
You don’t want to miss this event . . . Space is limited so RSVP TODAY!!

You don’t want to miss this event . . . Space is limited so RSVP TODAY!!


I am amazed after just two treatments.
100 percent of the muscle contracts with this amazing technology. Nothing else does that like EMSculptNEO.
I am personally amazed at how much better my motorcycle riding, fencing and sword-fighting has improved with just two core treatments. He is absolutely correct. It’s amazing what you can do when you strengthen your core.
4-6 treatments one week apart. HIFEM + RF gives you 20,000 crunches in 30 minutes while burning fat through a patented radiofrequency wavelength between contractions. I cannot tell you how amazed I am by this technology.
30% more muscle and 25% fat reduction – you can’t beat that.
When combined with a daily exercise program, and a ketogenic diet, you will see AMAZING results. Cut your carbohydrates back to less than 20 grams per day. For women, I recommend 90 grams of protein or more daily. For men, I recommend 150 grams of protein daily or more to see the best results.
Call the office and schedule your consultation with me today!!
Office Number: (623) 584-7805.
#LeadFolloworGetOutOrMyWay #JustKeepEsterifying #Ketogenic #Keto #KetogenicLifestyle #Carnivore #DrAdamNally #DocMuscles #DocMusclesLive #DocTalk #DocsWhoLift #LiftRunShoot #DocMusclesLife #PlantBasedDietsSuck YouTube.com/drnally/.
Dr Nallys Lasers: #PicoSure #Icon #SculpSure #TempSure #EMScuptNeo #EMSella #EMFace
I will be starting a twice weekly exclusive live-stream here for my amazing online followers and patient who are participating in the KetoClan Group on the following sixteen topics next week. Will be sharing the basics and my 22 years of clinical experience with each of these topics as it relates to health and weight management. These topics will take 10-30 minutes, then giving the remainder of the hour to you to ask questions.

The topics we will cover over the next 8 weeks are listed below:
1. Insulin
2. Monitoring Glucose – CGMs
3. Fat Adaptation
4. Things that make insulin go “bump in the night (or the day)” – (sweeteners, creamers, teas, Resveratrol, nuts, etc)
5. Protein
6. Basic Thyroid Function
7. Female Hormones
8. Male Hormones
9. Testing Ketones in Urine, Breath, Blood
10. Ketoacidosis
11. Medications and ketogenic diets (Metformin, DPP4s, GLP-1, SLT-2s, sulfonoureas, Berberine)
12. Stress – Cortisol & DHEA
13. Exercise – Cardiovascular and Resistance Exercise
14. Sleep
15. Food Cravings and the Subconscious Mind
16. Keto, Carnivore or Fasting – What should I be doing?
Not a member yet? Sign up here.

I’ve been told that many of you have nominated me. Thank you!!!
Every year Ketogenic.com hosts the Keto Awards with Metabolic Health Summit to highlight some of the best and brightest in our community.
There are five unique categories in which you can nominate and it would be an honor to me for you to add your vote:
Top Keto Educator
Top Keto Book
Top Keto Podcast
Top Keto Researcher
Making Positivity Louder
I’ll be sure to let you know who is selected.
Please take a minute to cast your vote for me.
Vote Here:

What is the cause of abdominal bloating when following a ketogenic or low-carbohydrate diet?

BHB stands for beta-hydroxybutyrate. This is one of three naturally occurring ketones formed in the body when metabolizing fat.

I’ve been asked what they are and how to use them quite a few times in the last week, so I thought I’d answer it here. . .
BHB can be used for a number of things:
1) to push you into a ketogenic state for 1-6 hours – I use them to jumpstart keto in people just starting a ketogenic diet (however, if BHB is being used while cheating on carbs at the same time, they often halt weight loss and in some cases can allow for weight gain).
2) I use it as a pre-workout drink for increased energy and stronger muscle contraction (I use them prior to sword fighting and it allows me more energy and endurance.)
3) For appetite suppression when the “munchies” try to kick in due to stress or anxiety.
4) To help enhance cognition in patients with Alzheimer’s dementia and Parkinson’s disease.
5) To improve mental clarity and focus in those with ADD/ADHD.
6) I also use them as a meal replacement while traveling.
7) I use them to help people who are morbidly obese experience a ketogenic state when they have never restricted carbohydrates before.
8) And, to prevent seizures when scuba diving with re-breather type equipment (bubble-less SCUBA).
You can find my exogenous ketones (BHB) at http://www.ketoliving.com

I’m not sure what it is about this time of year . . . maybe the post-holiday weight gain, or the fear of pulling out a swimming suit in a few months. But I have had a number of people, both men and women, in the office with excessive estrogen levels.
Estrogen excess and estrogen dominance are two hormone abnormalities I find commonly in both men and women in my practice. These two issues are frequently complicating factors that make feeling good and weight loss difficult. They are, also, often the main reasons people don’t see dramatic improvement in a person’s symptoms of energy, fatigue and mental clarity when they’ve already changed their diet and lifestyle.
IMPORTANT NOTE BEFORE WE GO ON: This information applies to patient who already have normal thyroid function and corrected insulin resistance. If your thyroid is off or if you are still significantly insulin resistant, it will affect estrogen and other male and female hormones, so follow a ketogenic diet and get your thyroid balanced FIRST!
I’ve addressed estrogen dominance in a previous blog post. You can find it here. Estrogen dominance is a condition where there is an abnormal estrogen/progesterone ratio. The estrogen/progesterone ratio MUST be balanced. Normal estrogen levels with low progesterone (this can commonly occur with the use of a synthetic progestin (HRT) in female patients) is a common scenario that falls into the estrogen dominance pattern.
Estrogen excess is a situation where progesterone levels may be normal but estrogen is elevated (an abnormal ratio can also be present in this condition).
The symptoms of excess estrogen can be:
Estrogen naturally stimulates cells to grow and multiply. Natural estrogens are essential. But, too much estrogen increases thyroid binding globulin, inactivating the thyroid function causing abdominal weight gain. Too much estrogen changes the body’s ability to remodel bone.
Estrogen is essential to stabilize the inner lining of arteries, however, excessive estrogen doubles one’s risk for stroke and increases the risk of coronary atherosclerosis and heart attack. Too much estrogen increases the size of the prostate, increases risk of prostate cancer and increases the risk of rheumatoid arthritis.
Estrogen excess is an elusive condition. Measuring estrogen levels is not frequently done, and most doctors were never trained to look at the three separate forms of estrogen in men and women. I had no idea this was an issue until about five years ago.
What causes excess estrogen?
The eleven most common causes of estrogen excess are:
Other diseases can cause estrogen ratio’s to be elevated. These include liver disease, zinc deficiency, excessive alcohol intake, obesity, calcium deficiency, insulin resistance, diabetes, and excessive testosterone therapy.
These hormones, like estrogens, progesterone and testosterone can be easily checked by your doctor through blood or salivary testing. The key is a balance in the ratio between progesterone and estrogens.
The two estrogens that are essential to test are:
These can be ordered through your doctor. Estrogens can take 2-3 months to balance out. It may take some time after making changes to see your levels normalize. Don’t fret.
When natural methods of lowering estrogen levels are ineffective, then your doctor will recommend treatment. A number of other effective medicinal approaches including:
In my clinical experience, a ketogenic lifestyle is foundational to balancing these hormones consistently and naturally. Carbohydrate restriction by itself corrects many of the diseases of civilization. I addressed this in my book The Keto Cure. For many, there are few more steps necessary to living a long, happy and healthy life.
In my office, in addition to the ketogenic or carnivorous diet, I add on Berberine Plus 500mg twice daily with meals. This has been shown to notably improve the insulin resistance, lower estrogen and improve progesterone naturally.
Years ago, this was hard to find, so I created my own supplement line and these can be found at Ketoliving.com. Go to Ketoliving. com and order your bottle of Berberine Plus right now, before it is too late. I designed my own pharmaceutical grade berberine so that my patients could make sure they are getting real berberine in the doses I want you to have.
The treatment of this issue isn’t difficult. There is much more to come on this subject. I will address each of the progesterone, testosterone, DHEA and sex hormone binding globulin abnormalities in my future blogs. So, keep an eye on my web page DocMuscles.com/blog/.
So, get your hormones checked by someone who understand this problem and knows how to treat it. Second, limit estrogen stimulating sources in your diet and environment. Third, control you diet and order a bottle of Berberine Plus right away.
What do you do when you hit a weight loss stall while living a ketogenic lifestyle? Find out below. Dr. Nally goes into detail on the multiple causes of stalling while following a low-carbohydrate or ketogenic lifestyle. He dispels the myths around counting calories and macros. And, he discussed the basics of overcoming a stall.
Help Dr. Nally have time to make more great videos: https://www.patreon.com/docmuscles

