kream) of the of the carbohydrates that we eat with each meal. De novo lipogenesis speeds up as we increased the carbohydrate in our meal and slows down as we decrease the carbohydrate in our meal. We’ve known this for over 50 years, since it was published by Dr. Werthemier in the 1965 edition of the Handbook of Physiology (2).
While we know that fat from our diet and fat from our food is stored as triglyceride, it has to enter and exit the fat cell in the form of fatty acids. They are called “free fatty acids” when they aren’t stuck together in a triglyceride. In their unbound state, they can be burned as fuel for the body within the cells. I like to think of the free fatty acids as the body’s “diesel fuel” and of glucose as the body’s version of “unleaded fuel.” The free fatty acids can easily slip in and out of the fat cell, but within the adipose cell, they are locked up as triglycerides and are too big to pass through the cell membranes. Lipolysis is essentially unlocking the glycerol from the free fatty acids and allowing the free fatty acids to pass out of the fat cell. Triglycerides in the blood stream must also be broken down into fatty acids before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).
So when carbohydrates increase in the diet, the flow of fat into the fat cell increases, and when carbohydrates are limited in the diet, the flow of fat out of the fat cells increases.
Summarizing the control mechanism for fat entering the fat cell:
The Triglyceride/Fatty Acid cycle is controlled by the amount of glucose present in the fat cells (conversion to glycerol phosphate) and the amount of insulin in the blood stream regulating the flow of fatty acid into the fat cell
Glucose/Fatty Acid cycle or “Randle Cycle” regulates the blood sugar at a healthy level. If the blood glucose goes down, free fatty acids increase in the blood stream, insulin decreases, and glycogen is converted to glucose in the muscle and liver.
These two mechanisms ensure that there is always unleaded (glucose) or diesel fuel (free fatty acids) available for every one of the cells in the body. This provides the flexibility to use glucose in times of plenty, like summer time, and free fatty acids in times of famine or winter when external sources of glucose are unavailable.
The regulation of fat storage, then, is hormonal, not thermodynamic. Unfortunately, we’ve know this for over 65 years and ignored it.
We’ve ignored it for political reasons, but that’s for another blog post . . .
References:
1. James, W. J Intern Med, 2008, 263(4): 336-352
2. Wertheimer, E. “Introduction: A Perspective.” Handbook of Physiology. Renold & Cahill. 1965.
3. Taubs, G. “The Carbohydrate Hypothesis, II” Good Calorie, Bad Calorie. Random House, Inc. 2007, p 376-403.
I’ve been looking for the answer for quite some time. . . what role does caffeine play in your and my weight management journey? The answer gave me a headache. . . literally and figuratively.
As many of you, including my office staff, know, I love my Diet Dr. Pepper (and my bacon). I found that being able to sip on a little soda throughout the day significantly helped the carbohydrate cravings and munchies during a busy and stressful day at the office. Diet Dr. Pepper contains caffeine, however, I wasn’t really worried. Caffeine has been well know to have a thermogenic effect which increases your metabolism and has been thought for many years to help with weight loss among the weight loss community.
Diet Dr. Pepper is, also, one of only four diet sodas on the grocery store shelves that doesn’t contain acesulfame potassium (click here to see why most artificial sweeteners cause weight gain). The four diet sodas that I have been comfortable with my patients using are Diet Dr. Pepper, Diet Coke, Diet Mug Root-beer and Diet A&W Cream Soda. These are the last four hold out diet sodas that still use NutraSweet (aspartame) as the sweetener. Most of the soda companies have switched the sweetener in their diet sodas to the insulinogenic acesulfame potassium because it tastes more natural and aspartame has been given a media black eye of late. However, NutraSweet (aspartame) is the only sweetener that doesn’t spike your insulin or raise blood sugar (click here to find out why that is important).
Yes, I know. The ingestion of 600 times the approved amount of aspartame causes blindness in lab rats (but we’re not lab rats, and . . . have you ever met someone that drinks 600 Diet Dr. Peppers in a day? The lethal dose of bananas, which are high in potassium that will stop your heart, is 400). Aspartame can also exacerbate headaches in some (about 5% of people) and I’ve had a few patients with amplified fibromyalgia symptoms when they use aspartame. But for most of us, its a useful sweetener that doesn’t spike your insulin response, halting or causing weight gain.
But, over the last few years, I’ve noticed that increased amounts of Diet Dr. Pepper & Diet Coke seem to cause plateauing of weight and decreasing the ability to shift into ketosis, especially mine. I’ve also noticed (in my personal n=1 experimentation) that my ability to fast after using caffeine regularly seems to be less tolerable, causing headaches and fatigue 8-10 hours into the fast, symptoms that don’t seem to let up until eating. Through the process of elimination, caffeine seems to be the culprit.
After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the August 2004 Diabetes Care Journal screamed for my attention.
It appears that caffeine actually stimulates a glucose and insulin response through a secondary mechanism. The insulin surge and glucose response is dramatically amplified in patients who are insulin resistant. Caffeine doesn’t effect glucose or insulin if taken while fasting; however, when taken with a meal, glucose responses are 21% higher than normal, and insulin responses are 48% higher in the insulin resistant patient. Caffeine seems to only effect the postprandial (2 hours after a meal) glucose and insulin levels. The literature shows mixed responses in patients when caffeine is in coffee or tea, probably due to the effect of other organic compounds (1).
Caffeine effect on plasma glucose and plasma insulin compared to placebo (1).
Caffeine also diminishes insulin sensitivity and impairs glucose tolerance in normal and already insulin resistant and/or obese patients. This is seen most prominently in patients with diabetes mellitus type II (stage IV insulin resistance). Caffeine causes alterations in glucose homeostasis by decreasing glucose uptake into skeletal muscle, thereby causing elevations in blood glucose concentration and causing an insulin release (2-6).
Studies show that caffeine causes a five fold increase in epinephrine and a smaller, but significant, norepinephrine release. The diminished insulin sensitivity and exaggerated insulin response appears to be mediated by a catacholamine (epinephrine, norepinephrine & dopamine) induced stress response (5). Caffeine has a half life of about 6 hours, that means the caffeine in your system could cause a catacholamine response for up to 72 hours depending upon the amount of caffeine you ingest (7).
The reason for my, and other patient’s, headaches and fatigue after a short fast was due to the exaggerated stress hormone response. Increased levels of insulin were induced by a catacholamine cascade after caffeine ingestion with a meal, dramatically more amplified in a person like me with insulin resistance. The caffeine with the last meal cause hypoglycemia 5-7 hours into the fasting, leading to headaches and fatigue that are only alleviated by eating.
Even when not fasting, the caffeine induced catacholamine cascade causes up to 48% more insulin release with a meal, halting weight loss and in some cases, causing weight gain.
Caffeine is not the “Wonder-Boy” we thought it was.
How much caffeine will cause these symptoms? 50 mg or more per day can have these effects.
10,000 mg (10 grams) – lethal dose (Yes, 25 cups of Starbucks Coffee can kill you)
The equivalent of 100 mg of in a human was given to a spider, you can see the very interesting effect on productivity. How often does the productivity of the day feel like the image below?
Normal Spider (9)Spider on caffeine (9)
Beware that caffeine is now being added to a number of skin care products including wrinkle creams and makeup. Yes, caffeine is absorbed through the skin, so check the ingredients on your skin care products.
