Intent
The intent of this brief is to analyze the burden of obesity in the United States and to recommend policy changes to reduce the medical costs of obesity imposed upon the individual and country as a whole.
Introduction
Conventional fat reduction/caloric restriction guidelines for the treatment of obesity and associated cardiovascular disease, diabetes, cancer, and hypertension have been recommended since the early 1970’s. Because these guidelines are based on questionable evidence, the cost of obesity has dramatically risen to almost 21% of overall health care costs in the United States (1). This brief will analyze the current medical cost of obesity and will explain why the current obesity reduction guidelines perpetuate the problem. In addition, the brief will examine the impact of government agricultural policy on dietary habits, and will recommend changes to farm subsidy legislation in order to reduce the incidence of obesity and decrease costs to the healthcare system.
History & Background
The Cost of Obesity on the Nation
 As of 2012, obesity accounts for nearly 21% of overall health care costs in the United States. An obese person incurs $2741 more in medical expenses per year than his or her non-obese counterpart (1). Medicare spending has increased per person per year by $600 for each obese beneficiary (includes out-patient and prescription drugs) and Medicaid beneficiary prescription drug spending increased by $230 per year per obese person. Private insurance has increased by $248 for prescription drugs and $443 for in-patient services for each obese beneficiary per year (2). That adds up to $190.2 billion spent annually on obesity-related medical problems (3). This is a drastic change. Health care costs related to obesity were $85.7 billion (9.1% of overall health care costs) in 2006 and $61.2 billion (6.5% of overall health care costs) in 1998 (4).
As of 2012, obesity accounts for nearly 21% of overall health care costs in the United States. An obese person incurs $2741 more in medical expenses per year than his or her non-obese counterpart (1). Medicare spending has increased per person per year by $600 for each obese beneficiary (includes out-patient and prescription drugs) and Medicaid beneficiary prescription drug spending increased by $230 per year per obese person. Private insurance has increased by $248 for prescription drugs and $443 for in-patient services for each obese beneficiary per year (2). That adds up to $190.2 billion spent annually on obesity-related medical problems (3). This is a drastic change. Health care costs related to obesity were $85.7 billion (9.1% of overall health care costs) in 2006 and $61.2 billion (6.5% of overall health care costs) in 1998 (4).
 The most recent Center for Disease Control statistics reveal that 35.7% of the U.S. adult population is currently obese and another 33% is overweight. Over 78 million adults and 12.5 million children are obese (5). The addition of 30 million people to the health care roles (current estimation of the Affordable Care Act including Medicaid expansion) means that an estimated $27 billion (in 2012 dollars) more will be spent per year on obesity-related health care costs.
The most recent Center for Disease Control statistics reveal that 35.7% of the U.S. adult population is currently obese and another 33% is overweight. Over 78 million adults and 12.5 million children are obese (5). The addition of 30 million people to the health care roles (current estimation of the Affordable Care Act including Medicaid expansion) means that an estimated $27 billion (in 2012 dollars) more will be spent per year on obesity-related health care costs.
Impact of Government Policy on Consumption
The ‘Farm Bill’ was originally enacted as part of President Franklin D. Roosevelt’s Agricultural Adjustment Act of 1933, which provided subsidies to American farmers in the midst of the Great Depression. Since that time the federal government has paid farmers not to grow seven specific crops – known as commodities – with the intent of decreasing the supply, increasing the demand, and thereby raising the price (7). Dr. Susan Blumenthal, former Assistant Surgeon General and current SNAP to Health project director, writes, “The Farm Bill has since expanded to include many different categories or ‘titles.’ The last bill to be authorized, in 2008, had 15 titles, including nutrition (food stamps), crop subsidies, conservation, livestock, crop insurance and disaster assistance. The 2008 Farm Bill approved $300 billion in spending: 67% was spent on food stamps; 15% on agricultural subsidies; 9% on conservation; and 8% on crop insurance” (8).
