Today’s Periscope with Jimmy was a teaser for what is to come. I will be joining Jimmy Moore to create a new weekly podcast to address “Keto Questions” you may have. Stay tuned for more information . . .
The amazing Jimmy Moore and his wonderful wife, Christine, will be stopping by my office on Monday, September 28th, 2015, between the hours of 9 am and 1pm. Jimmy Moore, Podcaster for Livin’ La Vita Low Carb and author of The Ketogenic Cookbook, KetoClarity and Cholesterol Clarity has been in Phoenix this weekend and agreed to visit the office.
I have been recommending his books and website to my patients for years. His website, books and podcasts have served as superb resources for Low-Carb, High Fat and Paleo dietary programs and patients just starting or fine tuning their programs.
Jimmy and his sweet wife, Christine, have become great friends and trusted colleagues over the years as new science and treatment protocols have been identified in the treatment of obesity, insulin resistance and diabetes. He has been a resource for me and my patients for over 10 years.
Pick up your copy of these books at Barnes & Noble or your favorite nearby bookstore; and if you are in the neighborhood and would like meet Jimmy, bring your copy of the Ketogenic Cookbook, KetoClarity or Cholesterol Clarity to get signed and shake his hand.
If you haven’t checked out his podcasts on Livin’ La Vita Low Carb, or seen his Periscope casts on JimmyScopes.com you need to click on the links and check them out.
I’ve heard this question at least 5-6 times per day for the last 20 years. The problem has been, there hasn’t been just one or two products that fit my or my patient’s needs. I’ve seen many that are close, but no one seems to understand the needed nutrients for insulin resistance, leptin resistance and the tremendous effect adequate nutrients has on inflammation, atherosclerosis, uric acid, sodium balance, cholesterol and blood pressure. That is, until I found a company that would let me design my own vitamin.
Working with a world renowned lab, I put together what I know to be the best ketogenic multivitamin on the market. I give you the “KetoNutritionals Multivitamin.”
It provides the nutrients that we recognize are essential to the TCA (tricarboxylic acid) or Krebs cycle. I call it the Multivitamin Adult Formula, because it has the potential to enhance the body’s ability to use insulin, leptin and regulate normal blood sugar and maintain ketosis. Now, it is essential that I inform you that these statements have not been evaluated by the FDA and that this product is not intended to diagnose, treat, cure, or prevent any disease.
Methylated Folic Acid
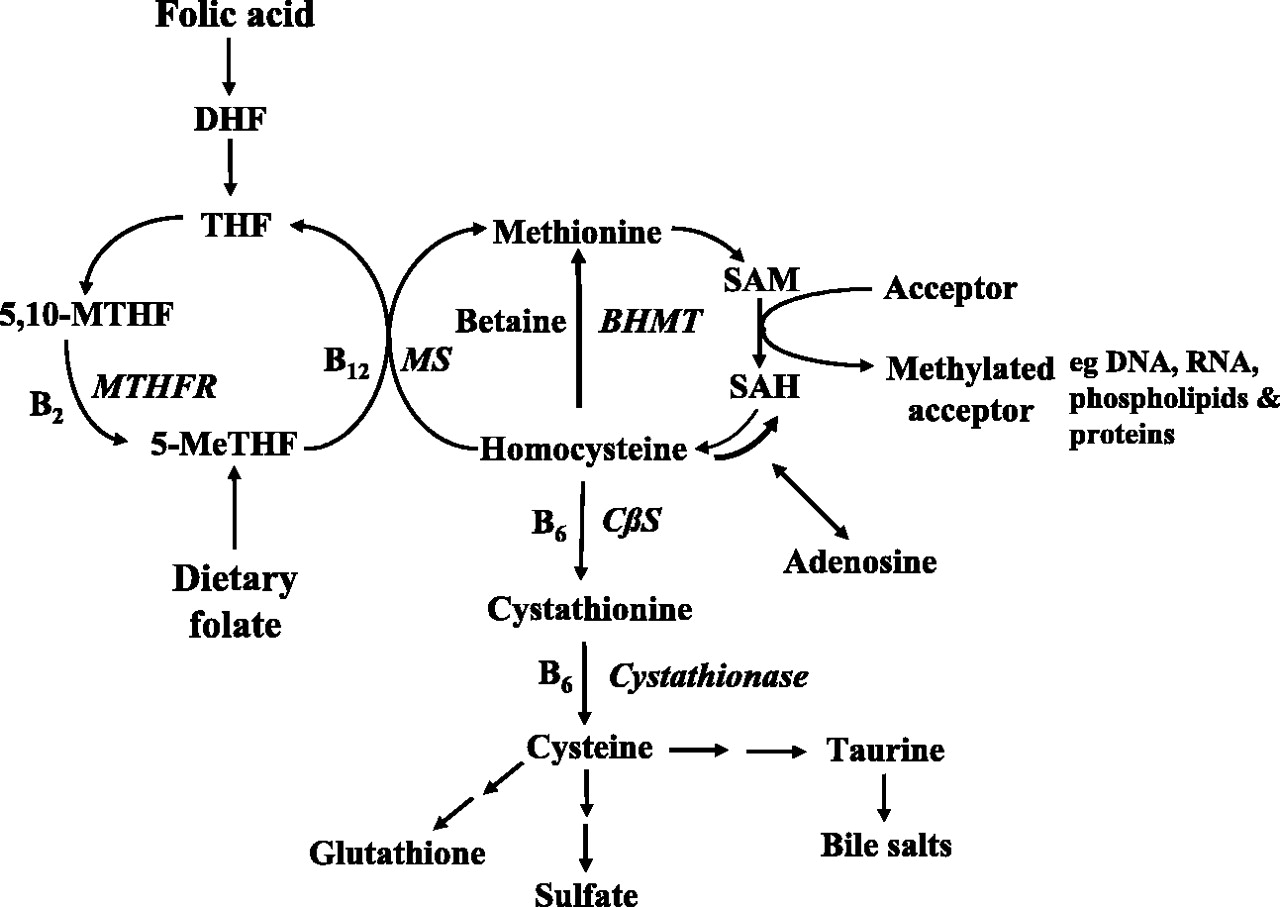