Over the last 18 years of my practice, I’ve seen tremendous success in helping people improve their health when low-carbohydrate dietary changes are anchored as the foundation of treatment. However, there is still a group of people that struggle with seeing success. Even with the most effective ketogenic dietary control, there are those that see abnormal weight gain, inability to lose weight, poor libido, fatigue, foggy thinking, mood swings, persisting depression, headaches, bloating, breast tenderness, fibro-cystic breast changes, hair loss, and hot flashes. They may not experience all these symptoms, however, many are often present. If you have been following a ketogenic lifestyle and are still experiencing any of these symptoms, you are probably suffering from estrogen dominance.
Estrogen dominance is a condition that elusively effects thousands of women (and men) and your doctor probably doesn’t even know about it. I didn’t know about it. I, like all of my physician colleagues, were trained in school that the symptoms above are related to fluctuations of estrogen as a woman ages (or dropping of testosterone as a man ages). We were, and still are, taught that they are fixed by giving more powerful doses of estrogen or testosterone.
Over the years of my clinical experience, giving more estrogen frequently didn’t work. And, giving men more testosterone didn’t work either. What I found very effective, for many, was changing the diet. And, for about 85% of people, the symptoms list above resolved. However, the cause of the symptoms above in that last 15% of patients I see was still elusive. Examinations, blood tests, and even psychological evaluations never revealed the answer. Giving synthetic estrogen, progestin or testosterone when the blood work showed abnormality partially alleviated some of the symptoms for a few months, but then the patients would end up back in my office with the symptoms having returned.
I’ve found a number of problems following the “standard” medical approach to using synthetic sex hormones.
The first problem is that estrogen, progesterone and testosterone are heavily bound to proteins in the blood. It is only the free component of the three forms of estrogen and progesterone in the body and the free testosterone that acts upon the delicate cells located throughout the body. Blood testing does not account for the levels of free estrogen forms and progesterone effectively. These can only be tested through salivary testing.
The second obstacle is that the synthetic forms of progesterone (progestin), cannot effectively enter the brain. When synthetic forms are used, a person only gets half the benefits of progesterone found in the human body. This is why so many women have depression, anxiety and foggy brain feelings when using the synthetic versions.
The third challenge is that pharmaceutical companies cannot patent a drug that is identical to your human hormones. The chemical structure of the synthetic estrogen, progestin or testosterone must be slightly different. Hormones effectively work on certain aspects of various cells throughout the body, however, progesterone and progestin (the synthetic version found in medroxyProgesterone) DO NOT have the same hormonal effect on each cell. Natural progesterone is broken down by the stomach when ingested. That’s why progestin was invented, however, it doesn’t act the same in the body and only does half the job.
The fourth dilema is that much of our food in the standard American Diet stimulates increased estrogen production or inhibits clearance of estrogen excess through the gut and digestive tract. This happens in men and women. We can get excess estrogen from animals treated with hormones in meats, milk and dairy products. Hydrogenated oils in processed foods change the way estrogen and progesterone are handled in the body. These unstable fats increase the effects of estrogen on the body and amplify the risk for cancers. Excessive omega-6 fatty acids in the diet magnify estrogen receptor response to estrogen.
Estrogen metabolism in the liver and removal in the gut are dependent on vitamins B & E, magnesium and idol-3-carbinol (IC3). Diets without adequate IC3 from glucobrassicin found in leafy green and crucirferous vegetables allow re-uptake of estrogen in the gut leading to high estrogen levels and estrogen dominance. This is where gut health is even more important, and where I see failure in the “carnivore” approach to a ketogenic lifestyle.
The fifth problem is that the more estrogen I give a person, the more estrogen receptors are unregulated to the surfaces of the cells in the body. When that happens, more estrogen is required. Excess estrogen can actually cause many of the same symptoms present in progesterone deficiency including:
More estrogen isn’t needed. Balancing natural progesterone with the current estrogen the body is already making is the solution in most cases. This can only be effectively assessed through a salivary hormone test.
In my clinical experience, a ketogenic lifestyle is foundational to balancing these hormones consistently and naturally. Carbohydrate restriction by itself corrects many of the diseases of civilization. I addressed this in my book The Keto Cure. For many, there are few more steps necessary to living a long, happy and healthy life.
The treatment to this issue isn’t difficult. For that reason, much more is to come on this subject. I will address each of the points above in future blogs. However, the first step is get your hormones checked by someone who understand this problem. And, then knows how to interpret it and treat it.

What is Insulin Resistance? Dr. Nally talks about the nuts and bolts of this syndrome and how it works. He answers multiple questions regarding diet and insulin resistance. Let me know what you thing and what questions future videos should answer.

Listen to KetoTalk Podcast #32 where we talk about hereditary angio-edema, adequate ketone ranges, statin use while in ketosis and healthy keto questions. You can listen in by going to KetoTalk.com or you can listen in on iTunes.

I am always fascinate when religious or spiritual topics collide with medical evidences and/or disease. I am convinced that “the natural man” has trouble recognizing that all things are spiritual unto God (1 Corinthians 2:14). Unfortunately, training in medicine often attempts to “educate the spirituality out of you.”
However, this week,and in church today, I’ve been reading about “signs of the times.” Of interest, and something that I’ve been pondering, is the statement made in Luke 21:25-26 where the Savior, Jesus Christ, specifically foretells the signs of His Second Coming. Among the perplexities and distress outlined, one statement stands out this week and has been the food of much thought, “Men’s hears failing them for fear,…” (Luke 21:26).

This food for thought is actually what directed me to this verse, as I’ve had a number of people express notable fear and worry over whether their diet is correct, because so much miss-information abounds in society today. Argument, stress and fear over diet, apparently, is not new and was something that even Paul noticed and wrote about in his Epistle to the Romans (Romans 14:1-3).
Stress and fear are two of the biggest hindrances to health and weight loss in my office. The most common non-food cause of failing to maintain ketosis while living a ketogenic lifestyle is stress. Stress is often due to fear. Men, and women alike, become fearful because they seem to:
When heartache arise from illness, injury, disability, death, divorce, wayward children and the other innumerable causes, stress and fear abound. Worry about diet and health, in a time when so much contradictory advise is at our fingertips, adds to that fear.
 When we forget our purpose and our identity, three symptoms arise both physically and spiritually:
When we forget our purpose and our identity, three symptoms arise both physically and spiritually:
The scriptures call this “weak hands & feeble knees” (Isaiah 35:3), and we in medicine refer to this as dysthymia, the first step in progression toward chronic depression and/or anxiety.
These symptoms all increase chronic levels of cortisol and  insulin. Amplified “brain fog,” weight gain, and inflammation are physical responses to the mental fear that is chronically unresolved. These symptoms just add to the apathy, mental slumber and fear of pain that was already present.
insulin. Amplified “brain fog,” weight gain, and inflammation are physical responses to the mental fear that is chronically unresolved. These symptoms just add to the apathy, mental slumber and fear of pain that was already present.
The problem is that over time, this progressive triad lead down the hormonal path to what we now call atherosclerosis, narrowing of the blood vessels, increasing the risk for heart attack, heart failure and stroke. This was seen in Hippocrates day as “sudden death related to episodes of chest distress” (Leibowitz, 1970). The Italian anatomist Giovanni Morgagni (1682-1771) described it in his day as “the force of the heart decreases so much more in proportion as the greater number of its parts becomes tendonous instead of being fleshy.”
SO, WHAT DOES ONE DO?
First, realize that the problems you are facing have been faced by millions of human beings and you are not alone. But, to paraphrase Irene Dunne, if you don’t stand for something, you will fall for anything.
I no longer believe in coincidence. Whether you have thought about it or not, every interaction you have with others (even our interaction . . . your reading this blog), are not by coincidence. There is a reason. Whether you believe it or not, everything around us testifies that God exists; the Hand of Providence can be seen from the rotation of the earth, planets and stars, the precision of the seasons, the balance of the atmosphere allowing for the perfect pressures and concentration of elements to sustain a life giving breath, to the perfect replication of DNA within billions of cells throughout the body.
I’m not trying to get religious, and, no, I can’t prove this through the scientific method . . . But, that is just the point. Hands are weak because of lack of faith. Faith is the substance of things hoped for, the evidences of which are not yet seen. Even though we do not see the evidences, we can discern the light and that gives hope. Hope is a substance that gives purpose. I can strengthen hands by sharing a little light and stabilize knees through friendship and fellowship (Romans 14:1).
If the Big Bang started the universe, what started the Big Bang? Where did the first atom or molecule or particle of dust come from? I have a very difficult time accepting that you and I are here by accident, by a chaotic explosion that created order. That implies that there must be a plan, and that plan had to have been set in motion by a Creator. You and I have a place in that plan. That also implies that that Creator placed solutions to our challenges, including the diseases of civilization, within our grasp and available to those seeking the solutions upon the earth today.
 Second, today’s society teaches the Pleasure Principle. This is the human instinct to seek pleasure and avoid pain, including avoiding painful recollections. We often define ourselves by those things that bring us pleasure. We each go through personal tests, failures and triumphs. Some of us harness all of those experiences for good, others find worsening mental paralysis due to fear of them. We often hide from the painful experiences and attempt to bury or forget them. Food is often involved with many of the experiences of life, and for a significant number of people, the endorphin release from eating a meal, sometimes just the act of chewing, may be the only pleasure one experience in a day, in a week or a in a year. Many people hide from painful recollections behind the simple pleasure produced by the eating of “comfort foods.” Food, and our opportunities to experience pleasure from it’s various flavors, textures and physical stimulus, begin to define us. However, hiding from life’s painful memories with momentary pleasures usually prolongs or makes the problem worse. The ingestion of simple foods containing glucose and fructose, their effect on the liver, and the hedonistic hormonal response is the basis of addiction, and simple carbohydrates provide the perfect fix.
Second, today’s society teaches the Pleasure Principle. This is the human instinct to seek pleasure and avoid pain, including avoiding painful recollections. We often define ourselves by those things that bring us pleasure. We each go through personal tests, failures and triumphs. Some of us harness all of those experiences for good, others find worsening mental paralysis due to fear of them. We often hide from the painful experiences and attempt to bury or forget them. Food is often involved with many of the experiences of life, and for a significant number of people, the endorphin release from eating a meal, sometimes just the act of chewing, may be the only pleasure one experience in a day, in a week or a in a year. Many people hide from painful recollections behind the simple pleasure produced by the eating of “comfort foods.” Food, and our opportunities to experience pleasure from it’s various flavors, textures and physical stimulus, begin to define us. However, hiding from life’s painful memories with momentary pleasures usually prolongs or makes the problem worse. The ingestion of simple foods containing glucose and fructose, their effect on the liver, and the hedonistic hormonal response is the basis of addiction, and simple carbohydrates provide the perfect fix.
Fascinatingly, when fructose is metabolized in the liver, in the presence of glucose (the basic structure of sugar – one fructose molecule bound to a glucose molecule), the byproduct has a hedonic (pleasure experiencing) effect on the exact same pleasure receptors in the brain that bind to morphine. Yes, that’s why the M&M’s make you forget your troubles and why the Jolly Rancher is so jolly. And, its the same reason you crave another do-nut two hours after you ate the entire baker’s dozen.
Healing can only occur when one is willing to confront and talk about the reasons, the real reasons you’d rather experience the endorphins from the do-nuts with your family instead of acknowledge your weakness, stresses, and fears. Many of us are so afraid of where we might be, we avoid acknowledging where and who we are. It takes courage not to take the easy path. And I will be the first to admit, pizza is the easy path and it’s scenic views are decorated with french fry palms and sunset clouds of apple fritters.
Third, many cultures and most forms of religion or spirituality incorporate the use of fasting to one degree or another. Why fasting? Well, it removes the effect of the pleasure principle for starters.
Fasting is also a simple and inexpensive method of shifting the body’s metabolism to one of ketosis. Spiritual, physical and mental clarity are more prominent in the ketotic state. Finding your identity and purpose are often encouraged while fasting. In fact, a whole chapter in the Old Testament’s Book of Isaiah is dedicated to the powerful effects of fasting and the ketogenic state it produces (Isaiah 58:3-12).
Your life is never without meaning. Keep it real by recognizing that diet alone may not compete your answer for physical health. Having courage and faith allow you to see and embrace the truth that is right in front of you. The Alcoholics Anonymous’ 12 step program only becomes successful when one realistically and courageously applies their faith to align with the truth they have felt all along. For any long-term lifestyle change to take place, one must connect and live the principles before one truly knows they are true. In this way the Ketogenic Lifestyle becomes real and men’s hearts are less likely to fail them. You can start here: The Principle Based KetoDynamic Lifestyle.