Diet Dr. Pepper, my caffeine delivery system of choice, has slightly less caffeine (39 mg per 12 oz can or 3.25 mg per oz) than regular Dr. Pepper. I found myself drinking 2-3 liters of Diet Dr. Pepper per day (long 16-18 hour work days in the office). After doing my research, I realized that my caffeine tolerance had built up to quite a significant level (230-350 grams per day).
So, a few weeks ago, I quit . . . cold turkey.
Did I mention the 15 withdrawal symptoms of caffeine? (8)
Headache – behind the eyes to the back of the head
Sleepiness – can’t keep your eyes open kind of sleepiness
Irritability – everyone around you thinks you’ve become a bear
Lethargy – feels like your wearing a 70 lb lead vest
Constipation – do I really need to explain this one?
Depression – you may actually feel like giving up on life
Muscle Pain, Stiffness, Cramping – feel like you were run over by a train
Lack of Concentration – don’t plan on studying, doing your taxes or performing brain surgery during this period
Flu Like Illness – sinus pressure and stuffiness that just won’t clear
Insomnia – you feel sleepy, but you can’t sleep
Nausea & Vomiting – You may loose your appetite
Anxiety – amplified panic attacks or feeling like the sky is falling
Brain Fog – can’t hold coherent thoughts or difficulty with common tasks
I experienced 13 of the 15 that lasted for 4 days. I do not recommend quitting cold turkey unless you have a week off and someone to hold your hand, cook your meals and dose your Tylenol or Motrin. My wife thought I was dying. . . I thought I was dying on day two. I actually had a nightmare about buying and getting into my own coffin. It can take up to three weeks to completely recover from caffeine withdrawal.
The other way to quit is to decrease your caffeine intake by 50 mg every two days. That means decrease caffeine by:
1 can of soda every two days
1/4 cup of coffee every day
1/2 can of Energy Drinks every two days
1 cup of tea every two days
The benefit of this method is that withdrawal symptoms are much less severe without the caffeine headache and the ability to remain productive. It will take longer, but quitting cold turkey is not a pretty picture. Been there . . . done that, . . . and I’m not going back. I actually lost another half inch off my waistline by day 5 of caffeine discontinuation.
What is the take home message here? If you have any degree of insulin resistance, caffeine makes it worse and will amplify your weight gain as well as decrease the productivity of your day.
“I’ve tried your low-carb diet, Dr. Nally, and it didn’t work.”
“Hmm . . . really?” If you’re mumbling this to yourself, or you’ve said it to me in my office, then lets have a little talk. You’ve probably been subjected to the common ketosis killers.
I’ve heard this statement before. It’s not a new statement, but it’s a statement that tells me we need to address a number of items. If you’ve failed a low carbohydrate diet, I’d suspect you are pretty severely insulin resistant or hyperinsulinemic. You probably never really reached true ketosis. I’d want to have you checked out by your doctor to rule out underlying disease like hypothyroidism, diabetes, other hormone imbalance, etc.
Nutritional Ketosis is Most Effective as a Lifestyle Change
Next, switching to a low-carbohydrate lifestyle is literally a “lifestyle change.” It requires that you understand a few basic ketosis principles. And, it takes the average person 3-6 months to really wrap their head around what this lifestyle means . . . and, some people, up to a year before they are really comfortable with how to eat and function in any situation.
I assume, if you are reading this article, that you’ve already read about ketosis and understand the science behind it. If not, please start your reading with my article The Principle Based Ketogenic Lifestyle – Part I and Ketogenic Principles – Part II. If this is the case, then please proceed forward, “full steam ahead!”
There are usually a few areas that are inadvertently inhibiting your body transformation, so let’s get a little personal.
Nutritional Ketosis is a Very Low Carbohydrate Diet
First, this is a low carbohydrate diet. For weight loss, I usually ask people to lower their carbohydrate intake to less than 2o grams per day. How do you do that? (A copy of my diet is accessible through my membership site HERE.) You’ve got to begin by restricting all carbohydrates to less than 20 grams per day. Any more than 20 to 30 grams per day will cause an insulin release from the pancreas and stimulate fat storage of both carbohydrate and fat for the next 10-12 hours, commonly killing ketosis. Keep a dietary journal to record your progress, your cravings, your successes and failures. I’m going to want to see it and review it with you if you see me.
No, I don’t believe in “Net Carbs.” Net Carbs are a sales gimmick to get you to buy “artificial food” that keeps you coming back for “artificial food” and halts your weight loss (you’ll see why shortly). You’re going to lose the most weight and feel your best when you eat real food. I do allow for the subtraction of real fiber, specifically non-cooked, non-blended, non-juiced leafy greens (If you cook, blend or juice a leafy green, it activates more carbohydrate availability). Leafy greens are real fiber. You can subtract them. In fact, I recommend eating 1-3 cups of leafy greens per day to help bowel function & provide necessary folic acid, but, everything else is “carbage.” Avoid it.
Yes, cottage cheese and yogurt contain carbohydrates. Be very cautious with them.
Alcohol also halts your weight loss. It’s not the sugar in the alcohol I’m worried about, the distilling process changes the sugar to alcohol, however, alcohol stimulates an insulin response after the alcohol is metabolized in the liver with a SIMILAR RESPONSE to regular sugar.
To Effectively Maintain Nutritional Ketosis, You MUST get adequate Protein
Second, this is a low carbohydrate, moderate protein, high fat lifestyle. N0 . . . it is NOT a high protein diet! However, so many of my patients don’t eat enough protein that they feel like it is a “high protein diet.”
Protein is essential for the building and maintaining of muscle, connective tissue and a number of other enzymatic reactions in your body. However, in patients who are morbidly obese [people with a body mass index (BMI) over 50], excess protein intake can cause fat to be stored by producing an excessive insulin response. In these patients we initially moderate protein. Excess sugars and a number of proteins, in the presence of a high insulin response, are converted to triglyceride (the soft squishy stuff inside the fat cells that make them plump) and stocked away inside your adipose tissue. Excessive protein, especially the amino acids argenine, leucine and tryptophan are common ketosis killers, not because they are converted to sugar, but because they stimulate and insulin response all by themselves.
If you don’t fall into the morbidly obese category (BMI over 50). Then, I encourage you to use the protein levels below.
Initially, I ask my patients to focus on lowering their carbohydrate intake and I don’t really worry about protein. (It is often hard enough to figure out what the difference between a carbohydrate and a protein in the first month or two if you’ve never had any nutrition background.) Most people begin losing weight just by lowering carbohydrates over the first few months. Once you figure out how to lower your carbohydrates, if your weight loss is not moving and your pants are not getting looser, then you’re probably eating too much protein.
How much protein do you need? It’s pretty easy to calculate and is based on your height and gender. Your basic protein needs to maintain muscle, skin and hair growth are as follows:
70 grams or higher for women per day
120 grams or higher for men per day.
However, these levels are WAY TOO LOW for weight loss and maintaining good health. Because we now know that protein acts as a hormone in a number of ways, in my office I recommend women get 80-90 grams of protein per day, and men should get > 150 grams of protein per day.
This also goes for protein powders and protein shakes. Many of these have 25-40 grams of protein in them per serving, so be careful with their use.
Nutritional Ketosis is a High Fat Diet
Third, this is a high fat lifestyle. Yes, I want you to INCREASE your fat intake. I’m going to repeat that, again, just for clarity, . . . . INCREASE your fat intake. Increase it to around 50% of your total calories, . . . 70% of your total calories if you can do it. Not enough fat is a common ketosis killer.