However, 60-65% of pre-diabetic and diabetic patients I see in the office do not correctly convert Folic Acid (Vitamin B9). It is suspected that over 40% of the population in general has a genetic deficiency in the gene that codes for MTHFR. MTHFR (also called methylenetetrahydrofolate reductase) is a genetic sequence that encodes for an essential enzyme in your body that helps make the active form of folate. Your body cannot make folate on its own, so it requires enzymes including the one encoded by the MTHFR gene, to make it from the foods that you eat. MTHFR enzyme also has an important role in making amino acids, the building blocks of proteins, by helping convert the chemical homocysteine to methionine in concert with Vitamin B12. Homocysteine is a harmful chemical made by your body that can damage the lipid membrane of cells leading to damage of the walls of your blood vessels, and may affect your blood clotting. In contrast, methionine is an amino acid required by your body for normal functioning. Supplementing the methylated folate helps to provide the needed components for methionine production. KetoNutritional Multivitamin contains both forms of active isomer, naturally occurring folates. MTHFR deficiency can easily be tested for through a simple saliva test in the office.
Metabolism of folate and homocysteine. American Journal of Physiology – Heart and Circulatory Physiology Published 1 July 2004 Vol. 287 no. 1
The conversion of methionine to SAMe is essential in this pathway. SAMe (pronounced Sammy) is necessary for methylation. It is essential in the formation of neurotransmitters like serotonin and liver detoxification through the methylation pathway. Serotonin is key in the treatment and prevention of depression, chronic pain, and liver detoxification. In a number of cases, just fixing this methylation has dramatically improved symptoms of depression that would have otherwise been treated with strong psychogenic medications.
N-Acytylcysteine
Cysteine is used by the body as a source of sulfur for detoxification and the production of glutathione. Glutathione is your body’s chief anti-oxidant and protector against all kinds of damage. This is where Vitamin B6 plays a major role. Vitamin B6 is also a cofactor in hundreds of different chemical reactions necessary for healthy hormones like estrogen, and progesterone. It is also essential for the production of neurotransmitters like serotonin, dopamine, and GABA for proper brain function.
Carnosine
KetoEssentials contains the essential vitamins to allow these metabolic pathways to function properly. May people on a ketogenic diet don’t get the full effect of weight loss until adequate Vitamin B12 and Vitamin B6 are supplemented. It also contains Vitamin B1, and carnosine that have been found to decrease the effect of inflammatory glycation and damage caused by higher blood sugars like diabetic retinopathy. High gamma Vitamin E has also demonstrated retinopathy protection.