Listen in today as Jimmy and Adam blaze through a bunch of listener questions in Episode 27 of KetoTalk with Jimmy and the Doc!

KEY QUOTE: “Children are born in ketosis, so ketones are perfect for babies. The level of fat in breast-milk is essential for them to maintain their health and their growth.” — Dr. Adam Nally
Here’s are the 12 questions Jimmy and Adam answered in this special Keto Talk Mailbox Blitz extended podcast today:
– Testimonial from someone who learned his lesson why it’s important to stay ketogenic all the time
– Three-decade study confirms saturated fats are bad for health
– Is increased testosterone from a ketogenic diet a bad thing for women?
– Why am I still struggling with low energy and low ketones after months of being in ketosis?
– Can being in nutritional ketosis above 1.0 mmol cause painful headaches?
– Do artificial sweeteners and stevia raise insulin?
– Is my ketogenic diet causing me to cramp up before and during my half marathon racing?
– Is MCT oil a better fat to use on a ketogenic diet than other fats like coconut oil, cream, or butter?
– Why do I have a constant stomachache while I’m on a ketogenic diet?
– Do you have to be in ketosis to burn fat?
– Does being in ketosis lead to daily spotting and extended periods?
– Are ketones in my baby’s breastmilk safe for her to consume? And why did my milk supply drop when I went keto?
– What is the impact of the supplement creatine on ketones, blood sugar, and insulin levels?
– Can I ease into ketosis as a way to avoid the dreaded “keto flu?”
KEY QUOTE: “If you’re not feeling energy after that adaptation period of 2-4 weeks at the very most, then you’re doing something wrong. Let that be your wakeup call to change something.” — Jimmy Moore

Listen in here at KetoTalk.com or you can download the episode for free on iTunes.
Hypertension (elevated blood pressure) is one of the triad symptoms of metabolic syndrome. Most of the hypertension that I see clinically is driven by insulin resistance as  the underlying cause. I see this problem in a very large majority of the people in my office and I am seeing people younger and younger show up with continually increasing blood pressure.
the underlying cause. I see this problem in a very large majority of the people in my office and I am seeing people younger and younger show up with continually increasing blood pressure.
In medical school, we were taught to treat “borderline” or “slightly elevated blood pressure,” through “lifestyle changes” which was another way of saying exercise, caloric restriction & hold the salt. But most physicians today will tell you that exercise, salt & caloric restriction doesn’t work. When asked why the 34 year old male in my office suddenly has elevated blood pressure, the only explanation we had was it is a “genetic problem,” or “blood pressure naturally goes up as we get older,” or “you’ve been eating too much salt,” and they are started on blood pressure medication and sent on their way. But, as time went on, I found that I had to keep adding more and more blood pressure medication to control the continually rising blood pressure of the patients in my practice.
Most of these people will have a progressive elevation in blood pressure over time, and these blood pressure (anti-hypertensive) medications are/were continually raised until the person is on four or five different blood pressure pills at maximal doses. Again, when questioned why, their genetics are blamed and that is the end of it. Or is it?!
What shocked me was that when I took patients off of salt & caloric restriction, and placed them on low carbohydrate high fat diets (and yes, I gave them back their salt), their blood pressure normalized. I noticed that as their fasting insulin levels began to fall, their blood pressure began to return to normal.
What?! Blood pressure rise is caused by insulin?!
Ummm . . . Yes!
I am a prime example. During the first few years of my medical practice and reserve military service, we had routine vitals checkups. I was working out 3-5 days a week with weights and running 3-5 miles 2-3 times a week and restricting my calories to 1500 per day. So, I thought I was in pretty good shape. However, it was not uncommon for for the nurse to raise her eyebrows at my blood pressure readings in the 140-160 systolic and 85-98 range diastolic. “Oh, it’s the lack of sleep last night,” or “it’s the caffeine I had this morning,” would be my excuse. But I was making a lot of excuses, and in light of those excuses, my caloric restriction, exercise and salt restriction, I was also still gaining weight.
By the 5th year of my medical practice, I weighed 60 lbs heavier than I do today and I struggled to keep my blood pressure under 150/95. I was violating my own counsel . . . don’t trust a fat doctor for nutritional advise. (Or, was that advise from Dr.House?)

After cutting out the carbohydrates (I’ve kept my carbohydrate intake < 20 grams per day), moderating my protein intake and eating all the fat I am hungry for each day, my recent physical examination at the beginning of June 2016 revealed my blood pressure at 112/64. I don’t remember ever having blood pressure that low. And to be honest, I didn’t sleep well the night before my exam due to a number of middle of the night patient calls.
When I first started treating the insulin resistance problem in the human, rather than the blood pressure problem, I began to see immediate reductions in blood pressure within one to two weeks. So much of a reduction that if I didn’t warn the patient that they should  begin to back down their blood pressure medications, they would experience symptoms of dizziness, light-headedness, headache and a few patient’s nearly passing out. On a low-carbohydrate, high-fat (ketogenic) diet you need salt (sodium, potassium, & magnesium).
begin to back down their blood pressure medications, they would experience symptoms of dizziness, light-headedness, headache and a few patient’s nearly passing out. On a low-carbohydrate, high-fat (ketogenic) diet you need salt (sodium, potassium, & magnesium).
The process of burning fat as fuel causes you to lose increased amounts of sodium & potassium, and you have to replace these electrolytes. A number of my patients begin a low-carbohydrate, high-fat diet and are afraid of increasing their salt intake. Not replacing these electrolytes while on a ketogenic diet can also lead to low blood pressure, dehydrate and dizziness.
I often wondered why applying a ketogenic diet had such a profound effect on blood pressure so quickly. Dr. Robert Lustig helped answer that question for me.
In order to understand how the Standard American Diet (we call it the SAD diet in my office) raises your blood pressure, it is important to understand how the body processes the basic sugar molecule. Sugar is one glucose molecule bound to a fructose molecule. This is broken down in the body and 20% of the glucose is metabolized in the liver, the other 80% is sent on to be used as fuel throughout the body. Fructose, however, is where the problems arise. 100% of the fructose is metabolized in the liver, and the by product of fructose metabolism is increasing the liver’s production of MORE glucose and the byproduct of uric acid. Uric acid is produced and this inhibits the production of nitric oxide. The diminished nitric oxide in the presence of an increased level of glucose (stimulating increased insulin production due to eating starches) constricts the blood vessels and raises blood pressure. Yes, that donut you just ate raised your blood pressure for the next 12 hours.
The mechanism that fructose containing carbohydrates, sugars and starches raise blood pressure, cholesterol and cause weight gain can be seen in the really complex diagram found in Dr. Lustig’s 2010 article:

So, how do you lower your blood pressure through diet?
First, cut out all the simple sugars. These include anything with table sugar, high fructose corn syrup and corn syrup. (This is why people with any change in diet see some improvement in weight and blood pressure as they remove the simple sugars like candy, sugared drinks and pastries from their diet.)
Second, limit your overall intake of other sources of carbohydrates including any type of bread, rice, pasta, tortilla, potato, corn and carrots. Realize that carbohydrate in fruit is fructose, and when taken with other forms of glucose can have the same effect as table sugar – it can and will raise your blood pressure, as well as halt or cause weight gain.
Third, if you are taking blood pressure medications for hypertension, see your doctor about close monitoring of your blood pressure as it can and will drop within 2-4 weeks of making these dietary changes.
Maintaining ketosis is really important for weight loss and blood pressure or hypertension control. I am very much an advocate of using real food for this process, but I have also found that the use of exogenous ketone salts aid significantly in maintaining ketosis. I have found that exogenous ketones are the next step in bridging the difficulty of day to day maintenance of ketosis.
It isn’t making the mistakes that’s critical; it’s correcting them and getting on with the task that’s important. If you’ve been calorie restricting and exercising to lower you blood pressure, don’t fret. A simple change in your diet focused on restricting starches and carbohydrates has been demonstrated in my office to be more powerful than many of the blood pressure medications we’ve used for years.
Learn how to get started on a low carbohydrate, high fat (ketogenic) diet here. You can also read about the basic principles in my recent articles The Principle Based Ketogenic Lifestyle – Part I and Ketogenic Principles – Part II.