“What?! Won’t that cause heart disease and stroke and make my cholesterol worse?!!!”
I know, take a big deep breath . . . (you may even need to breath into a paper bag for a minute if you begin hyperventilating).
No, it will not raise your cholesterol, cause heart disease, or cause a stroke. If you have lowered your carbohydrate intake to less than 20 grams per day, then there is NO hormonal signal for you to make more bad cholesterol, worsen heart disease, or cause a stroke. In fact, there is great data showing that increasing your fat and lowering your carbohydrates reverses the blockage in the arteries. I see this reversal every single day in my clinic through the application of ketogenic diets.
If we remove carbohydrate as your primary fuel, you must replace it with something else.That something else should be fat. Protein must be moderated, as it will also be stored as fat if you eat too much. So, if the carbohydrates are kept low, fat intake can be increased and the body will pick the fat it wants and essentially throw the rest out without raising cholesterol, causing weight gain or causing heart disease. This is why we want you to use good natural animal fats like butter, hard cheese, olive oil, coconut oil, avocado, etc. Look for fats highest in omega-3 fatty acids as these decrease inflammation and improved weight loss. Look for meats highest in fat like red meat (55% fat) and pork (45% fat). Take the food pyramid and flip it over.
Check Your Sweeteners At the Door
The fourth common ketosis killer and culprit in halting your weight loss is artificial sweeteners. There are quite a few of them. Most of them WILL cause an insulin response (exactly what we don’t want for weight loss) with minimal to no rise in blood sugar. Raising blood sugar doesn’t matter, if the insulin is being stimulated . . . “you’re gonna gain weight for the next 10-12 hours.” I wrote an article for you to print off and hang on your fridge, upload it to your iPhone or carry it with you in your purse to the grocery store. (If you’re a man and you’re carrying a purse, please don’t tell me about it.) You can find the article here: The Skinny About Sweeteners. The short list of those sweeteners that are OK to use and cook with, and do not increase insulin response, can be found here in my Amazon Store.
Don’t Even Start with Coffee Creamers
Fifth on my list is coffee creamer. Coffee creamer contains corn syrup solids (another very special name for . . . SUGAR!!) and/or maltodextrin (SUGAR’s married name!). If you must put something in your coffee, then use real heavy cream (pure tasty fat) or real butter. It will taste much better (I’m told – I don’t drink coffee personally) and you won’t get an insulin spike 2-3 hours later and begin craving more coffee and donuts.
Yes, “Half & Half” is half fat and half sugar. . . avoid it too!!
Ketosis Killing Medications
The sixth culprit in halting weight loss is medications. Please talk to your doctor before making ANY changes in your medications as suddently stopping them can be hazardous to your health. Those highest on my list for stopping your weight loss are Glyburide (glipizide), insulin, & steroids like prednisone. A more complete list of medications that will halt your weight loss can be found on my on my ketogenic diet plan. If you are on any prescription medications, please talk to your doctor or to a physician board certified in obesity medicine treatment about how to adjust or wean these medications in a way that is safe and appropriate for your individual needs.
Estrogen
The seventh common culprit in halting weight loss is a lack of estrogen in menopausal or post-menopausal women. About 20% of women that I see in my practice who are over 55 years old, need some degree of estrogen replacement before they are able to lose weight. Estrogen plays a very large role in regulation of the metabolism and when deficient, causes weight retention or weight gain. Talk to your doctor about the risks and benefits of estrogen for you individually in this situation.
For many years, we’ve thought that caffeine was great for weight loss. However, we are finding, clinically, that too much caffeine can also cause a stress response by raising cortisol, releasing glycogen, thereby stimulating an insulin response and bringing your weight loss to a screeching halt. How much caffeine? . . . The jury is still out . . . and remains to be determined. But, I am currently under going an n=1 experiment on myself (as many of you know, I loved Diet Dr. Pepper. But I had to give it up). I’ll keep you posted . . .
Look closely at these eight issues. Correcting them usually solves most plateaus with weight loss and improves blood pressure, blood sugar and cholesterol control dramatically.
Adrenal Fatigue? Adrenal Insufficiency? Cortisol? PseudoCushing’s Syndrome? What do these terms mean and why are they all over the internet these days? And, what do they have to do with your weight loss?
This was our topic this evening on PeriScope. Katch Dr. Nally speak about this topic with rolling comments at Katch.me/docmuscles. Or you can watch the video below:
If you’re not sure about what this is, you’re not alone. I think I’ve heard the term “Adrenal Fatigue” at lease four times a day for the last three months. If you ask your doctor, they’ll probably scratch their heads too. The funny thing is that “Adrenal Fatigue” isn’t a real diagnosis, but it is all over the internet and it shows up in the titles of magazines in the grocery store every day. There’s even and “Adrenal Fatigue For Dummies” so it must be real, right?!
No. It isn’t a real diagnosis. It is a conglomeration of symptoms including fatigue, difficulty getting out of bed in the morning, and “brain fog” that have been lumped together to sell an “adrenal supplement.” (Sorry, but that’s really what it is all about.) Do a Google search and the first five or six sites describing adrenal fatigue claim the solution is taking their “special adrenal supplement.”
I know what you’re thinking, “Your just a main stream, Western Medicine doctor, Dr. Nally, you wouldn’t understand.” Actually, I do understand.
Adrenal fatigue has risen in popularity as a “lay diagnosis” because many patients show up at their doctors office with significant symptoms that actually interfere with their ability to function, and after all the testing comes back negative for any significant illness, they are told that they are normal. But the patient still has the symptoms and no answer or treatment has been offered. It’s discouraging. . . very discouraging.
That’s because the symptoms are actually the body’s response to chronic long term stress. Many of my patients, myself included, have found themselves “stuck” in their weight loss progression, feeling fatigued, struggling to face the day, with a number of symptoms including cold intolerance, memory decline, difficulty concentrating, depression, anxiety, dry skin, hair loss, and even infertility in some cases. Is it poor functioning adrenal glands? No, your feeling this way because the adrenal glands are actually doing their job!!
If the adrenal glands weren’t working you’d experience darkening of the skin, weight loss, gastric distress, significant weakness, anorexia, low blood pressure, and low blood sugar. The symptoms are actually called Addison’s disease and it is actually fairly rare (1 in 100,000 chance to be exact). So what is causing the symptoms you ask?
There are a number of reasons, but one that I am seeing more and more frequently is “Pseudo-Cushings’s Syndrome.” Pseudo-Cushing’s Syndrome is a physiologic hypercortisolism (over production of cortisol) that can be caused by five common issues:
Chronic Physical Stress
Severe Bacterial or Fungal Infections that Go Untreated
Malnutrition or Intense Chronic Exercise
Psychological Stress – including untreated or under-treated depression, anxiety, post-traumatic stress, or dysthymia (chronic melancholy)
Alcoholism
The psychiatric literature suggest that up to 80% of people with depressive disorders have increased cortisol secretion (1,2,3). People with significant stressors in their life have been show to have an increased corsiol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing a daily, cyclic over production of cortisol and then normalization of cortisol after resolution of the stressor. This cortisol response is not high enough to lead to a true Cushing’s Syndrome, but has the effect of the symptoms listed above and begins with limiting ones ability to loose weight.