Alpha Lipoic Acid, Taurine, ECGC
Alpha lipoic acid combined with biotin has been shown to augment a more natural, healthy insulin secretion thereby promoting a more effective glucose metabolism. Taurine, epigallocatechin gallate (EGCg) from green tea and Vitamin D have all been shown to improve the effect of the insulin you produce.
Improving insulin use and production has a direct effect your triglycerides. We now know that when your triglycerides are “out -of-whack,” leptin transport across the blood brain barrier is affected and this worsens your risk leptin resistance. Leptin is that amazing hormone that tells your brain that your fat cells are “full” and to stop eating.
Vitamin A
Vitamin A as a carotenoid acts helps aid immune function and Molybdenum aids in detoxification processes in the body.
Zinc
Added zinc, taurine and EGCg to reduce the damaging effects that fructose can have in the liver, and also enhancing your insulin signaling. Added zinc also helps stabilize your testosterone and sex hormones.
Chromium, Manganese, Vanadium
But, these vitamins and anti-oxidants don’t help if they’re not absorbed correctly, so magnesium, chromium, zinc, manganese and vanadium help to enhance absorption. Correct supplementation of these nutrients may have the effect of normalizing glucose, insulin and leptin levels an reduction in risk for long term cardiovascular disease, diabetic complications, water retention, and more effective weight loss.
Moat SJ, Doshi SN, Lang D, McDowell IFW, Lewis MJ, Goodfellow J. “Treatment of coronary heart disease with folic acid: is there a future?” American Journal of Physiology – Heart and Circulatory Physiology Published 1 July 2004 Vol. 287 no. 1, H1-H7 DOI: 10.1152/ajpheart.00952.2003
Hipkiss AR, Brownson . Reaction of carnosine with aged proteins: another protective process? Ann N Y Acad Sci. 2002 Apr;959:285-94.
Waltner-Law ME, Wang XL Epigallocatechin gallate, a constituent of green tea, represses hepatic glucose production. J Biol Chem. 2002 Sep 20;277(38):34933-40. Epub 2002 Jul 12.
Jacob S, Ruus P, Hermann R, Oral administration of RAC-alpha-lipoic acid modulates insulin sensitivity in patients with type-2 diabetes mellitus: a placebo-controlled trial. Free Radic Biol Med. 1999 Aug;27(3-4):309-14.
Boucher BJ . Inadequate vitamin D status: does it contribute to the disorders comprising syndrome ‘X’? Br J Nutr. 1998 Apr;79(4):315-27.
Hammes HP, Du X . Benfotiamine blocks three major pathways of hyperglycemic damage and prevents experimental diabetic retinopathy. Nat Med. 2003 Mar;9(3):294-9. Epub 2003 Feb 18.
Maassen JA, Mitochondrial diabetes, diabetes and the thiamine-responsive megaloblastic anaemia syndrome and MODY-2. Diseases with common pathophysiology? Panminerva Med. 2002 Dec;44(4):295-300.
Ozcelikay AT, Becker DJ. Improvement of glucose and lipid metabolism in diabetic rats treated with molybdate. Am J Physiol. 1996 Feb;270(2 Pt 1):E344-52.
Banks WA, Coon AB, Robinson SM, Moinuddin A, Schultz JM, Nakaoke R, Morley JE. Triglycerides Induce Leptin Resistance at the Blood-Brain Barrier. Diabetes May 2004 vol. 53 no. 5 1253-1260.
ery October I get a hankering for homemade root beer. But it is usually loaded with sugar. Thanks to Maria Emmerich and her amazing recipes, that doesn’t have to happen this year. She just posted this on her site today and I can’t wait to try this as I sit by my fire pit roasting some hot dogs with my kids . . . Thanks Maria.
I pasted a copy of her root beer image below just to make you drool, too . . .
I found these charts to be very helpful when trying to calculate your fat intake with a meal. Fish can be challenging in calculating fat content. After reading these charts, I’m craving some sashimi’ed mackerel and salmon.
I’ve personally been following and prescribing ketogenic diets to my patients since 2005. When I started on my ketogenic journey, it was called a “Low Carbohydrate Diet.” Over the last 5-10 years, we’ve learned a thing or two about how the body processes carbohydrate, protein and fat. Specifically, it’s not just the restriction of the carbohydrates that leads to metabolic health, but appropriate protein intake and significant emphasis on the level and type of fat intake as well. The majority of people who cut out carbohydrates will initially see successful weight loss, but to maintain that weight loss and see significant metabolic changes that reverse the diseases of civilization, an understanding of protein and fat needs are essential.