Listen to Dr. Nally & Jimmy Moore as they answer the following questions in KetoTalk Podcast #21.
Get the answers to these questions and much more when you listen to KetoTalk.com or download the podcast for free on iTunes.


We have been taught for over 50 years that the minimum carbohydrate intake necessary to maintain health is 130 grams per day, with the average diet of 2000 calories per day containing around 300 grams per day based on 1977 recommendations that 55-60% of are dietary intake should come from carbohydrates. This value was initially established during World War II by a committee of scientists tasked with determining dietary changes that might effect national defense (1). These “guidelines,” originally called the Recommended Daily Allowances (RDA) and accepted by many as the gospel truth, have been modified every ten years and in 1997 changed to the Dietary Reference Intake (DRI). However, the recommended carbohydrate values have not changed other than “avoiding added sugars” in the most recent 2015 recommendations.
In light of the fact that there are NO actual diseases caused by lack of carbohydrate intake, most dietitians and physicians still preach the carbohydrate dogma originally outlined by the RDA. I say dogma, because these recommendations are based on a diet that vilifies fat, particularly animal fat like red meat. Say the words “red meat” around a dietician these days you’d think Voldemort (“He Who Shall Not Be Named”) had returned.
I bring up the carbohydrate quandary because it is a question that I am asked every single day. The question that seems to be asked of me, more and more, is what exactly is a carbohydrate?
Let’s make it simple. There are really only three types of carbohydrates:
Let’s start with Sugar. The simple form of carbohydrates, and the form that spikes your blood sugar and insulin rapidly, are called mono-saccharides (glucose, galactose, fructose & xylose). When two of these mono-saccharides are bound together they form disaccharides like sucrose, also known as “table sugar” (glucose + fructose), lactose found in milk (glucose + galactose), and maltose found in cereals and sweet potatoes (glucose + glucose).

The simple monosaccharides or disaccharides are easy broken into their mono-saccharide form in the blood stream and require the body to produce insulin to be used. The person with insulin resistance, impaired fasting glucose or type II diabetes often produces 2-10 times the normal amount of insulin to correctly use these mono-saccharides (see why this is a problem in: The Dreaded Seven: Seven Detrimental Things Caused By High Insulin Levels). Remember, fruit is also simple sugar containing the mono-saccharide fructose . . . which we call “natures candy” in my office.

“Yea, I know sugar is bad for me, but Dr. Nally, I just eat the good starches.”
If I had a nickel for every time I’ve herd that phrase . . .
We’ve become comfortable with shunning fat and “simple sugar,” but in the process we’ve been eating more “good starch.” But the “good starches” are also saccharides – just in longer chains of more than three glucose molecules bound together. Our gut easily breaks the bonds between the glucose links and turns these starches into mono-saccharides to be used as fuel. It takes a bit longer than the simple sugars above, so the release of insulin is slower (which is why it has a better glycemic index score), but whether you produce the insulin in the first hour or the second hour after eating it, insulin is still insulin. In the case of insulin resistance, the damage is still done.
These good starches make up “comfort food” like bread, rice, pasta, potatoes, corn, grains & oats. To the patient with insulin resistance, impaired fasting glucose or type II diabetes, the higher insulin response stimulates increased weight gain, rise in cholesterol, shift in hormone function and progression of atherosclerosis (vascular and heart disease). See the recent article on Why Your Oatmeal is Killing Your Libedo.
What about “resistance starches?” These are still starches and I am finding clinically that they still cause a rise in insulin and push people out of ketosis (See Common Ketosis Killers).
Finally, Fiber. Fiber is a carbohydrate, however, it is the indigestible part of the plant. Fiber has double bonds between the saccharides that human gastrointestinal tracts cannot digest. In most cases, fiber passes right through the intestines without being digested. It actually acts like a broom for your colon, helping the intestines to move nutrients through the system. This is why I recommend 1-2 leafy green salads a day for most patient’s following ketogenic diet. Fiber does help to promote bowel function.

Fruit, non-green vegetables, pasta, grains and breads do contain good sources of fiber, however, these foods also have absorbable starches making them problematic as noted above.
The take home message is this, the use of starch or simple carbohydrate will be problematic for weight loss, cholesterol control, blood sugar control or blood pressure control in a patient with insulin resistance.
Therefore, the ketogenic lifestyle truly begins at the end of your comfort zone.