I’m convinced that this is becoming more and more prevalent due to the high paced, high-stress, always on, plugged in, 24 hour information overload lives we live.
What is cortisol? It is a steroid hormone made naturally in the body by the adrenal cortex (outer portion of the adrenal gland). Cortisol is normally stimulated by a number of daily activities including fasting, awakening from sleep, exercise, and normal stresses upon the body. Cortisol release into the blood stream is highest in the morning, helping to wake us up, and tapers into the afternoon. Cortisol plays a very important role in helping our bodies to regulate the correct type (carbohydrate, fat, or protein) and amount of fuel to meet the bodies physiologic demands that are placed upon it at a given time (4,5,6).
Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids or proteins into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues (by stimulating insulin production) and turns on the maturation process of adipocytes (it makes your fat cells age – nothing like having old fat cells, right?!) In the process, cortisol suppresses the immune system through an inhibitory effect designed to decrease inflammation during times of stress (7,8,9). If this was only occurring once in a while, this cascade of hormones acts as an important process. However, when cortisol production is chronically turned up, it leads to abnormal deposition of fat (weight gain), increased risk of infection, impotence, abnormal blood sugars, brain fog, head
aches, hypertension, depression, anxiety, hair loss, dry skin and ankle edema, to name a few.
The chronic elevation in cortisol directly stimulates increased insulin formation by increasing the production of glucose in the body, and cortisol actually blunts or block-aids the thyroid function axis. Both of these actions halt the ability to loose weight, and drive weight gain.
Cortisol also increases appetite (10). That’s why many people get significant food cravings when they are under stress (“stress eaters”). Cortisol also indirectly affects the other neuro-hormones of the brain including CRH (corticotrophin releasing hormone), leptin, and neuropeptide Y (NPY). High levels of NPY and CRH and reduced levels of leptin have also been shown to stimulate appetite and cause weight gain (10-11).
How do you test for Pseudo-Cushing’s Syndrome?
Testing can be done by your doctor with a simple morning blood test for cortisol. If your cortisol is found to be elevated, it needs to be repeated with an additional 24 hour urine cortisol measurement to confirm the diagnosis. If Cushing’s Syndrome is suspected, some additional blood testing and diagnostic imaging will be necessary. Pseudo-Cushing syndrome will demonstrate a slightly elevated morning cortisol that doesn’t meet the criteria for true Cushing’s type syndrome or disease.
How do you treat it?
First, the stressor must be identified and removed. Are you getting enough sleep? Is there an underlying infection? Is there untreated anxiety or depression present? Are you over-exercising? These things must be addressed.
Second, underlying depression or anxiety can be treated with counseling, a variety of weight neutral anti-depressant medications or a combination of both. Many of my patients find that meditation, prayer, and journaling are tremendous helps to overcoming much of the anxiety and depression they experience.
Third, adequate sleep is essential. Remove the television, computer, cell phone, iPad or other electronic distraction from the bedroom. Go to bed at the same time and get up at the same time each day. Give yourself time each day away from being plugged in, logged in or on-line.
Fourth, mild intensity (40% of your maximal exertion level) exercise 2-3 days a week was found to lower cortisol; however, moderate intensity (60% of your maximal exertion level) to high intensity (80% of your maximal exertion level) exercise was found to raise it (12). A simple 20 minute walk, 2-3 times per week is very effective. Find a hobby that you enjoy and participate in it once or twice a week. Preferably, a hobby that requires some physical activity. The activity will actually help the sleep wake cycles to improve.
Fifth, follow a low carbohydrate or ketogenic diet. Ketogenic diets decrease insulin and reverse the effect of long term cortisol production. Ketogenic diets a have also been shown to decrease or mitigate inflammation by reducing hyperinsulinemia commonly present in these patients (13).
So, the take home message is . . . take your adrenal glands off of overdrive.
References:
Pfohl B, Sherman B, Schlechte J, Winokur G. Differences in plasma ACTH and cortisol between depressed patients and normal controls. Biol Psychiatry 1985; 20:1055.
Pfohl B, Sherman B, Schlechte J, Stone R. Pituitary-adrenal axis rhythm disturbances in psychiatric depression. Arch Gen Psychiatry 1985; 42:897.
Gold PW, Loriaux DL, Roy A, et al. Responses to corticotropin-releasing hormone in the hypercortisolism of depression and Cushing’s disease. Pathophysiologic and diagnostic implications. N Engl J Med 1986; 314:1329.
Ely, D.L. Organization of cardiovascular and neurohumoral responses to stress: implications for health and disease. Annals of the New York Academy of Sciences (Reprinted from Stress) 771:594-608, 1995.
McEwen, B.S. The brain as a target of endocrine hormones. In Neuroendocrinology. Krieger and Hughs, Eds.: 33-42. Sinauer Association, Inc., Massachusetts, 1980.
Vicennati, V., L. Ceroni, L. Gagliardi, et al. Response of the hypothalamic- pituitary-adrenocortical axis to high-protein/fat and high carbohydrate meals in women with different obesity phenotypes. The Journal of Clinical Endocrinology and Metabolism 87(8) 3984-3988, 2002.
Wallerius, S., R. Rosmond, T. Ljung, et al. Rise in morning saliva cortisol is associated with abdominal obesity in men: a preliminary report. Journal of Endocrinology Investigation 26: 616-619, 2003.
Epel, E.S., B. McEwen, T. Seeman, et al. Stress and body shape: stress-induced cortisol secretion is consistently greater among women with central fat.
Psychosomatic Medicine 62:623-632, 2000.
Tomlinson, J.W. & P.M. Stewart. The functional consequences of 11_- hydroxysteroid dehydrogenase expression in adipose tissue. Hormone and Metabolism Research 34: 746-751, 2002.
Epel, E., R. Lapidus, B. McEwen, et al. Stress may add bite to appetite in women: a laboratory study of stress-induced cortisol and eating behavior.Psychoneuroendocrinology 26: 37-49, 2001.
Cavagnini, F., M. Croci, P. Putignano, et al. Glucocorticoids and neuroendocrine function. International Journal of Obesity 24: S77-S79, 2000.
Hill EE, Zack E, Battaglini C, Viru M, Vuru A, Hackney AC. Exercise and circulating cortisol levels: the intensity threshold effect. J Endocrinol Invest. 2008. Jul;31(7):587-91.
Fishel MA et al., Hyperinsulinemia Provokes Synchronous Increases in Central Inflammation and β-Amyloid in Normal Adults. Arch Neurol. 2005;62(10):1539-1544. doi:10.1001/archneur.62.10.noc50112.
This evening we covered the 5 myths of weight loss identified through the National Weight Control Registry’s research findings. What causes “wrinkle face” for Dr. Nally? We also talked about & answered 20 minutes of rapid fire questions ranging from the amount of protein you need daily to the likelihood a human could be a bomb calorimeter . . . exciting stuff!!
You can watch the video stream below. Or you can Katch the replay with the rapid stream of exciting comments here at Katch.me/docmuscles.
What laboratory testing is necessary when you start your weight loss journey on a Ketogenic, Low-Carbohydrate, Paleolithic or any other dietary changes? Why do you need them and what are you looking for? We discuss these questions and others on today’s PeriScope. Lots of questions from around the world to day . . . this one lasted a bit longer than normal . . . 45 minutes to be specific. But it’s a good one because of all of your fantastic questions! You really don’t want to miss this one.