It’s Not Necessarily a High Protein Diet
Most people, when they hear you’re following a “Low-Carb” diet . . . respond with, “Oh, you are on that high protein, Adkins’ thing, . . . right?!”
Well, not really. A true ketogenic diet is NOT a “high protein diet.” However, you must be ingesting enough protein to maintain muscle, hair growth and energy levels. Most people, having been brainwashed in grade school and middle school about the horrors of fat in the diet, assume that if you’re not eating carbohydrates, then you must be eating extra protein to stay satiated. (No one would ever intentionally increase the fat in their diet, right?!!) However, remember that protein and fat usually come together in the sources that the Good Lord put them in.
That’s the impression that most people in my office get when I mention the words “Low-Carb” or “Adkins.” And, before I have a chance to explain that I’m not recommending that you race home to eat three large turkey legs and a pound of turkey bacon, the vegetarians gather their things to leave and the former home economics teachers begin to get chest pain at the mental picture in their heads.
How Are Ketones Made?
A ketogenic diet is one which allows your body to use ketones as it’s primary fuel source. Ketones are produced from the breakdown of triglyceride and free fatty acids. Ketones are essentially produced by two distinctly different events:
1) Starvation caused by prolonged periods without food (which is essentially what happens to type I diabetics when they have no insulin at all in their systems)
2) When fat is ingested as the primary fuel, and very low levels of insulin are concurrently produced, primarily when the diet has minimal to no carbohydrate present (allowing the body to activate its free fatty acid reserves found within in the adipose cells).
The body is an amazing machine. It was designed to take any of the three main macro-nutrients (carbohydrate, protein or fat) as fuel and function quite well. It’s like a futuristic car that can run on unleaded gasoline, oil, or diesel fuel. It is able to recognize which fuel is present and run quite well off of any of the three. The amazing thing about the body is that we mix up all three fuel types and just pour them into the tank. Impressively, the body can separate them out and run very well in the short term on any combination of mixes. We don’t have cars or trucks that do that today . . . maybe in the future . . .?
We have Two Fuel Systems
I like to equate carbohydrates to unleaded fuel. These are clean burning, easy to access and cheap. However, the body requires the production of insulin to use this “unleaded” type of fuel. When carbohydrates are identified to be present in the liver and pancreas, insulin is released so that the rest of the cells throughout the body can “open the tank” and let the carbohydrate into the cell to be used as fuel. The challenge is that carbohydrates don’t store very well in the form they are supplied in, so, as a protective mechanism against starvation and famine, if excess carbohydrate is found in the system, it is converted into triglyceride. Insulin is required for this. Interestingly, when your insulin levels rise, the signal to the body is that “unleaded fuel” is in the system, so it stores any fats and excess carbohydrates in the form of free fatty acid and triglyceride. Carbohydrate stimulate an insulin response and cause fat storage. It is the same reason we give corn to cattle — to plump them up before taking them to market.
Fat then is the “diesel fuel” of macro-nutrients. It burns well, can be stored very easily, and provides over twice the energy to the body when measured in the form of k-cal per gram. Fat is used preferentially when there is limited or no insulin floating around the blood stream and is quickly and efficiency stored when other forms of fuel are available. (Insulin being the key hormone signaling that other fuel is around.)
Nutritional Ketosis is Using Fat as Your Optimum Fuel
So what is this “ketosis thing?” It is a method of dietary change (a lifestyle) that intentionally focuses the body’s metabolism to use fat (in the form of triglyceride & free fatty acid) as its primary fuel. Leading to weight loss, dramatically improved blood sugars, significantly improved cholesterol and triglyceride levels, and notably improved inflammatory markers.
“But don’t you end up eating a lot more protein on your weight loss program?” I frequently get asked.
Honestly, No.
Protein and fat are both very filling, and most people find that limiting the carbohydrates actually causes less hunger and diminishes the rebound carbohydrate cravings often stimulated by the two or three slices of bread, pasta or that potato often occurring 2-3 hours later. Interestingly, most people don’t eat that much more and the protein levels remain fairly constant. Because fat and protein come together in meats, eggs, fish, etc., satiation occurs with just minor increases in dietary intake real animal food. I don’t recommend increase the fat alone. I recommend increasing the amount of real animal protein until you are full. This is even more satiating and many people find themselves eating only twice a day when they are hungry.