A few of my patients have recently asked me, “Dr. Nally, why to you post pictures of your horse, koi and farm animals on instagram?”
Let me answer that question with the following questions:
If you can answer “yes” to any of the questions above, then I highly recommend prescription strength nature . . .
All parody and humor aside, full strength prescription nature is one of the very best treatments for stress.
I find that sitting outside with my animals, watching the birds, dogs, horses and ducks dramatically helps with lowering my stress levels and helps me re-focus. You can see my favorite place to sit on my farm and watch nature . . . here on Katch.me
You may find the following posts very insightful in explaining how stress wreaks havoc on your weight loss, mood & emotions and how to go about fixing it:
For someone like me, who spends 14-18 hours a day taking care of illness and sickness, I have found that spending time in nature is often more therapeutic than any pill available in the pharmacy. So, this afternoon, if your looking for me, I’ll be taking my own medicine, a prescription of Nature Rx on my horse.
Today in the office I had the calorie conversation again . . . three times. We have an entire society with a very influential health and fitness industry built around the almighty calorie. Has it helped? Looking at our 5 year obesity outcomes. It hasn’t helped a bit. In fact, it is worse. In 1985 only 19% of U.S. adults were obese.
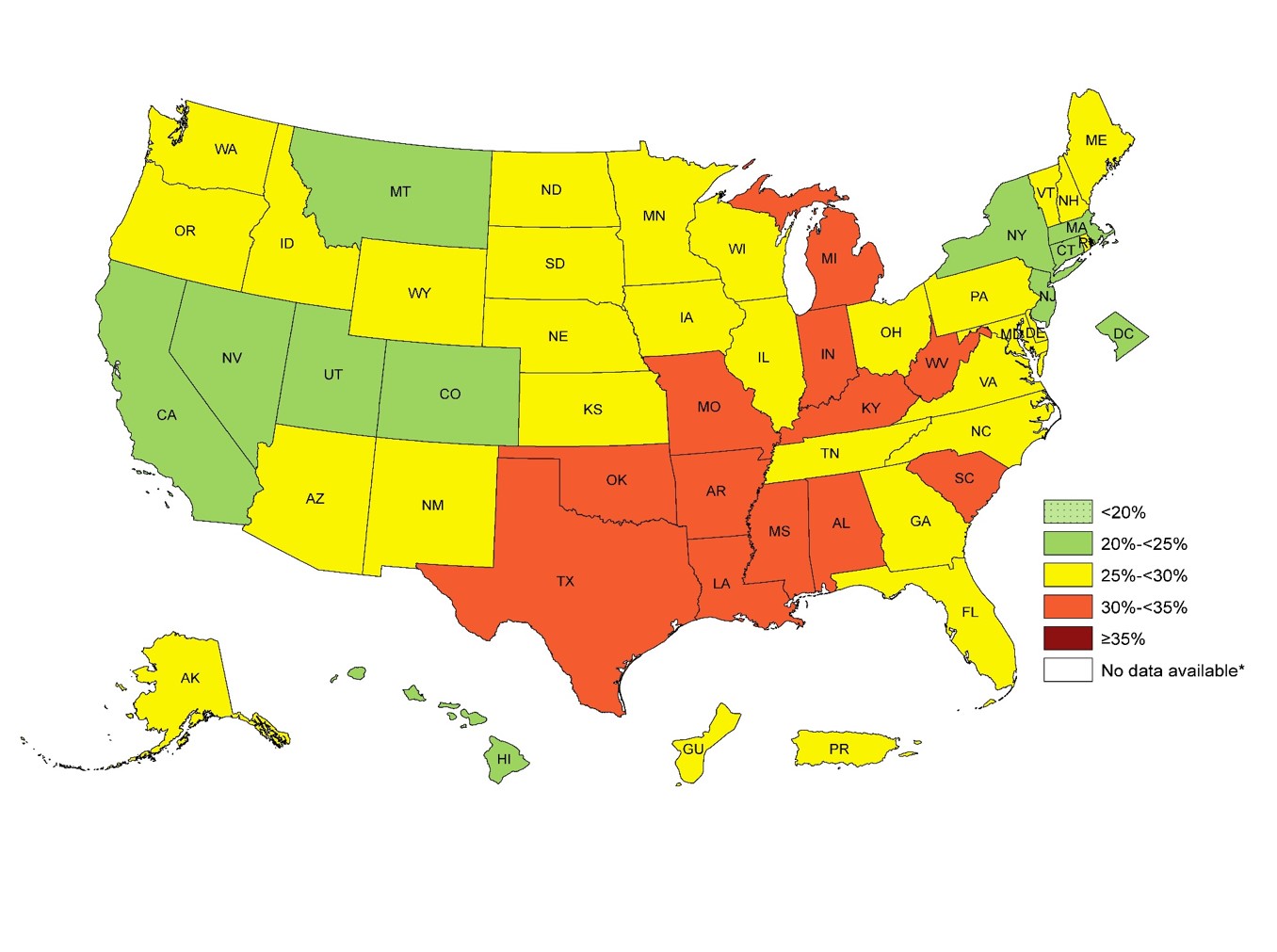
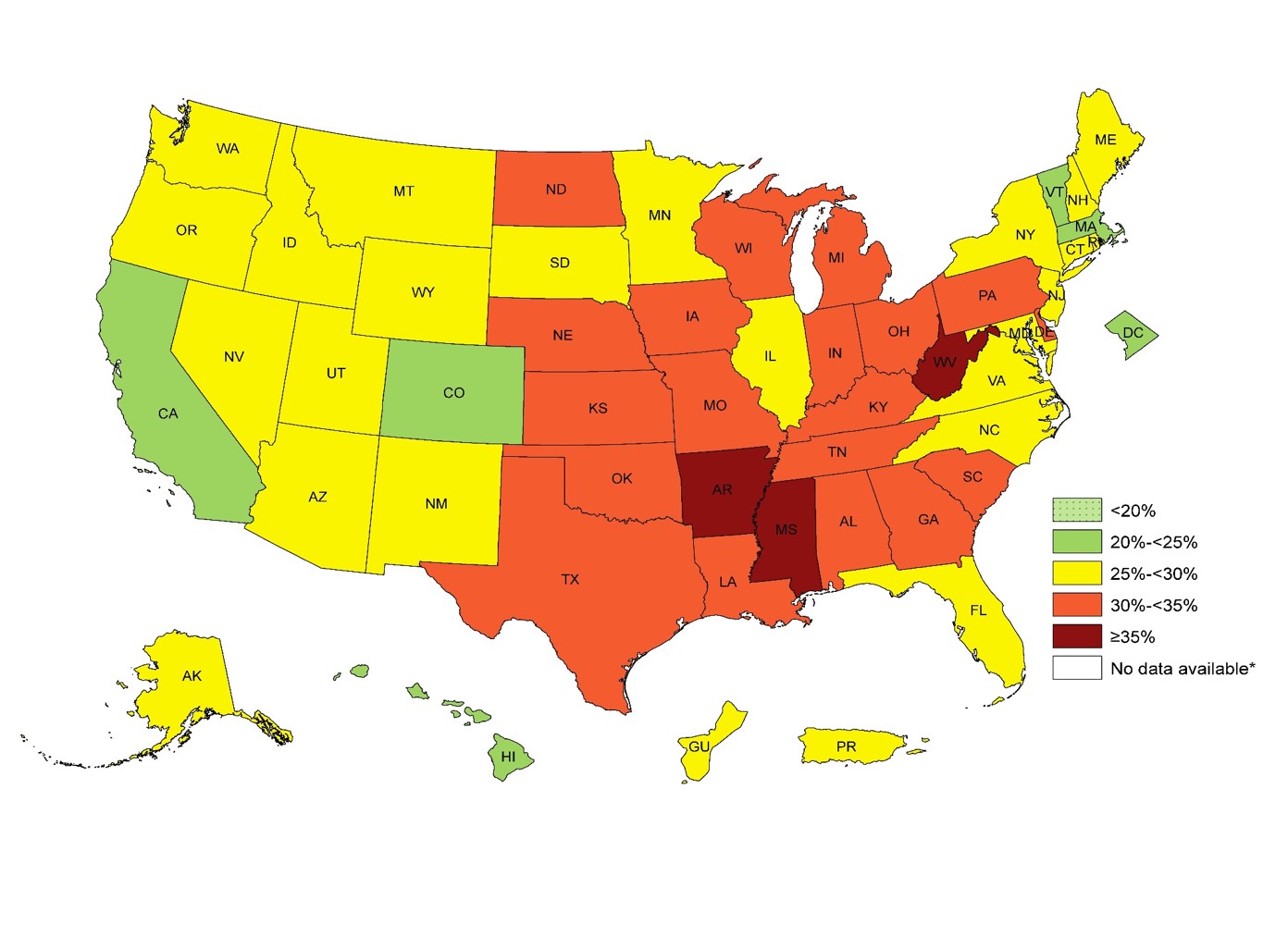
In 2014, 34.5% of U.S. adults were obese. The numbers this year are approaching 35.6% You can see the dramatic increase in obesity by 1-3% every year for the last 5 years in the CDC images above.
For over 50 years we have been told that caloric restriction and fat restriction is the solution. But by the numbers above, the 58 million people in the U.S. utilize a gym or health club to burn off those calories aren’t seeing the success that they should be expecting.
Why? Because the calorie is NOT king. What do I mean by that? We don’t gain weight because of the thermogenic dogma we’ve been taught for the last 50 years. Our weight gain is driven by a hormone response to food. Hear more about why the calorie is NOT king on tonight’s PeriScope. You can Katch it here with all the live stream comments and hearts at Katch.me/docmuscles.
Or you can watch the video without the comments here:
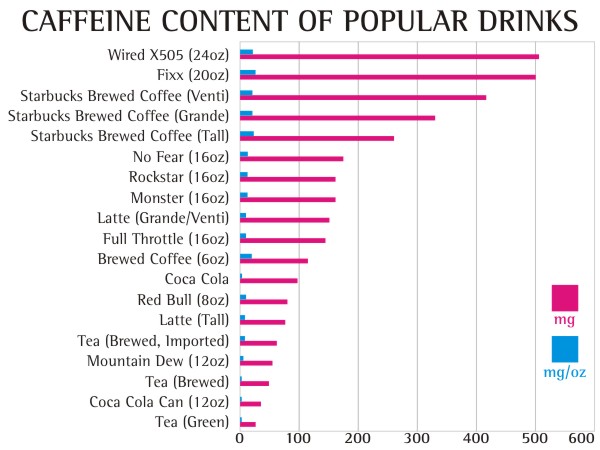
I’ve been looking for the answer for quite some time. . . what role does caffeine play in your and my weight management journey? The answer gave me a headache. . . literally and figuratively.
As many of you, including my office staff, know, I love my Diet Dr. Pepper (and my bacon). I found that being able to sip on a little soda throughout the day significantly helped the carbohydrate cravings and munchies during a busy and stressful day at the office. Diet Dr. Pepper contains caffeine, however, I wasn’t really worried. Caffeine has been well know to have a thermogenic effect which increases your metabolism and has been thought for many years to help with weight loss among the weight loss community.
Diet Dr. Pepper is, also, one of only four diet sodas on the grocery store shelves that doesn’t contain acesulfame potassium (click here to see why most artificial sweeteners cause weight gain). The four diet sodas that I have been comfortable with my patients using are Diet Dr. Pepper, Diet Coke, Diet Mug Root-beer and Diet A&W Cream Soda. These are the last four hold out diet sodas that still use NutraSweet (aspartame) as the sweetener. Most of the soda companies have switched the sweetener in their diet sodas to the insulinogenic acesulfame potassium because it tastes more natural and aspartame has been given a media black eye of late. However, NutraSweet (aspartame) is the only sweetener that doesn’t spike your insulin or raise blood sugar (click here to find out why that is important).
Yes, I know. The ingestion of 600 times the approved amount of aspartame causes blindness in lab rats (but we’re not lab rats, and . . . have you ever met someone that drinks 600 Diet Dr. Peppers in a day? The lethal dose of bananas, which are high in potassium that will stop your heart, is 400). Aspartame can also exacerbate headaches in some (about 5% of people) and I’ve had a few patients with amplified fibromyalgia symptoms when they use aspartame. But for most of us, its a useful sweetener that doesn’t spike your insulin response, halting or causing weight gain.
But, over the last few years, I’ve noticed that increased amounts of Diet Dr. Pepper & Diet Coke seem to cause plateauing of weight and decreasing the ability to shift into ketosis, especially mine. I’ve also noticed (in my personal n=1 experimentation) that my ability to fast after using caffeine regularly seems to be less tolerable, causing headaches and fatigue 8-10 hours into the fast, symptoms that don’t seem to let up until eating. Through the process of elimination, caffeine seems to be the culprit.
 After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the August 2004 Diabetes Care Journal screamed for my attention.
After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the August 2004 Diabetes Care Journal screamed for my attention.
It appears that caffeine actually stimulates a glucose and insulin response through a secondary mechanism. The insulin surge and glucose response is dramatically amplified in patients who are insulin resistant. Caffeine doesn’t effect glucose or insulin if taken while fasting; however, when taken with a meal, glucose responses are 21% higher than normal, and insulin responses are 48% higher in the insulin resistant patient. Caffeine seems to only effect the postprandial (2 hours after a meal) glucose and insulin levels. The literature shows mixed responses in patients when caffeine is in coffee or tea, probably due to the effect of other organic compounds (1).
Caffeine also diminishes insulin sensitivity and impairs glucose tolerance in normal and already insulin resistant and/or obese patients. This is seen most prominently in patients with diabetes mellitus type II (stage IV insulin resistance). Caffeine causes alterations in glucose homeostasis by decreasing glucose uptake into skeletal muscle, thereby causing elevations in blood glucose concentration and causing an insulin release (2-6).
Studies show that caffeine causes a five fold increase in epinephrine and a smaller, but significant, norepinephrine release. The diminished insulin sensitivity and exaggerated insulin response appears to be mediated by a catacholamine (epinephrine, norepinephrine & dopamine) induced stress response (5). Caffeine has a half life of about 6 hours, that means the caffeine in your system could cause a catacholamine response for up to 72 hours depending upon the amount of caffeine you ingest (7).
The reason for my, and other patient’s, headaches and fatigue after a short fast was due to the exaggerated stress hormone response. Increased levels of insulin were induced by a catacholamine cascade after caffeine ingestion with a meal, dramatically more amplified in a person like me with insulin resistance. The caffeine with the last meal cause hypoglycemia 5-7 hours into the fasting, leading to headaches and fatigue that are only alleviated by eating.
Even when not fasting, the caffeine induced catacholamine cascade causes up to 48% more insulin release with a meal, halting weight loss and in some cases, causing weight gain.
Caffeine is not the “Wonder-Boy” we thought it was.
How much caffeine will cause these symptoms? 50 mg or more per day can have these effects.
Ingestion of caffeine has the following effects:
The equivalent of 100 mg of in a human was given to a spider, you can see the very interesting effect on productivity. How often does the productivity of the day feel like the image below?