The U.S. Department of Agriculture (USDA) Subsidy Programs tend to favor, either directly or indirectly, foods that increase obesity and other diseases. These subsidies support commodity crops, specialty crops, dairy products, livestock, and federal purchase programs. Their justification is that they help to stabilize prices in agricultural commodity markets by balancing supply and demand (9). Between 1995 and 2011, $277.3 billion were given in farm subsidies to almost 40% of U.S. farmers. Arizona received $1.1 billion (mainly for cotton); however, only 7% of Arizona farms received subsides during this period (10). These subsidies are incentives to grow and produce specific commodities that have a higher monetary return. Subsidies also act as a disincentive for farmers to grow fruits and vegetables which fall under the “specialty crops” category. This restricts both small and large farmers from diversifying their crops, and limits fruit and vegetable production (11).
Arizona farms received $25.3 million in dairy subsidies from 1995-2011 and $29.5 million in livestock subsidies during that same period (9). Arizona ranks 2nd nationally in its production of cantaloupe & honeydew melons, head & leaf lettuce, spinach, broccoli, cauliflower and lemons, all of which are “specialty crops” and do not receive subsidies (12). The most recent statistics show that the top five states receiving subsidies are Iowa, Texas, Illinois, Nebraska and Minnesota, with Kansas coming in at a close sixth. The majority of these subsidies are for corn ($81.7 billion), soybeans ($26.4 billion), rice ($13.3 billion) and wheat ($34.4 billion) from 1995-2011 (10). It is important to note that the Renewable Fuel Standard of 2012 (legislation protecting the corn-ethanol lobby) mandates that 37% of the corn harvest be used in ethanol production (13).
The food subsidies above have been in place since the Food, Conservation & Energy Act of 2002 and renewed in 2008. They were only to be available for a period of five additional years and were set to expire September 30, 2012. However, the American Taxpayer Relief Act of 2012 (H.R. 8), enacted by Congress and signed into law by President Barack Obama, included provisions that extended these subsidies until September 30, 2013 (20).
For many low-income Americans and especially children, federal programs have a direct and significant influence on food choices.  Over 30 million children receive government subsidized school lunch through National School Lunch Program (NSLP) administered by the USDA Food and Nutrition Service (14). USDA-purchased meats, dairy products, grains, fruits, and vegetables are supplied to schools for use in meal programs. Current school lunch recommendations on calorie intake set by the USDA and The Healthy, Hunger-Free Kids Act of 2010mandate school lunches provide 650-850 calories per meal to the 30 million children currently enrolled in this program (15). Interestingly, that is the same caloric count of a Big Mac®, small fry and Diet Coke® from McDonalds® (16). The rational for these purchase decisions are based upon agricultural support goals and adherence to national dietary guidelines (14). A study published in the journal Economics and Human Biology reveals that a person’s body mass index (BMI) increased faster if that personwere on food stamps, and the BMI increased at a faster rate while on the Supplemental Nutrition Assistance Program (SNAP). “We can’t prove that the Food Stamp Program causes weight gain, but this study suggests a strong linkage,” said Jay Zagorsky, co-author of the study and a research scientist at Ohio State University’s Center for Human Resource Research (17). However, much of the food available through the SNAP programs are refined, subsidized high-carbohydrate containing foods.
Over 30 million children receive government subsidized school lunch through National School Lunch Program (NSLP) administered by the USDA Food and Nutrition Service (14). USDA-purchased meats, dairy products, grains, fruits, and vegetables are supplied to schools for use in meal programs. Current school lunch recommendations on calorie intake set by the USDA and The Healthy, Hunger-Free Kids Act of 2010mandate school lunches provide 650-850 calories per meal to the 30 million children currently enrolled in this program (15). Interestingly, that is the same caloric count of a Big Mac®, small fry and Diet Coke® from McDonalds® (16). The rational for these purchase decisions are based upon agricultural support goals and adherence to national dietary guidelines (14). A study published in the journal Economics and Human Biology reveals that a person’s body mass index (BMI) increased faster if that personwere on food stamps, and the BMI increased at a faster rate while on the Supplemental Nutrition Assistance Program (SNAP). “We can’t prove that the Food Stamp Program causes weight gain, but this study suggests a strong linkage,” said Jay Zagorsky, co-author of the study and a research scientist at Ohio State University’s Center for Human Resource Research (17). However, much of the food available through the SNAP programs are refined, subsidized high-carbohydrate containing foods.