Excessive protein in those who are morbidly obese with severe overproduction of insulin can experience a spike the insulin levels further with large amounts of protein. Protein can be equated to the oil you put in your car. Protein is a building block used for muscle, connective tissue and some essential metabolic functions. When too much protein, in this group is ingested, it spikes the insulin. (See my article on Why Your Chicken Salad is Making you Fat)
Most people have problems when they start supplementing with protein shakes. These often contain sweeteners that raise insulin and consequently halts your weight loss – or even causing weight gain.
I recently read a blog post decrying anyone that would recommend a low carbohydrate / ketogenic diet to their patients.
What?!
In fact, this particular blog outlined a number of “adverse reactions” to a ketogenic diet, and based upon these perceived reactions, the writer advised severe caution with its use in just about anyone. It is important to note at the outset that most of the data this blogger quotes are from older studies completed in children for the treatment of epilepsy with specific liquid ketogenic dietary meal replacements. (Not what you’d expect in a low-carb / ketogenic diet for the average obese adult today.)
Diet Confusion
Thanks to recent misinformation by a number of medical professionals, including the person writing the blog referenced above, a poor understanding of fatty acid metabolism by the general community, and a distinct lack of understanding of human adaptability recorded over the last 5,000-6,000 years, there is still significant confusion about ketogenic diets.
It is important to recognize the crucial fact that the human body is designed to function quite well when supplied any of three macronutrients: carbohydrates, proteins or fats. It does so through an amazing series of enzymatic reactions referred to as the Krebs (tricarboxylic acid) cycle, producing needed ATP (adenosine triphosphate) required for our muscles to contract, our heart to beat and our diaphragm to expand our lungs. What’s even more amazing that that the body was designed to recognize the season we are in based up on the food we eat. That is, until we invented refrigerators in 1913. (Now our bodies think it’s year round summer time . . . wait . . . I live in Arizona where it is year round summer time.)
No, this is not a post about unplugging your refrigerator, living on solar, getting off the grid and saving energy.
Our bodies recognize the seasons we are in based upon inherent hormone release. The key hormone is insulin. Insulin can be looked at as the seasonal indicator to our bodies. Insulin production rises and falls based on our intake of carbohydrates (sugar, starches, some fibers). Insulin, essentially, tells our bodies when it is a “time of plenty” and when it was a “time of famine.” Why? You ask. We didn’t have refrigerators 100 years ago and you were lucky if you had a root cellar. The body needs to know when to store for the famine (the winter) that was around the corner. Insulin is that signal.
During the summer, potatoes, carrots, corn and other fruits are readily available. These are all starchy carbohydrates and they all require the body to stimulate an insulin response so that they can be absorbed. Insulin stimulates fat storage (J Clin Invest. 2000;106(4):473-481. doi:10.1172/JCI10842). Just like bears, our bodies were designed to store for the winter.
If you think back in history, your grandparents probably used stored meats & cheeses that could be salted or smoked for preserving during this time of year. Those crossing the plains were commonly found with pemmican, a concentration of fat and protein used as a portable nutrition source in the absence of other food. (Chapter VIII. Narrative of the Life of David Crockett, of The State of Tennessee, Written by Himself, Sixth Edition [E.L. Carey and A. Hart:Philadelphia] 1834, 1837; Marcy, The Prairie Traveler, p. 31.) Think about conversations you may have had with your grandmother when she told you that for Christmas, she received an orange. A single orange for a gift?! Many of my patients drink 12-15 of them in a glass every morning. The winter diets of our grandparents were very low in starches and carbohydrates. When carbohydrate intake is low, little insulin is produced.
Again, insulin is the hormone that tells you that you’re in “a time of plenty” and stimulates weight gain and cholesterol production to prepare for winter. Those prescribing the use of ketogenic diets understand this innate human adaptive trait, and use it to effect changes in weight, cholesterol and other desired metabolic changes.
Three types of ketones. Uptodate.com, May 2015
Now, let’s define the difference between ketosis and keto-acidosis and try to clarify the misinformation that is being spread around the blogosphere.