You can see the video below or watch the video combined with the rolling comments here on Katch.me/docmuscles.
A list of the labs that we discussed are listed below:
Fasting insulin with 100 gram 2 or 3 hour glucose tolerance test with insulin assay every hour
CMP
CBC
HbA1c
Leptin
Adiponectin
C-Peptid
NMR Liprofile or Cardio IQ test
Lipid Panel
Urinalysis
Microalbumin
Apo B
C-reactive protein
TSH
Thyroid panel
Thyroid antibodies
AM Cortisol
This list will at least get one started, provide the screening necessary to identify insulin resistance (Diabetes In-Situ), Impaired fasting glucose, diabetes and allow for screening for a number of the less common causes of obesity.
I would highly recommend that you get these through your physician’s office so that appropriate follow up can be completed. These labs will need to be interpreted by your physician, someone who understands and is familiar with various causes of obesity.
Join me as we chew the phat of ketogenic lifestyles PeriScope style and answer many questions like, “Why do I get ‘hangry’?” What causes hypoglycemia? How many times a day should I eat? and many more . . .
We talk briefly about why 60% of people with insulin resistance may need methylated folic acid to help with B vitamin absorption/use and where it can be found. (See me recent article about this called The Power of a Good Vitamin.)
You can see the whole PeriScope conversation on Katch.me/docmuscles with the comments scrolling or you can see the video stream below:
I recently read a blog post decrying anyone that would recommend a low carbohydrate / ketogenic diet to their patients.
What?!
In fact, this particular blog outlined a number of “adverse reactions” to a ketogenic diet, and based upon these perceived reactions, the writer advised severe caution with its use in just about anyone. It is important to note at the outset that most of the data this blogger quotes are from older studies completed in children for the treatment of epilepsy with specific liquid ketogenic dietary meal replacements. (Not what you’d expect in a low-carb / ketogenic diet for the average obese adult today.)
Diet Confusion
Thanks to recent misinformation by a number of medical professionals, including the person writing the blog referenced above, a poor understanding of fatty acid metabolism by the general community, and a distinct lack of understanding of human adaptability recorded over the last 5,000-6,000 years, there is still significant confusion about ketogenic diets.
It is important to recognize the crucial fact that the human body is designed to function quite well when supplied any of three macronutrients: carbohydrates, proteins or fats. It does so through an amazing series of enzymatic reactions referred to as the Krebs (tricarboxylic acid) cycle, producing needed ATP (adenosine triphosphate) required for our muscles to contract, our heart to beat and our diaphragm to expand our lungs. What’s even more amazing that that the body was designed to recognize the season we are in based up on the food we eat. That is, until we invented refrigerators in 1913. (Now our bodies think it’s year round summer time . . . wait . . . I live in Arizona where it is year round summer time.)
No, this is not a post about unplugging your refrigerator, living on solar, getting off the grid and saving energy.
Our bodies recognize the seasons we are in based upon inherent hormone release. The key hormone is insulin. Insulin can be looked at as the seasonal indicator to our bodies. Insulin production rises and falls based on our intake of carbohydrates (sugar, starches, some fibers). Insulin, essentially, tells our bodies when it is a “time of plenty” and when it was a “time of famine.” Why? You ask. We didn’t have refrigerators 100 years ago and you were lucky if you had a root cellar. The body needs to know when to store for the famine (the winter) that was around the corner. Insulin is that signal.
During the summer, potatoes, carrots, corn and other fruits are readily available. These are all starchy carbohydrates and they all require the body to stimulate an insulin response so that they can be absorbed. Insulin stimulates fat storage (J Clin Invest. 2000;106(4):473-481. doi:10.1172/JCI10842). Just like bears, our bodies were designed to store for the winter.
If you think back in history, your grandparents probably used stored meats & cheeses that could be salted or smoked for preserving during this time of year. Those crossing the plains were commonly found with pemmican, a concentration of fat and protein used as a portable nutrition source in the absence of other food. (Chapter VIII. Narrative of the Life of David Crockett, of The State of Tennessee, Written by Himself, Sixth Edition [E.L. Carey and A. Hart:Philadelphia] 1834, 1837; Marcy, The Prairie Traveler, p. 31.) Think about conversations you may have had with your grandmother when she told you that for Christmas, she received an orange. A single orange for a gift?! Many of my patients drink 12-15 of them in a glass every morning. The winter diets of our grandparents were very low in starches and carbohydrates. When carbohydrate intake is low, little insulin is produced.
Again, insulin is the hormone that tells you that you’re in “a time of plenty” and stimulates weight gain and cholesterol production to prepare for winter. Those prescribing the use of ketogenic diets understand this innate human adaptive trait, and use it to effect changes in weight, cholesterol and other desired metabolic changes.
Three types of ketones. Uptodate.com, May 2015
Now, let’s define the difference between ketosis and keto-acidosis and try to clarify the misinformation that is being spread around the blogosphere.
A ketone is a molecule the body produces from the breakdown of fat and some proteins (amino acids). There are specifically three types of ketones: beta-hydroxybutyric acid, acetoacetic acid and acetone. If ketosis was “bad,” then why would our bodies produce these molecules? They are not bad, and in fact, multiple studies show that the body is often more efficient and effective when it functions on ketones rather than glucose as its primary fuel source. The body can only supply a limited amount of sugar or glucose for fuel. If you talk to runners, marathoners or triathletes, they will tell you that after about 45-90 minutes of continuous endurance exercise the glucose supply runs out and they will experience what is termed a “bonk” (have a low-blood sugar or hypoglycemic episode). Unfortunately, our bodies can only store about 18-24 hours of glucose.
Metobolic Changes of Ketogenic Diet (American Journal of Physiology – Endocrinology and Metabolism Published 1 June 2007 Vol. 292 no. 6, E1724-E1739 DOI: 10.1152/ajpendo.00717.2006)
However, the body can store days upon days of fat in the form of triglyceride in the fat cells. Triglyceride is broken down into ketones. If glucose is the “unleaded” fuel, you can think of ketones as the “diesel fuel” that is easier to store and runs longer.
The average body functioning on ketones as the primary fuel will have a ketone level measured in the blood somewhere between 0.4 and 4 mmol/L. Because of a balance that is created by the use of ketones and a feedback mechanism that kicks in when the ketone level rises, the body will maintain a pH of around 7.4.
Ketoacidosis is dramatically different. If you are a type I diabetic, you don’t produce any insulin. The feedback mechanism regulating ketone use is broken and the ketone levels and triglyceride breakdown speeds up because the body can’t access glucose and can’t produce insulin. The ketone levels spike and the level can rise to > 25 mmol/L. In the presence of a high blood sugar and high ketone level, the acid level in the blood shifts to a pH of less than 7.3. This is referred to as metabolic acidosis and can be life threatening as the low pH shuts down the bodies’ enzymatic processes and a person becomes critically ill and without treatment, can die. (Kitabchi AE et al., Clinical features and diagnosis of diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults. www.uptodate.com, May 2015.)
If you’re not a type I diabetic, you have nothing to worry about. Regardless of what the “ketogenic nay-sayers” blog about, your liver makes approximately 240g of glucose per day, this stimulates a basal release of insulin which keeps the pH in check. It’s also what keeps weight loss at a consistent pace of around 2-10 lbs per month.