The price of food influences an individual’s consumption choices (6). Foods that are refined contain increased amounts of sugar or high-fructose corn syrup. These foods contain more caloric density and are often cheaper and more easily accessible. These are foods that are usually found in the center of the grocery store and frequently on sale at the end-caps of each isle. Nutrient-dense, higher fiber foods are frequently associated with higher prices and are consumed less often. These are the foods you usually find around the peripheral areas of the grocery store (fruits, vegetables, etc.) Current food subsidy policy found in the Food, Conservation and Energy Act of 2008 extension mandated by the American Taxpayer Relief Act of 2012 drives up the price of fruits, vegetables, and meats. This policy also turns people toward lower cost foods that are higher in simple carbohydrates and caloric density. Thus, current policy is actually making obesity worse and making America fatter. Research completed at the University of Illinois at Chicago reveals that small taxes or price changes do not produce a change in a person’s BMI; however, more significant price change has a measurable and significant effect on weight in both adults and children. Price increases of 100-150% have been shown to change purchasing behavior and thereby affect health (18). An example of this is the tax levied on cigarette smoking.
The USDA disagrees with the amount of influence they have over the individual American’s food choices. They state openly on their website that “Some public health advocates have argued that falling real, or inflation-adjusted, prices for many high-calorie foods encourage people to buy and consume more of these foods, leading to poor diet quality and rising rates of obesity. A closer look at how consumers respond to food price variation–over time, across geographic markets, in different types of stores, and in response to taxes and subsidies–reveals how food prices affect people’s food choices, and their waistlines. In short, price matters, but not very much, and it is not the only factor” (19).
Why Current Dietary Guidelines Have Not Been Effective
Why do we get fat? Why have we not been successful in losing weight via diet and exercise? The obesity paradox was described by Jules Hirsch of Rockefeller University, who proposed two opposing hypotheses:
- “Obesity is the result of a willful descent into self-gratification” implying that we gain weight because we over-eat (caloric excess) leading to caloric imbalance.
- “Alternative hypothesis is that there is something ‘biologic’ about obesity, some alteration of hormones, enzymes or other biochemical control systems which leads to obesity” (22).
The 1977 Dietary Goals for the United States – the first comprehensive statement by any branch of the federal government about the American diet – supported the first theory. The Guidelines were heavily influenced by the American Heart Association’s position that fat intake alone would cause heart disease. The USDA 2011 Dietary Guidelines imply that the “people who are the most successful at achieving and maintaining a healthy weight do so through continued attention to consuming only enough calories from foods and beverages to meet their needs and by being physically active.” (15)
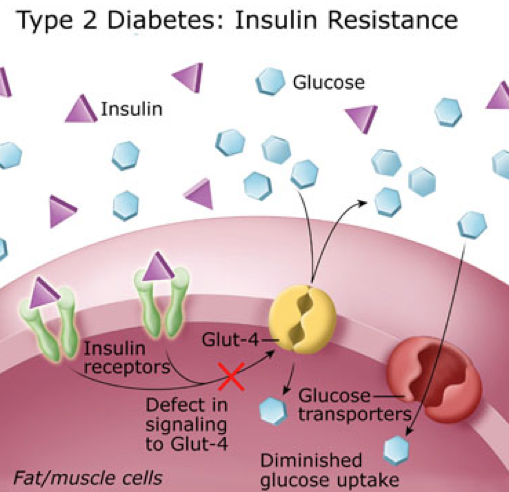
Current research contradicts the caloric restriction or “calorie in – calorie out” theory. Scientific evidence clearly demonstrates the domino effect of carbohydrate or starch intake increasing insulin levels which thereby stimulates obesity by raising cholesterol and triglyceride levels. Time Magazine recently published evidence that the longstanding recommendations to “eat less high-fat red meat, eggs and dairy and replace them with more calories from fruits, vegetables and especially carbohydrates” is now seen as incorrect (45). Even our medical textbooks from 1965, like the introductory chapter of the Handbook of Physiology, make it clear that carbohydrate intake cause weight gain and raise triglyceride and cholesterol levels (22), (23), (24).