A ketone is a molecule the body produces from the breakdown of fat and some proteins (amino acids). There are specifically three types of ketones: beta-hydroxybutyric acid, acetoacetic acid and acetone. If ketosis was “bad,” then why would our bodies produce these molecules? They are not bad, and in fact, multiple studies show that the body is often more efficient and effective when it functions on ketones rather than glucose as its primary fuel source. The body can only supply a limited amount of sugar or glucose for fuel. If you talk to runners, marathoners or triathletes, they will tell you that after about 45-90 minutes of continuous endurance exercise the glucose supply runs out and they will experience what is termed a “bonk” (have a low-blood sugar or hypoglycemic episode). Unfortunately, our bodies can only store about 18-24 hours of glucose.
Metobolic Changes of Ketogenic Diet (American Journal of Physiology – Endocrinology and Metabolism Published 1 June 2007 Vol. 292 no. 6, E1724-E1739 DOI: 10.1152/ajpendo.00717.2006)
However, the body can store days upon days of fat in the form of triglyceride in the fat cells. Triglyceride is broken down into ketones. If glucose is the “unleaded” fuel, you can think of ketones as the “diesel fuel” that is easier to store and runs longer.
The average body functioning on ketones as the primary fuel will have a ketone level measured in the blood somewhere between 0.4 and 4 mmol/L. Because of a balance that is created by the use of ketones and a feedback mechanism that kicks in when the ketone level rises, the body will maintain a pH of around 7.4.
Ketoacidosis is dramatically different. If you are a type I diabetic, you don’t produce any insulin. The feedback mechanism regulating ketone use is broken and the ketone levels and triglyceride breakdown speeds up because the body can’t access glucose and can’t produce insulin. The ketone levels spike and the level can rise to > 25 mmol/L. In the presence of a high blood sugar and high ketone level, the acid level in the blood shifts to a pH of less than 7.3. This is referred to as metabolic acidosis and can be life threatening as the low pH shuts down the bodies’ enzymatic processes and a person becomes critically ill and without treatment, can die. (Kitabchi AE et al., Clinical features and diagnosis of diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults. www.uptodate.com, May 2015.)
If you’re not a type I diabetic, you have nothing to worry about. Regardless of what the “ketogenic nay-sayers” blog about, your liver makes approximately 240g of glucose per day, this stimulates a basal release of insulin which keeps the pH in check. It’s also what keeps weight loss at a consistent pace of around 2-10 lbs per month.
If you are a type I diabetic, don’t fret. Carbohydrate restriction can still be used very effectively. It just takes some balancing and understanding of your individual metabolism. Talk to your physician and/or medical bariatrician about how to follow a carbohydrate restricted diet while using insulin.
What about all the other “adverse effects” the blogosphere and other so-called experts claim about ketogenic diets?
Let’s take them on one by one. Are you ready?
Gastrointestinal (GI) disturbances – Yes. Any time you change your diet you may experience diarrhea, constipation or gassiness. Most of the time, this is because you are either 1) not eating enough leafy greens (fiber) or 2) you’re using a supplement that contains an artificial sweetener. Most of the studies on ketogenic diets did not incorporate fiber and the studies used to make this point were on children who used a ketogenic fat supplement shake or liquid preparations containing these artificial sweeteners to make them palatable. If you have spoken to any bariatrician, they will tell you, the best way to follow a ketogenic diet is to eat real food. If you want to read about the anecdotal GI effects of sweeteners, read the comment section in Amazon about the Haribo Sugar Free Gummy Bears.
Inflammation Risk – In every patient that I have placed on a ketogenic diet in the last 8 years, all inflammatory markers including CRP, Sedimentation Rate and Uric Acid have all decreased. Inflammation gets better on an appropriately formulated ketogenic diet. The older studies of ketogenic diets in children contain most of their fat from Omega-6 fatty acids from vegetable oil which will increase inflammation and oxidative stress, spike the cortisol levels and have the secondary effect of actually raising the triglycerides. (Simopoulos AP,The importance of the ratio of omega-6/omega-3 essential fatty acids, Biomed Pharmacother., 2002 Oct;56(8):365-79.)
Muscle Cramps/Weakness – The process of weight loss occurs by burning fat into CO2 and water. We breathe the CO2 out, but the water produced has to follow salts out through the kidneys. Hence, we lose salts. This can cause weakness and muscle cramps. The solution? Stop restricting salt on a low carbohydrate diet. We are the only mammal that restricts salt and we do it because low-fat diets cause us to retain water. Low carbohydrate diets do the opposite. Use sea salt or sip beef or chicken bouillon broth with your dinner. The use of yellow mustard also helps (the small amount of quinine in yellow mustard stops the cramping). If you have congestive heart failure, talk to your doctor about monitoring your salt intake in balance with your diuretic or water pill.