If you are a type I diabetic, don’t fret. Carbohydrate restriction can still be used very effectively. It just takes some balancing and understanding of your individual metabolism. Talk to your physician and/or medical bariatrician about how to follow a carbohydrate restricted diet while using insulin.
What about all the other “adverse effects” the blogosphere and other so-called experts claim about ketogenic diets?
Let’s take them on one by one. Are you ready?
Gastrointestinal (GI) disturbances – Yes. Any time you change your diet you may experience diarrhea, constipation or gassiness. Most of the time, this is because you are either 1) not eating enough leafy greens (fiber) or 2) you’re using a supplement that contains an artificial sweetener. Most of the studies on ketogenic diets did not incorporate fiber and the studies used to make this point were on children who used a ketogenic fat supplement shake or liquid preparations containing these artificial sweeteners to make them palatable. If you have spoken to any bariatrician, they will tell you, the best way to follow a ketogenic diet is to eat real food. If you want to read about the anecdotal GI effects of sweeteners, read the comment section in Amazon about the Haribo Sugar Free Gummy Bears.
Inflammation Risk – In every patient that I have placed on a ketogenic diet in the last 8 years, all inflammatory markers including CRP, Sedimentation Rate and Uric Acid have all decreased. Inflammation gets better on an appropriately formulated ketogenic diet. The older studies of ketogenic diets in children contain most of their fat from Omega-6 fatty acids from vegetable oil which will increase inflammation and oxidative stress, spike the cortisol levels and have the secondary effect of actually raising the triglycerides. (Simopoulos AP,The importance of the ratio of omega-6/omega-3 essential fatty acids, Biomed Pharmacother., 2002 Oct;56(8):365-79.)
Muscle Cramps/Weakness – The process of weight loss occurs by burning fat into CO2 and water. We breathe the CO2 out, but the water produced has to follow salts out through the kidneys. Hence, we lose salts. This can cause weakness and muscle cramps. The solution? Stop restricting salt on a low carbohydrate diet. We are the only mammal that restricts salt and we do it because low-fat diets cause us to retain water. Low carbohydrate diets do the opposite. Use sea salt or sip beef or chicken bouillon broth with your dinner. The use of yellow mustard also helps (the small amount of quinine in yellow mustard stops the cramping). If you have congestive heart failure, talk to your doctor about monitoring your salt intake in balance with your diuretic or water pill.
Hypoglycemia – If you read the ketogenic diet research, most of it was done on epileptic children. The diets called for a period of starvation, then the use of a ketogenic liquid based on the John’s Hopkin’s protocol. It is a well-known fact in medicine that starvation in children can frequently cause hypoglycemia, especially in children with other genetic or congenital defects leading to forms of epilepsy. In clinical practice, with ketogenic diet use in adults, hypoglycemia is rare.
Low Platelet Count (Thrombocytopenia) – Again, this was seen in the epileptic children who were placed into starvation first, then introduced a liquid fat replacement shake to stop intractable seizures. These liquids or shakes were often nutrient deficient in other essentials. Folic acid, B12 and copper deficiency can occur when not eating “real food.” Low platelet counts are rarely seen on ketogenic diets based around “real food.” Many children in the ketogenic studies had been on or were concomitantly on valproic acid for their seizures. Valproic acid is commonly known to cause thrombocytopenia (Barry-Kravis E et al, Bruising and the ketogenic diet: evidence for diet-induced changes in platelet function. Ann Neurol. 2001 Jan;49(1):98-103.; Kraut E, Easy Bruising, http://www.uptodate.com, May 2015.)
Easy Bruising – This is usually due to inadequate protein supplementation as was the case in much of the ketogenic literature where protein levels were also restricted. (Kraut E, Easy Bruising, http://www.uptodate.com, May 2015.)
Pancreatitis – Patients who are insulin resistant or have impaired fasting glucose commonly have high triglycerides. Elevation in triglycerides itself is a cause of pancreatitis. Ketogenic diets lower the triglycerides. However, if a patient has not been following their diet as directed, spikes in the triglycerides can occur placing the person at risk for pancreatitis.
Long QT Intervals/Heart Arrhythmias – The list of things causing Long QT intervals and abnormal heart rhythms is long and variable (Acquired Long QT Syndrome. Berul C et al. www.uptodate.com, May 2015). It is well know that starvation, rapid weight loss and liquid protein diets can cause a delay in the conduction signal in the heart. Anyone wishing to start any diet should have an electrocardiogram (EKG) through their doctor to ensure that the diet (of any type) doesn’t exacerbate a prolonged QT interval.
Three year weight loss and metabolic improvement in a patient on a Low-Carb / Ketogenic diet. Note: Patient admits to not following ketogenic diet during holidays from Nov 2013 – Feb 2014 (see the dramatic changes to the body when cheating happens)
Cardiomyopathy – Prolonged QT intervals have been associated with cardiomyopathy and the former can stimulate the later. Any diet that has the potential to prolong a QT interval has the potential to cause cardiomyopathy. Hence the need for regular EKG monitoring on any diet (Acquired Long QT Syndrome. Berul C et al. www.uptodate.com, May 2015).
Lipid/Cholesterol Changes – In the 8 years I have been applying ketogenic diets to patients, I have seen dramatic improvement in the triglycerides and HDL levels. The only time triglycerides rise over 100 is if the patient is using artificial sweeteners or is cheating on the carbohydrate restriction. Total cholesterol commonly rises, however, this is indicative of the fact that there is a shift in the LDL particle size and this affects the calculation of both total cholesterol and LDL-C. In light of this, most of my patients have dramatic improvement in triglycerides and small dense LDL particle number. I’ve included the common cholesterol changes I seen in my office as a few case reports to demonstrate the effectiveness of a ketogenic diet:
2 year ketogenic dietary labs and weight loss
Myocardial Infarction – It is interesting that one blogger includes this on the list of adverse reactions, however, when you actually read the study, the author of the paper make an “assumption” that there was potential for heart attack due to an elevated total cholesterol, however, a correlation was never made. Again, in the 8 years I have been using ketogenic diets, I have seen dramatic improvement in cholesterol profiles, inflammatory markers, atherosclerosis and carotid intimal studies (Shai I et al, Circulation 2010; 121:1200-1208).
Three year metabolic history of a Low-Carbohydrate / Ketogenic diet
Menstrual Irregularities / Amenorrhea – It is well known that any diet causing protein or other nutritional deficiency will affect the menstrual cycle first and growth second. The only time menstrual irregularities occur with a ketogenic or Low-Carb diet is when a patient is not taking in enough protein or is not eating real food. What amazes me is that a properly applied ketogenic diet causes normalization of the menstrual cycle, and in my practice, I’ve had a number of women successfully be able to conceive after making a ketogenic dietary change.
For more details on the nutrient content of a ketogenic diet, see the recent article by a friend of mine, Maria Emmerich. She’s been creating ketogenic diets for years and has a number of fantastic books my wife and I have been using in our home over the last nine years. She is one among many that can give you some direction on how to devise a healthy, real food based ketogenic diet. See the page on my website here that will give you some direction in formulating your Ketogenic Lifestyle.
Nally Family Low-Carb / Ketogenic Cheese Cake
So, to celebrate Mother’s Day, today, with my family, I am going to indulge in some Low-Carb / Ketogenic Cheese Cake!! Happy Mother’s Day, to all of you and especially to all you mothers out there making a healthy difference in the lives of your families! (You can find the recipe for this delicious cheese cake here)
In the words of Sir William Ostler, “If it were not for the great variability among individuals, medicine might well be a science and not an art.”