Beware that caffeine is now being added to a number of skin care products including wrinkle creams and makeup. Yes, caffeine is absorbed through the skin, so check the ingredients on your skin care products.
Diet Dr. Pepper, my caffeine delivery system of choice, has slightly less caffeine (39 mg per 12 oz can or 3.25 mg per oz) than regular Dr. Pepper. I found myself drinking 2-3 liters of Diet Dr. Pepper per day (long 16-18 hour work days in the office). After doing my research, I realized that my caffeine tolerance had built up to quite a significant level (230-350 grams per day).
So, a few weeks ago, I quit . . . cold turkey.
Did I mention the 15 withdrawal symptoms of caffeine? (8)
I experienced 13 of the 15 that lasted for 4 days. I do not recommend quitting cold turkey unless you have a week off and someone to hold your hand, cook your meals and dose your Tylenol or Motrin. My wife thought I was dying. . . I thought I was dying on day two. I actually had a nightmare about buying and getting into my own coffin. It can take up to three weeks to completely recover from caffeine withdrawal.
The other way to quit is to decrease your caffeine intake by 50 mg every two days. That means decrease caffeine by:
The benefit of this method is that withdrawal symptoms are much less severe without the caffeine headache and the ability to remain productive. It will take longer, but quitting cold turkey is not a pretty picture. Been there . . . done that, . . . and I’m not going back. I actually lost another half inch off my waistline by day 5 of caffeine discontinuation.
What is the take home message here? If you have any degree of insulin resistance, caffeine makes it worse and will amplify your weight gain as well as decrease the productivity of your day.
References:
How do you know if you're insulin resistant? What questions need to be asked? What should your numbers be? And, many other great ketosis questions. Also, why does Dr. Nally look like he has dirt on his chin? See it here . . .
Adrenal Fatigue? Adrenal Insufficiency? Cortisol? PseudoCushing’s Syndrome? What do these terms mean and why are they all over the internet these days? And, what do they have to do with your weight loss?
This was our topic this evening on PeriScope. Katch Dr. Nally speak about this topic with rolling comments at Katch.me/docmuscles. Or you can watch the video below:
If you’re not sure about what this is, you’re not alone. I think I’ve heard the term “Adrenal Fatigue” at lease four times a day for the last three months. If you ask your doctor, they’ll probably scratch their heads too. The funny thing is that “Adrenal Fatigue” isn’t a real diagnosis, but it is all over the internet and it shows up in the titles of magazines in the grocery store every day. There’s even and “Adrenal Fatigue For Dummies” so it must be real, right?! 
No. It isn’t a real diagnosis. It is a conglomeration of symptoms including fatigue, difficulty getting out of bed in the morning, and “brain fog” that have been lumped together to sell an “adrenal supplement.” (Sorry, but that’s really what it is all about.) Do a Google search and the first five or six sites describing adrenal fatigue claim the solution is taking their “special adrenal supplement.”
I know what you’re thinking, “Your just a main stream, Western Medicine doctor, Dr. Nally, you wouldn’t understand.” Actually, I do understand.
Adrenal fatigue has risen in popularity as a “lay diagnosis” because many patients show up at their doctors office with significant symptoms that actually interfere with their ability to function, and after all the testing comes back negative for any significant illness, they are told that they are normal. But the patient still has the symptoms and no answer or treatment has been offered. It’s discouraging. . . very discouraging.
That’s because the symptoms are actually the body’s response to chronic long term stress. Many of my patients, myself included, have found themselves “stuck” in their weight loss progression, feeling fatigued, struggling to face the day, with a number of symptoms including cold intolerance, memory decline, difficulty concentrating, depression, anxiety, dry skin, hair loss, and even infertility in some cases. Is it poor functioning adrenal glands? No, your feeling this way because the adrenal glands are actually doing their job!!
If the adrenal glands weren’t working you’d experience darkening of the skin, weight loss, gastric distress, significant weakness, anorexia, low blood pressure, and low blood sugar. The symptoms are actually called Addison’s disease and it is actually fairly rare (1 in 100,000 chance to be exact). So what is causing the symptoms you ask?
There are a number of reasons, but one that I am seeing more and more frequently is “Pseudo-Cushings’s Syndrome.” Pseudo-Cushing’s Syndrome is a physiologic hypercortisolism (over production of cortisol) that can be caused by five common issues:
The psychiatric literature suggest that up to 80% of people with depressive disorders have increased cortisol secretion (1,2,3).  People with significant stressors in their life have been show to have an increased corsiol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing a daily, cyclic over production of cortisol and then normalization of cortisol after resolution of the stressor. This cortisol response is not high enough to lead to a true Cushing’s Syndrome, but has the effect of the symptoms listed above and begins with limiting ones ability to loose weight.
People with significant stressors in their life have been show to have an increased corsiol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing a daily, cyclic over production of cortisol and then normalization of cortisol after resolution of the stressor. This cortisol response is not high enough to lead to a true Cushing’s Syndrome, but has the effect of the symptoms listed above and begins with limiting ones ability to loose weight.
I’m convinced that this is becoming more and more prevalent due to the high paced, high-stress, always on, plugged in, 24 hour information overload lives we live.
What is cortisol? It is a steroid hormone made naturally in the body by the adrenal cortex (outer portion of the adrenal gland). Cortisol is normally stimulated by a number of daily activities including fasting, awakening from sleep, exercise, and normal stresses upon the body. Cortisol release into the blood stream is highest in the morning, helping to wake us up, and tapers into the afternoon. Cortisol plays a very important role in helping our bodies to regulate the correct type (carbohydrate, fat, or protein) and amount of fuel to meet the bodies physiologic demands that are placed upon it at a given time (4,5,6).
 Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids or proteins into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues (by stimulating insulin production) and turns on the maturation process of adipocytes (it makes your fat cells age – nothing like having old fat cells, right?!) In the process, cortisol suppresses the immune system through an inhibitory effect designed to decrease inflammation during times of stress (7,8,9). If this was only occurring once in a while, this cascade of hormones acts as an important process. However, when cortisol production is chronically turned up, it leads to abnormal deposition of fat (weight gain), increased risk of infection, impotence, abnormal blood sugars, brain fog, head
Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids or proteins into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues (by stimulating insulin production) and turns on the maturation process of adipocytes (it makes your fat cells age – nothing like having old fat cells, right?!) In the process, cortisol suppresses the immune system through an inhibitory effect designed to decrease inflammation during times of stress (7,8,9). If this was only occurring once in a while, this cascade of hormones acts as an important process. However, when cortisol production is chronically turned up, it leads to abnormal deposition of fat (weight gain), increased risk of infection, impotence, abnormal blood sugars, brain fog, head
aches, hypertension, depression, anxiety, hair loss, dry skin and ankle edema, to name a few.
The chronic elevation in cortisol directly stimulates increased insulin formation by increasing the production of glucose in the body, and cortisol actually blunts or block-aids the thyroid function axis. Both of these actions halt the ability to loose weight, and drive weight gain.
Cortisol also increases appetite (10). That’s why many people get significant food cravings when they are under stress (“stress eaters”). Cortisol also indirectly affects the other neuro-hormones of the brain including CRH (corticotrophin releasing hormone), leptin, and neuropeptide Y (NPY). High levels of NPY and CRH and reduced levels of leptin have also been shown to stimulate appetite and cause weight gain (10-11).
How do you test for Pseudo-Cushing’s Syndrome?
Testing can be done by your doctor with a simple morning blood test for cortisol. If your cortisol is found to be elevated, it needs to be repeated with an additional 24 hour urine cortisol measurement to confirm the diagnosis. If Cushing’s Syndrome is suspected, some additional blood testing and diagnostic imaging will be necessary. Pseudo-Cushing syndrome will demonstrate a slightly elevated morning cortisol that doesn’t meet the criteria for true Cushing’s type syndrome or disease.
How do you treat it?
First, the stressor must be identified and removed. Are you getting enough sleep? Is there an underlying infection? Is there untreated anxiety or depression present? Are you over-exercising? These things must be addressed.
Second, underlying depression or anxiety can be treated with counseling, a variety of weight neutral anti-depressant medications or a combination of both. Many of my patients find that meditation, prayer, and journaling are tremendous helps to overcoming much of the anxiety and depression they experience.
Third, adequate sleep is essential. Remove the television, computer, cell phone, iPad or other electronic distraction from the bedroom. Go to bed at the same time and get up at the same time each day. Give yourself time each day away from being plugged in, logged in or on-line.
Fourth, mild intensity (40% of your maximal exertion level) exercise 2-3 days a week was found to lower cortisol; however, moderate intensity (60% of your maximal exertion level) to high intensity (80% of your maximal exertion level) exercise was found to raise it (12). A simple 20 minute walk, 2-3 times per week is very effective. Find a hobby that you enjoy and participate in it once or twice a week. Preferably, a hobby that requires some physical activity. The activity will actually help the sleep wake cycles to improve.
Fifth, follow a low carbohydrate or ketogenic diet. Ketogenic diets decrease insulin and reverse the effect of long term cortisol production. Ketogenic diets a have also been shown to decrease or mitigate inflammation by reducing hyperinsulinemia commonly present in these patients (13).
So, the take home message is . . . take your adrenal glands off of overdrive.
References:
Join me as we chew the phat of ketogenic lifestyles PeriScope style and answer many questions like, “Why do I get ‘hangry’?” What causes hypoglycemia? How many times a day should I eat? and many more . . .
We talk briefly about why 60% of people with insulin resistance may need methylated folic acid to help with B vitamin absorption/use and where it can be found. (See me recent article about this called The Power of a Good Vitamin.)
You can see the whole PeriScope conversation on Katch.me/docmuscles with the comments scrolling or you can see the video stream below:
Thanks for visiting!!!
I can’t help myself. Some days I enjoy a good murder mystery, but on others, I enjoy a good journal article elucidating our understanding of leptin. No, leptin is not a tiny Irish folk character or even a superhero. Leptin is a hormone. It’s made by fat cells. Anything made by fat cells becomes fascinating to a “fat doctor.”
Why is learning about leptin illuminating?
Well, if Sir Arthur Conan Doyle was an Obesity Specialist, the mystery would have been that Mr. Plump was killed by the wrench in the kitchen, but the wrench seems to have never left tool case in the garage. No one has been able to figure out how leptin, the allegorical wrench, plays its roll in lepin resistance. We know that a lack of leptin allows hunger to persist and a person without leptin will continue to eat without the sensation of feeling full – leading to obesity. What we haven’t understood is – what causes the brain to no longer sense larger and larger amounts of leptin being produced by those who are obese.
That is . . . we haven’t understood it until now. . .
We have known for some time that the hormone leptin is a key hormone produced by the adipose (fat) cells that suppresses hunger. A majority of obese patients in my clinic have elevated circulating leptin levels 2-10 times the normal levels. We know that a lack of leptin leads to obesity, but the patients that I see in the office are producing an over abundance consistent with leptin resistance. The leptin signal is not being recognized by the brain. This is very similar to type II diabetes and insulin resistance. The pancreas is producing an over abundance of insulin, but the cells are recognizing the signal to let the glucose in through the door way.