Hypoglycemia – If you read the ketogenic diet research, most of it was done on epileptic children. The diets called for a period of starvation, then the use of a ketogenic liquid based on the John’s Hopkin’s protocol. It is a well-known fact in medicine that starvation in children can frequently cause hypoglycemia, especially in children with other genetic or congenital defects leading to forms of epilepsy. In clinical practice, with ketogenic diet use in adults, hypoglycemia is rare.
Low Platelet Count (Thrombocytopenia) – Again, this was seen in the epileptic children who were placed into starvation first, then introduced a liquid fat replacement shake to stop intractable seizures. These liquids or shakes were often nutrient deficient in other essentials. Folic acid, B12 and copper deficiency can occur when not eating “real food.” Low platelet counts are rarely seen on ketogenic diets based around “real food.” Many children in the ketogenic studies had been on or were concomitantly on valproic acid for their seizures. Valproic acid is commonly known to cause thrombocytopenia (Barry-Kravis E et al, Bruising and the ketogenic diet: evidence for diet-induced changes in platelet function. Ann Neurol. 2001 Jan;49(1):98-103.; Kraut E, Easy Bruising, http://www.uptodate.com, May 2015.)
Easy Bruising – This is usually due to inadequate protein supplementation as was the case in much of the ketogenic literature where protein levels were also restricted. (Kraut E, Easy Bruising, http://www.uptodate.com, May 2015.)
Pancreatitis – Patients who are insulin resistant or have impaired fasting glucose commonly have high triglycerides. Elevation in triglycerides itself is a cause of pancreatitis. Ketogenic diets lower the triglycerides. However, if a patient has not been following their diet as directed, spikes in the triglycerides can occur placing the person at risk for pancreatitis.
Long QT Intervals/Heart Arrhythmias – The list of things causing Long QT intervals and abnormal heart rhythms is long and variable (Acquired Long QT Syndrome. Berul C et al. www.uptodate.com, May 2015). It is well know that starvation, rapid weight loss and liquid protein diets can cause a delay in the conduction signal in the heart. Anyone wishing to start any diet should have an electrocardiogram (EKG) through their doctor to ensure that the diet (of any type) doesn’t exacerbate a prolonged QT interval.
Three year weight loss and metabolic improvement in a patient on a Low-Carb / Ketogenic diet. Note: Patient admits to not following ketogenic diet during holidays from Nov 2013 – Feb 2014 (see the dramatic changes to the body when cheating happens)
Cardiomyopathy – Prolonged QT intervals have been associated with cardiomyopathy and the former can stimulate the later. Any diet that has the potential to prolong a QT interval has the potential to cause cardiomyopathy. Hence the need for regular EKG monitoring on any diet (Acquired Long QT Syndrome. Berul C et al. www.uptodate.com, May 2015).
Lipid/Cholesterol Changes – In the 8 years I have been applying ketogenic diets to patients, I have seen dramatic improvement in the triglycerides and HDL levels. The only time triglycerides rise over 100 is if the patient is using artificial sweeteners or is cheating on the carbohydrate restriction. Total cholesterol commonly rises, however, this is indicative of the fact that there is a shift in the LDL particle size and this affects the calculation of both total cholesterol and LDL-C. In light of this, most of my patients have dramatic improvement in triglycerides and small dense LDL particle number. I’ve included the common cholesterol changes I seen in my office as a few case reports to demonstrate the effectiveness of a ketogenic diet:
2 year ketogenic dietary labs and weight loss
Myocardial Infarction – It is interesting that one blogger includes this on the list of adverse reactions, however, when you actually read the study, the author of the paper make an “assumption” that there was potential for heart attack due to an elevated total cholesterol, however, a correlation was never made. Again, in the 8 years I have been using ketogenic diets, I have seen dramatic improvement in cholesterol profiles, inflammatory markers, atherosclerosis and carotid intimal studies (Shai I et al, Circulation 2010; 121:1200-1208).
Three year metabolic history of a Low-Carbohydrate / Ketogenic diet
Menstrual Irregularities / Amenorrhea – It is well known that any diet causing protein or other nutritional deficiency will affect the menstrual cycle first and growth second. The only time menstrual irregularities occur with a ketogenic or Low-Carb diet is when a patient is not taking in enough protein or is not eating real food. What amazes me is that a properly applied ketogenic diet causes normalization of the menstrual cycle, and in my practice, I’ve had a number of women successfully be able to conceive after making a ketogenic dietary change.