This post isn’t going to win me any friends . . . in fact, mentioning this topic a few days ago has already angered a number of them and resulted in an online tongue lashing by a few others. However, I can’t resist. And, based on some very persuasive data and personal experience, I don’t care.
Truth is truth . . . it doesn’t change no matter how you spin it, or attempt to fit it into your paradigm. The problem is what we have accepted in the last 40-50 years as “the scientific truth about getting healthy” is far from truth. By getting healthy, I’m implying the application of main-stream methods accepted to lose weight, reduce cholesterol, improve blood pressure and reduce your risk of heart disease and diabetes.
For the last 40 years we’ve been told that the only way to get and live healthy is to restrict our calories. This main-streamed advise continues even today in our USDA 2010 Dietary Guidelines. And, if you ascribe to this futile dogma propagated since the 1970’s, then you’ll know that the “only acceptable way” to do this is to “eat less fat” (because fat is the most caloric dense of the macro-nutrients, right?) and to “exercise more” (because that’s how we burn calories, right?!) Well, that’s what I thought, too. And that is the health prescription I doled out to my-self and to all of my patients for the first 8 years of my practice.
Interestingly, most of them, including myself, took that prescription of a caloric restricted diet of 1200-1500 calories per day and exercise 3-6 days a week for 30-60 minutes and ran with it. Personally, I restricted calories to 1200-1500 per day and began running triathlons. I performed cardiac monitored running, swimming and cycling for an hour a day during the week and 2 hours on the weekend. I lifted weights 2-3 days per week as well. Guess what it got me? Fat.
It raised my triglycerides by 100 points, elevated my LDL-C and increased my waistline by 3 inches. Yes, I gained weight. But, hey, my doctor was happy because my HDL-C went up by 4 points.
I saw this identical pattern with 3/4ths the patients in my office. A fourth of my patient’s (the group without any genetic insulin resistance) saw weight loss and improvement in their cholesterol profiles, but the rest didn’t. I had the exciting opportunity to introduce the saddened and discouraged 3/4ths of my patients to STATIN drugs and blood pressure medications. My average patient’s gained 2-3% of their body fat each year. Those that exercised like fiends were lucky if their weigh gain just stabilized.
What I saw in my office over a period of eight years was that exercise and caloric restriction didn’t work. But I couldn’t say that, because that goes against everything your 8th grade health teacher taught you. It contradicted your neighborhood dietitian, and it spat in the face of the food pyramid and the USDA Guidelines. The Government wrong? Never. . . . Speaking contradictory of the calorie-in/calorie-out exercise dogma was heresy, right? Contradict, Dr. Ornish, wouldn’t be heard of?!!
If I’ve learned one thing in my medical career, it is this: “Don’t be afraid to question everything” – even Dr. Dean Ornish, the USDA and the American Heart Association. And, fascinatingly, I’m not the only on that did.
——
——
Three Massive Studies did just that . . . question whether this exercise and caloric restriction dogma really works. This is what applying exercise and caloric cutting did for almost 67,000 people between 1972 and 2010 – little to nothing.
WHAT?!! Nothing?! You can’t be serous?
The first of these trials was the MRFIT (Multiple Risk Factor Intervention) Trial. It started in 1972, looking at 12,866 men with high risk for heart disease and followed them over seven years. All of them were placed on caloric restricted low fat diets and encouraged to exercise. It demonstrated that low fat diets and exercise FAILED to reduce weight or stop coronary artery disease in 100% of the cases. Don’t believe me? Read it for yourself (JAMA. 1982; 248 (12):1465-1477).
The second of these trials was the Women’s Health Initiative (WHI). This study started in 1991 and followed 48,835 women (yes, that’s a small city of women) for eight years. They didn’t believe the MRFIT results apparently, so they had a low fat (caloric restricted) arm and a control arm [the SAD diet (Standard American Diet)]. The women on the low fat arm lost a whooping 0.4 kg over the 8 year period (JAMA. 2006 Jan 4;295(1):39-49). 0.4 kg, really!?? That’s almost an entire pound of weight loss over 8 years. Quick, call Barnes & Noble so we can package that diet and sell it on Opra!! (Oh, wait, the news media was a little embarrassed by the findings and never really mentioned them.)
Lastly, if research on 60,000 men and women wasn’t enough to demonstrate what most primary care physicians seen in their offices daily, we had to do the Look AHEAD Study(Action for Health in Diabetes). This study started in 2001 and was supposed to run for 13.5 years. It studied 5,145 Type II diabetic patients with intensive lifestyle intervention. These patients were placed on intensive caloric and fat restriction of 1200-1800 calories per day with exercise and behavioral counseling. It was so unsuccessful, that they stopped the trial at 9.6 years – cause it wasn’t working.
The patients did lose some weight through Look AHEAD . . . an average of 6% of their body fat (That means you would have lost 15.6 lbs over 9 years if you weighed 260 lbs. Successful? . . . NOT). What made this trial worse is that it didn’t improve risk for coronary artery disease and people didn’t live longer (N Engl J Med 2013; 369:145-154). They just got the exciting chance to eat cardboard for 9 years of their lives. Sad. Very sad.
So, what does all this mean? Exercising your brains out at an expensive gym every morning won’t do much more than help you loose 1% of your body fat. It won’t increased your life span and it won’t decrease your risk of heart disease, despite what Dr. Ornish said. If you like spending $40 per month just to stare at sweaty fat bodies jumping up and down in spandex, by all means, please keep going to the gym. But I’d much rather spend that $40 on a nice rib eye steak at a restaurant staring at my wife. But, the benefits of saturated fat . . . that’s for another post.
Don’t get me wrong. I love lifting weights. I love riding my horse. I truly enjoy working in my yard. I even enjoy riding my bicycle. But I do these things now because they bring me peace, decrease my stress, and allow me to connect with nature. Believe me, there’s nothing natural about a 250 pound man in spandex staring at himself in a mirror repetitively lifting 30 pound bars of iron. But, we won’t go there.
My friends, and a few of my patients, get their knickers in a wad trying to decry the fact that I’m giving people a reason not to go running. Maybe I am. To be honest, there’s really only one reason I want to run, . . . and that’s when I’m being chased by a bear. But what good does it do to guilt a person into participation in an activity that isn’t really benefiting their health or help them lose weight, unless they really truly enjoy the activity for the sake of the activity?
Our health is not based upon a caloric scale of inputs and outputs. We are hormonal machines. We gain or lose weight and we gain or lose muscle based on powerful hormone signals, specifically insulin. Simple carbohydrate restriction has profound effects upon our weight, blood pressure, cholesterol and inflammatory states. Until we each come to grips with the fact that the food we eat triggers hormone responses in our bodies, we will continue down the path of diseases of civilization. Hippocrates summed it up when he said, “Let food be thy medicine, and let medicine be thy food.”
Have you noticed that there are a large number of advertisements in the media about checking your testosterone or “Low T” Syndrome? It seems like this is the new advertising trend on the radio and late night TV.
Suddenly, everyone’s testosterone is low and men are complaining about their libido, . . . or are they?