Three recent and very interesting studies have pointed to the probable cause. First, one of the most common genetic disorders causing human obesity is loss of function of the melanocortin receptor.

If the MC-4R receptor is broken, suppression of appetite is limited, continued eating occurs and weight gain continues. Leptin, produced by every adipose cell in the body, is carried in the blood stream to the brain and must pass through the blood-brain barrier. Once it crosses the blood-brain barrier and enters the hypothalamus, it has a stimulatory effect on the MC-3R receptor in the Arcuate Nucleus of the hypothalamus causing stimulation of the MC-4R receptor in the Parventricular Nucleus and Lateral Hypothalamus to turn off hunger.

However, if leptin cannot cross the blood brain barrier, the signal is never received from the adipose cells and continued eating without satiation (feeling full) persists. Studies have shown that dietary fructose ingestion alone or in combination with diets high in fat suppress the transmission of leptin across the blood-brain barrier.

Fructose is the primary component of high-fructose corn syrup, and makes up 45-50% of every other type of natural form of sugar (sucrose). Yes, it’s the major component found in table sugar, brown sugar, honey, agave, molasses and maple syrup. This is why a Paleolithic Diet isn’t fully effective for people with leptin resistance.

Lastly, anything that raises triglycerides inhibits leptin from crossing the blood-brain barrier.

Insulin has a direct effect on triglycerides. (See the articles “Insulin Resistance & The Horse,” “Fat Thoughts on Cholesterol,” “Ketogenic Living” and “So, What is this Ketogenic Thing?“). If your insulin levels go up, triglyceride production goes up. The patient with insulin resistance, pre-diabetes, impaired fasting glucose or type II diabetes produces between two to ten times the normal amount of insulin when eating the standard American diet (SAD diet). These patients have significant triglyceride elevation because of the high insulin response to carbohydrates in their diet. (Many of them were told by their doctor that “It’s just genetic so take your Lipitor.”) Statin drugs lower the LDL-C (calculated “bad cholesterol” level), but don’t reduce triglycerides effectively. Inadequate treatment of high triglycerides allows poor blood-brain barrier transmission of leptin and worsening leptin resistance.
In fact, this is the challenge and problem with the “frequent fasting” or “intermittent fasting” fad for weight loss that has been popping up in the blogosphere. If fasting reaches a state of starvation (which is a very fine line metabolically), it stimulates a stress response . . . causing a spike in cortisol, release of glycogen (a form of sugar), a compensatory release of insulin and a spike in triglycerides. If you have tried intermittent fasting and you’ve gained weight, you are probably not “fasting,” your probably “starving.” We’ve known for years that triglycerides are elevated in starvation. This diminishes leptin’s ability to cross the blood-brain barrier and leads to worsening leptin and insulin resistance.
High leptin levels caused by leptin resistance also seems to play a significant role in the development of diabetic retinopathy – damage to the tiny blood vessels at the back of the eye feeding the retina. Diabetic retinopathy starts insidiously without any symptoms initially and can lead to eventual blindness if not treated. Leptin seems to upregulate vascular endothelial growth factor (VEGF) which leads to narrowing of the blood vessels called “ischemia.” Chronic ischemia of the retinal vessels leads to damage to the delicate retinal cells of the eye.
So what do you do if you have leptin resistance. First, eliminate carbohydrates from your diet, especially sugars, high fructose corn syrup and any other form of simple sugar. This is why I am such a big fan of low carbohydrate, high fat diets.
Second, lower your triglycerides. This is done through decreasing overall insulin loads and is very effectively accomplished with a ketogenic diet. You can find this in my book, The KetoCure. Some additional great sources are KetoClarity, The Art and Science of Low Carbohydrate Living, and The Ketogenic Cookbook.
Third, use a supplement containing alpha-lipoic acid, carnosine high gamma vitamin E and benfothiamin (derivative of Vitamin B1). These have been demonstrated to decrease inflammation and render protection to the blood vessels.
The use of Epigallocatechin gallate (EGCg), a derivative extract of green tea, has been shown to repress hepatic glucose production, one of the insidious factors of insulin resistance, and may play a role in stabilizing the effect insulin has on production of triglycerides. You should consider using KetoEssentials. It is my specially formulated multivitamin that contains all of the above supplements, and includes methylated folic acid (B9), the necessary vitamin B6 & B12, chromium, vandium & zinc that help to further stabilize insulin resistance.
Fourth, get a good night’s sleep. Lack of sleep causes a stress response, increases cortisol, raises blood sugar and insulin leading to further leptin resistance.
Fifth, mild to moderate resistance exercise has been shown for years to improve insulin resistance significantly. If you’re not exercising, take a 20 minute walk 2-3 times per week, ride a bike for 20 minutes, start a weight lifting program, consider yoga or Pilates, Remember, jumping to conclusions, flying off the handle, carrying things too far, dodging responsibility and pushing your luck don’t qualify as resistance exercise.
Above all, if you’re having trouble losing weight, controlling insulin or leptin, see your doctor. He or she can really help.
References:
85% of the people that walk through my office doors have some degree of insulin resistance.
What is “insulin resistance?” It is an over production of insulin in response to ANY form of carbohydrate intake (yes, even the “good carbs” cause an insulin over-response in a person with insulin resistance.)
How do I know this? Because I routinely check insulin levels (I check them every three months) and the down stream markers of insulin on a large number of the patients that I see. I have been fascinated by the fact that a diet high in both sugar and fat [like the Standard American Diet, (SAD) diet] turn on the genetics leading to insulin resistance. Starch and sugar load the genetic gun.
Insulin acts like a key at the glucose doorway of every cell in your body. In many people, the insulin signal is blocked by hormones produced in the fat cell and the the insulin, acting like a “dull or worn out key” – can’t open the glucose doorway as efficiently.
So, the body panics, and releases extra insulin in response to the same load of carbohydrate or glucose. People with insulin resistance will produce between 2-20 times the normal amount of insulin in response to a simple carbohydrate load. Recent studies(1, 2) reveal high cholesterol and diets high in both fat and carbohydrate cause insulin resistance to progress or worsen.
So, instead of producing enough insulin to accommodate the one slice of bread or the one apple that you might eat, the insulin resistant person produces enough insulin for an entire loaf of bread or an entire bushel of apples. This excess insulin then stimulates one or all of the following:





If you are plagued by any or all of these, my first suggestion is to see your doctor and get screened for insulin resistance. I treat patients with these every day and have reversed these effects in thousands of patients with the correct diet and/or medications. Having seen these signs and patterns over the last 20 years of medical practice, I am still astonished every day by the dramatic effect our diet plays on the hormonal changes within the body. Remember that the food you eat is actually the most powerful form of medicine . . . and the slowest form of pernicious poison.
A ketogenic or carnivorous diet is your first step.
We take most insurances, however, check out my concierge program or my Direct Primary Care program if you are interested in an alternative to insurance.
References:
This post isn’t going to win me any friends . . . in fact, mentioning this topic a few days ago has already angered a number of them and resulted in an online tongue lashing by a few others. However, I can’t resist. And, based on some very persuasive data and personal experience, I don’t care.