For more details on the nutrient content of a ketogenic diet, see the recent article by a friend of mine, Maria Emmerich. She’s been creating ketogenic diets for years and has a number of fantastic books my wife and I have been using in our home over the last nine years. She is one among many that can give you some direction on how to devise a healthy, real food based ketogenic diet. See the page on my website here that will give you some direction in formulating your Ketogenic Lifestyle.
Nally Family Low-Carb / Ketogenic Cheese Cake
So, to celebrate Mother’s Day, today, with my family, I am going to indulge in some Low-Carb / Ketogenic Cheese Cake!! Happy Mother’s Day, to all of you and especially to all you mothers out there making a healthy difference in the lives of your families! (You can find the recipe for this delicious cheese cake here)
In the words of Sir William Ostler, “If it were not for the great variability among individuals, medicine might well be a science and not an art.”
Have you noticed that there are a large number of advertisements in the media about checking your testosterone or “Low T” Syndrome? It seems like this is the new advertising trend on the radio and late night TV.
Suddenly, everyone’s testosterone is low and men are complaining about their libido, . . . or are they?
Benefits of Testosterone Optimization. (Image Credit: ArtOfManliness.com)
If you practice medicine long enough, you’ll see a trend that seems to have arisen as our waistlines have expanded. About half of the men in my office with insulin resistance, pre-diabetes or diabetes have low testosterone levels. But this shouldn’t be a surprise. Type II diabetes, metabolic syndrome and insulin resistance are all driven by an over production in insulin in response to a carbohydrate load in the meal. Patients with these conditions produce between two to ten times the normal insulin in response to a starchy meal. A number of studies both in animal and human models demonstrate that insulin has a direct correlation on testosterone suppression in the blood. This has been demonstrated in both men and women. In fact, glucose intake has been shown to suppress testosterone and LH in healthy men by suppressing the gonadal hormone axis and more predominant testosterone suppression is seen in patient with insulin resistance or metabolic syndrome.
In fact, to put it simply, insulin increases the conversion (aromitization) of testosterone to estrogen in men (it does the opposite in women). Interestingly, Leptin resistance has a similar effect. I tend to see the worst lowering of testosterone in men with both insulin and leptin resistance.
How to you improve your testosterone? Supplemental testosterone has been shown to help, but it comes with some risks, including prostate enlargement and stimulating growth of prostate cancer. The most natural way to improve your testosterone is to change your diet.
A low carbohydrate or ketogenic diet turns down the insulin production and allows the testosterone to be available for use by the body. A ketogenic diet has the effect of reducing leptin resistance as well through weight loss. A simple dietary change of this type is frequently seen in my office to increase testosterone by 100-150 points.
KetoOS – Drinkable Exogenous Ketones
What is a ketogenic diet? It is a diet that restricts carbohydrates to less than 50 grams per day, thereby causing the body to use ketones as the primary fuel source. So, for breakfast tomorrow morning, hold the oatmeal (1/2 cup of Quaker Instant Oatmeal is 31 grams of carbohydrates) and have the bacon and eggs. And, rather than have the cheesecake for desert this evening, have an extra slice of steak butter on your rib-eye and hold the potato.
A few of my patients have come in struggling with their weight this week, following what they assumed to be a low carbohydrate diet. They were eating yogurt for breakfast, a chicken salad for lunch, and chicken and vegetables for dinner. A true low carbohydrate diet is ketogenic (it derives fuel from ketones) and is the byproduct of fatty acid metabolism. That means your fuel is coming from fat, not protein or carbohydrate. The presence of glucose, fructose, lactose or other sugars (or many sugar alcohols) shut fatty acid metabolism down and halt the process of weight loss and frequently increase weight gain. Too much protein does the same thing. A chicken salad is not ketogenic. It may be low carb, but without adequate fat, the absence of glucose drives the body to use protein as it’s primary fuel source. It is essential to maintain ketosis that a low carbohydrate diet moderate the protein and increase the fats to upwards of 60-70% of the total caloric intake.
Bacon is a 50/50 food. (I’m not talking about turkey bacon . . . that’s not real bacon). Each slice of real bacon is at a minimum 3 grams (50%) fat, and 3 grams (50%) protein. No carbs there, either.
So, if you’re struggling with your weight loss on a low carb diet . . . your first step should be “BLT” it!