Benefits of Testosterone Optimization. (Image Credit: ArtOfManliness.com)
If you practice medicine long enough, you’ll see a trend that seems to have arisen as our waistlines have expanded. About half of the men in my office with insulin resistance, pre-diabetes or diabetes have low testosterone levels. But this shouldn’t be a surprise. Type II diabetes, metabolic syndrome and insulin resistance are all driven by an over production in insulin in response to a carbohydrate load in the meal. Patients with these conditions produce between two to ten times the normal insulin in response to a starchy meal. A number of studies both in animal and human models demonstrate that insulin has a direct correlation on testosterone suppression in the blood. This has been demonstrated in both men and women. In fact, glucose intake has been shown to suppress testosterone and LH in healthy men by suppressing the gonadal hormone axis and more predominant testosterone suppression is seen in patient with insulin resistance or metabolic syndrome.
In fact, to put it simply, insulin increases the conversion (aromitization) of testosterone to estrogen in men (it does the opposite in women). Interestingly, Leptin resistance has a similar effect. I tend to see the worst lowering of testosterone in men with both insulin and leptin resistance.
How to you improve your testosterone? Supplemental testosterone has been shown to help, but it comes with some risks, including prostate enlargement and stimulating growth of prostate cancer. The most natural way to improve your testosterone is to change your diet.
A low carbohydrate or ketogenic diet turns down the insulin production and allows the testosterone to be available for use by the body. A ketogenic diet has the effect of reducing leptin resistance as well through weight loss. A simple dietary change of this type is frequently seen in my office to increase testosterone by 100-150 points.
KetoOS – Drinkable Exogenous Ketones
What is a ketogenic diet? It is a diet that restricts carbohydrates to less than 50 grams per day, thereby causing the body to use ketones as the primary fuel source. So, for breakfast tomorrow morning, hold the oatmeal (1/2 cup of Quaker Instant Oatmeal is 31 grams of carbohydrates) and have the bacon and eggs. And, rather than have the cheesecake for desert this evening, have an extra slice of steak butter on your rib-eye and hold the potato.










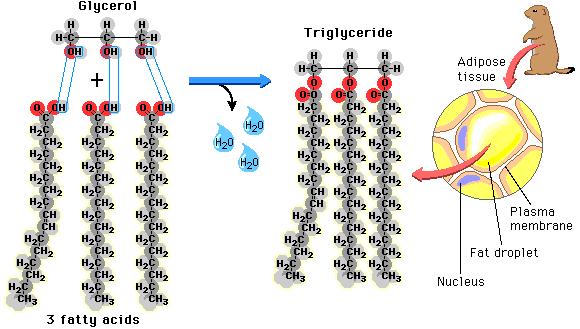 as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
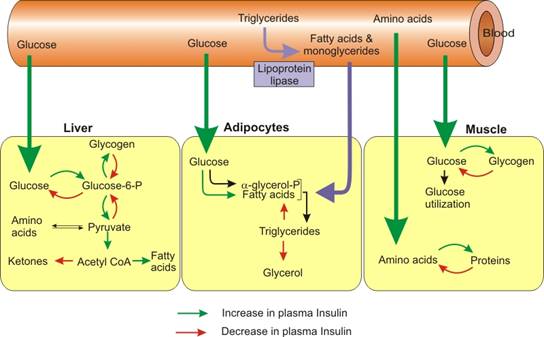 before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).
before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3). After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the
After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the 
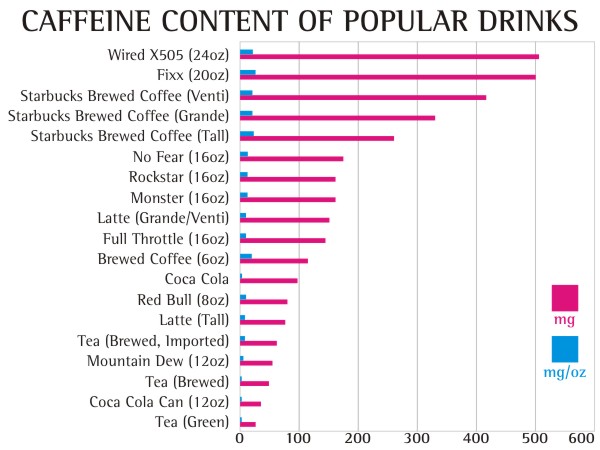





 That something else should be fat. Protein must be moderated, as it will also be stored as fat if you eat too much. So, if the carbohydrates are kept low, fat intake can be increased and the body will pick the fat it wants and essentially throw the rest out without raising cholesterol, causing weight gain or causing heart disease. This is why we want you to use good natural animal fats like butter, hard cheese, olive oil, coconut oil, avocado, etc. Look for fats highest in omega-3 fatty acids as these decrease inflammation and improved weight loss. Look for meats highest in fat like red meat (55% fat) and pork (45% fat). Take the food pyramid and flip it over.
That something else should be fat. Protein must be moderated, as it will also be stored as fat if you eat too much. So, if the carbohydrates are kept low, fat intake can be increased and the body will pick the fat it wants and essentially throw the rest out without raising cholesterol, causing weight gain or causing heart disease. This is why we want you to use good natural animal fats like butter, hard cheese, olive oil, coconut oil, avocado, etc. Look for fats highest in omega-3 fatty acids as these decrease inflammation and improved weight loss. Look for meats highest in fat like red meat (55% fat) and pork (45% fat). Take the food pyramid and flip it over.
 20% of women that I see in my practice who are over 55 years old, need some degree of estrogen replacement before they are able to lose weight. Estrogen plays a very large role in regulation of the metabolism and when deficient, causes weight retention or weight gain. Talk to your doctor about the risks and benefits of estrogen for you individually in this situation.
20% of women that I see in my practice who are over 55 years old, need some degree of estrogen replacement before they are able to lose weight. Estrogen plays a very large role in regulation of the metabolism and when deficient, causes weight retention or weight gain. Talk to your doctor about the risks and benefits of estrogen for you individually in this situation.
 People with significant stressors in their life have been show to have an increased corsiol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing a daily, cyclic over production of cortisol and then normalization of cortisol after resolution of the stressor. This cortisol response is not high enough to lead to a true
People with significant stressors in their life have been show to have an increased corsiol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing a daily, cyclic over production of cortisol and then normalization of cortisol after resolution of the stressor. This cortisol response is not high enough to lead to a true  Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids or proteins into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues (by stimulating insulin production) and turns on the maturation process of adipocytes (it makes your fat cells age – nothing like having old fat cells, right?!) In the process, cortisol suppresses the immune system through an inhibitory effect designed to decrease inflammation during times of stress (7,8,9). If this was only occurring once in a while, this cascade of hormones acts as an important process. However, when cortisol production is chronically turned up, it leads to abnormal deposition of fat (weight gain), increased risk of infection, impotence, abnormal blood sugars, brain fog, head
Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids or proteins into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues (by stimulating insulin production) and turns on the maturation process of adipocytes (it makes your fat cells age – nothing like having old fat cells, right?!) In the process, cortisol suppresses the immune system through an inhibitory effect designed to decrease inflammation during times of stress (7,8,9). If this was only occurring once in a while, this cascade of hormones acts as an important process. However, when cortisol production is chronically turned up, it leads to abnormal deposition of fat (weight gain), increased risk of infection, impotence, abnormal blood sugars, brain fog, head









 Fat.
Fat.