Truth is truth . . . it doesn’t change no matter how you spin it, or attempt to fit it into your paradigm. The problem is what we have accepted in the last 40-50 years as “the scientific truth about getting healthy” is far from truth. By getting healthy, I’m implying the application of main-stream methods accepted to lose weight, reduce cholesterol, improve blood pressure and reduce your risk of heart disease and diabetes. 
For the last 40 years we’ve been told that the only way to get and live healthy is to restrict our calories. This main-streamed advise continues even today in our USDA 2010 Dietary Guidelines. And, if you ascribe to this futile dogma propagated since the 1970’s, then you’ll know that the “only acceptable way” to do this is to “eat less fat” (because fat is the most caloric dense of the macro-nutrients, right?) and to “exercise more” (because that’s how we burn calories, right?!) Well, that’s what I thought, too. And that  is the health prescription I doled out to my-self and to all of my patients for the first 8 years of my practice.
is the health prescription I doled out to my-self and to all of my patients for the first 8 years of my practice.
Interestingly, most of them, including myself, took that prescription of a caloric restricted diet of 1200-1500 calories per day and exercise 3-6 days a week for 30-60 minutes and ran with it. Personally, I restricted calories to 1200-1500 per day and began running triathlons. I performed cardiac monitored running, swimming and cycling for an hour a day during the week and 2 hours on the weekend. I lifted weights 2-3 days per week as well. Guess what it got me?  Fat.
Fat.
It raised my triglycerides by 100 points, elevated my LDL-C and increased my waistline by 3 inches. Yes, I gained weight. But, hey, my doctor was happy because my HDL-C went up by 4 points.
I saw this identical pattern with 3/4ths the patients in my office. A fourth of my patient’s (the group without any genetic insulin resistance) saw weight loss and improvement in their cholesterol profiles, but the rest didn’t. I had the exciting opportunity to introduce the saddened and discouraged 3/4ths of my patients to STATIN drugs and blood pressure medications. My average patient’s gained 2-3% of their body fat each year. Those that exercised like fiends were lucky if their weigh gain just stabilized. 
What I saw in my office over a period of eight years was that exercise and caloric restriction didn’t work. But I couldn’t say that, because that goes against everything your 8th grade health teacher taught you. It contradicted your neighborhood dietitian, and it spat in the face of the food pyramid and the USDA Guidelines. The Government wrong? Never. . . . Speaking contradictory of the calorie-in/calorie-out exercise dogma was heresy, right? Contradict, Dr. Ornish, wouldn’t be heard of?!!
If I’ve learned one thing in my medical career, it is this: “Don’t be afraid to question everything” – even Dr. Dean Ornish, the USDA and the American Heart Association. And, fascinatingly, I’m not the only on that did.
——
——
Three Massive Studies did just that . . . question whether this exercise and caloric restriction dogma really works. This is what applying exercise and caloric cutting did for almost 67,000 people between 1972 and 2010 – little to nothing.
WHAT?!! Nothing?! You can’t be serous?
The first of these trials was the MRFIT (Multiple Risk Factor Intervention) Trial. It started in 1972, looking at 12,866 men with high risk for heart disease and followed them over seven years. All of them were placed on caloric restricted low fat diets and encouraged to exercise. It demonstrated that low fat diets and exercise FAILED to reduce weight or stop coronary artery disease in 100% of the cases. Don’t believe me? Read it for yourself (JAMA. 1982; 248 (12):1465-1477).
The second of these trials was the Women’s Health Initiative (WHI). This study started in 1991 and followed 48,835 women (yes, that’s a small city of women) for eight years. They didn’t believe the MRFIT results apparently, so they had a low fat (caloric restricted) arm and a control arm [the SAD diet (Standard American Diet)]. The women on the low fat arm lost a whooping 0.4 kg over the 8 year period (JAMA. 2006 Jan 4;295(1):39-49). 0.4 kg, really!?? That’s almost an entire pound of weight loss over 8 years. Quick, call Barnes & Noble so we can package that diet and sell it on Opra!! (Oh, wait, the news media was a little embarrassed by the findings and never really mentioned them.)
Lastly, if research on 60,000 men and women wasn’t enough to demonstrate what most primary care physicians seen in their offices daily, we had to do the Look AHEAD Study (Action for Health in Diabetes). This study started in 2001 and was supposed to run for 13.5 years. It studied 5,145 Type II diabetic patients with intensive lifestyle intervention. These patients were placed on intensive caloric and fat restriction of 1200-1800 calories per day with exercise and behavioral counseling. It was so unsuccessful, that they stopped the trial at 9.6 years – cause it wasn’t working.
The patients did lose some weight through Look AHEAD . . . an average of 6% of their body fat (That means you would have lost 15.6 lbs over 9 years if you weighed 260 lbs. Successful? . . . NOT). What made this trial worse is that it didn’t improve risk for coronary artery disease and people didn’t live longer (N Engl J Med 2013; 369:145-154). They just got the exciting chance to eat cardboard for 9 years of their lives. Sad. Very sad.

So, what does all this mean? Exercising your brains out at an expensive gym every morning won’t do much more than help you loose 1% of your body fat. It won’t increased your life span and it won’t decrease your risk of heart disease, despite what Dr. Ornish said. If you like spending $40 per month just to stare at sweaty fat bodies jumping up and down in spandex, by all means, please keep going to the gym. But I’d much rather spend that $40 on a nice rib eye steak at a restaurant staring at my wife. But, the benefits of saturated fat . . . that’s for another post.
Don’t get me wrong. I love lifting weights. I love riding my horse. I truly enjoy working in my yard. I even enjoy riding my bicycle. But I do these things now because they bring me peace, decrease my stress, and allow me to connect with nature. Believe me, there’s nothing natural about a 250 pound man in spandex staring at himself in a mirror repetitively lifting 30 pound bars of iron. But, we won’t go there.
My friends, and a few of my patients, get their knickers in a wad trying to decry the fact that I’m giving people a reason not to go running. Maybe I am. To be honest, there’s really only one reason I want to run, . . . and that’s when I’m being chased by a bear. But what good does it do to guilt a person into participation in an activity that isn’t really benefiting their health or help them lose weight, unless they really truly enjoy the activity for the sake of the activity?
Our health is not based upon a caloric scale of inputs and outputs. We are hormonal machines. We gain or lose weight and we gain or lose muscle based on powerful hormone signals, specifically insulin. Simple carbohydrate restriction has profound effects upon our weight, blood pressure, cholesterol and inflammatory states. Until we each come to grips with the fact that the food we eat triggers hormone responses in our bodies, we will continue down the path of diseases of civilization. Hippocrates summed it up when he said, “Let food be thy medicine, and let medicine be thy food.”
Have you noticed that there are a large number of advertisements in the media about checking your testosterone or “Low T” Syndrome? It seems like this is the new advertising trend on the radio and late night TV.
Suddenly, everyone’s testosterone is low and men are complaining about their libido, . . . or are they?

If you practice medicine long enough, you’ll see a trend that seems to have arisen as our waistlines have expanded. About half of the men in my office with insulin resistance, pre-diabetes or diabetes have low testosterone levels. But this shouldn’t be a surprise. Type II diabetes, metabolic syndrome and insulin resistance are all driven by an over production in insulin in response to a carbohydrate load in the meal. Patients with these conditions produce between two to ten times the normal insulin in response to a starchy meal. A number of studies both in animal and human models demonstrate that insulin has a direct correlation on testosterone suppression in the blood. This has been demonstrated in both men and women. In fact, glucose intake has been shown to suppress testosterone and LH in healthy men by suppressing the gonadal hormone axis and more predominant testosterone suppression is seen in patient with insulin resistance or metabolic syndrome.

In fact, to put it simply, insulin increases the conversion (aromitization) of testosterone to estrogen in men (it does the opposite in women). Interestingly, Leptin resistance has a similar effect. I tend to see the worst lowering of testosterone in men with both insulin and leptin resistance.
How to you improve your testosterone? Supplemental testosterone has been shown to help, but it comes with some risks, including prostate enlargement and stimulating growth of prostate cancer. The most natural way to improve your testosterone is to change your diet.
A low carbohydrate or ketogenic diet turns down the insulin production and allows the testosterone to be available for use by the body. A ketogenic diet has the effect of reducing leptin resistance as well through weight loss. A simple dietary change of this type is frequently seen in my office to increase testosterone by 100-150 points.

What is a ketogenic diet? It is a diet that restricts carbohydrates to less than 50 grams per day, thereby causing the body to use ketones as the primary fuel source. So, for breakfast tomorrow morning, hold the oatmeal (1/2 cup of Quaker Instant Oatmeal is 31 grams of carbohydrates) and have the bacon and eggs. And, rather than have the cheesecake for desert this evening, have an extra slice of steak butter on your rib-eye and hold the potato.
I have multiple patients that come to my office that we follow and treat for weight loss and metabolic syndrome. They are discouraged that their weight loss has stopped or is very, very slow. The most frequent problem I find when they bring in their food journals is the “healthy chicken salad.”
“What?! But, Doc, Chicken Salad is healthy?! RIGHT?”
The chicken salad shows up on their journal almost daily. Somehow, we’ve been indoctrinated that the chicken salad is good for us. I want you to look closely at the image that was recently shared on the internet below. How is the nutrient value of your chicken salad any different than the Big Mac?

Why is this unhealthy? The carbohydrate content greater than 20-30 grams will cause a spike in insulin. When insulin spikes, the body is told to store fat (and it will store fat for up to 12 hours) . . . Yes, the 24 grams of fat in the salad now become dangerous in the presence of an insulin spike. In my patients with metabolic syndrome, they will produce between two and ten times the insulin and store two to ten times the fat. (Ten Big Macs would have tasted better . . . )
There is actually more carbohydrate in your salad than in the big mac. Why not add a strawberry shake just to finish putting the nail in the coffin? And we wonder why we are having trouble with weight loss?
The other issue, and probably of even greater importance, is that chicken breast has the second highest content of lysine & argenine (two of the 10 essential amino acids) count of all the poultry family. This is second only to turkey breast, which also contains a large amount of tryptophan (a third essential amino acid that spikes insulin). Why is this a problem? Because argenine, tryptophan and lysine all stimulate an insulin response on their own, separate from glucose. We need these amino acids, however, when our meals contain a predominance of these amino acids, it rasies insulin significantly in those who are insulin resistant (pre-diabetic).
Those 43 carbohydrates, plus the stimulus from a meat high in argenine, lysine and tryptophan, spike your insulin, kick you out of nutritional ketosis and slow weight loss for up to 48 hours.
Please, if you are following a low-carb or ketogenic diet, get rid of the chicken salad.
If you want to learn more about this, read my article on the eight most common reasons you can’t lose weight.
A number of patients come in to the office struggling with loosing weight. When I review their dietary journals with them, I notice that many of them never stop eating fruit (because, fruit is good for you, right?!). Well, lets put it this way:
One banana for breakfast is equal to . . .

. . . just over seven (7) teaspoons of sugar.

Count them . . . seven (7) teaspoons.
If your eating a banana for breakfast, it is halting your weight loss for up to 12 hours. Give the banana’s to the monkeys and cook up some sausage and eggs for breakfast tomorrow.
Now you have to watch your salt ingredients too. Store bought salts are starting to add dextrose for flavor. Dextrose is just another word for SUGAR!! Aaarrrrhhhhh!! Why do you need to add sugar to your salt? You don’t. Throw out any salt that contains dextrose. It will raise your cholesterol and cause weight gain.

Never noticed this until it was pointed out by Maria Emmerich. Thanks, Maria.