Current Policy
The current version of the Farm Bill was set to expire September 30th, 2013. If it had been allowed to expire, the results would have returned us to the 1949 Farm Bill legislation and theoretically double the price of milk. However, this would have had the effect of freeing up over $5 billion dollars of federal spending per year and would also lead to decreased consumption of a major source of carbohydrates in the standard American diet like wheat and corn. Senator Debbie Stabenow (D-MI), and chairwoman of the Senate Agriculture Committee, had repeatedly said she was opposed to an extension; however, she agreed to a compromise extending the bill for another year to help the farmers experiencing serious drought conditions in 2012 (7). Two additional extensions were passed in the House and Senate, but because these differed so significantly, it was referred to a House-Senate Conference Committee to work out the compromise details. With only $23 billion in spending reductions, The Agricultural Act of 2014 was passed on January 29, 2014 (46).
Outcomes and Stakeholders
 If the United States continues its current course, up to 58% of the population will be obese by 2030 (26). Many believe that the USDA Dietary Guidelines are to blame. Richard David Feinman, President of the Nutrition and Metabolism Society and Professor of Cell Biology at SUNY Downstate Medical Center said, “The previous Guidelines have not worked well. It is unreasonable to ask the Dietary Guidelines Advisory Committee (DGAC) to audit its own work. An external panel of scientists with no direct ties to nutritional policy would be able to do a more impartial evaluation of the data. This would be far better for everyone.” (27) A recent Gallup Poll reveals that 63% of Americans believe the USDA Guidelines that a low fat, calorie restricted diet will help in reduction of obesity, and the same study showed that 48% of Americans worry about their weight “all of the time or some of the time” (28). Recent evidence from the Women’s Health Initiative Dietary Modification Trial studying 49,000 women supports Dr. Feinman’s conclusion above. It did not show any statistically significant evidence that following a low-fat or caloric restricted diet had any effect upon obesity (29). Other nutritional experts from the Salt Institute and the National Health Coalition have expressed their support for significant changes to the USDA Dietary Guidelines (30). The Weston A. Price Foundation, which according to its website is “dedicated to restoring nutrient-dense foods to the human diet through education, research and activism,” also supports the view that the current USDA Dietary Guidelines have been a significant cause of obesity and have been an active voice promoting legislative change (31).
If the United States continues its current course, up to 58% of the population will be obese by 2030 (26). Many believe that the USDA Dietary Guidelines are to blame. Richard David Feinman, President of the Nutrition and Metabolism Society and Professor of Cell Biology at SUNY Downstate Medical Center said, “The previous Guidelines have not worked well. It is unreasonable to ask the Dietary Guidelines Advisory Committee (DGAC) to audit its own work. An external panel of scientists with no direct ties to nutritional policy would be able to do a more impartial evaluation of the data. This would be far better for everyone.” (27) A recent Gallup Poll reveals that 63% of Americans believe the USDA Guidelines that a low fat, calorie restricted diet will help in reduction of obesity, and the same study showed that 48% of Americans worry about their weight “all of the time or some of the time” (28). Recent evidence from the Women’s Health Initiative Dietary Modification Trial studying 49,000 women supports Dr. Feinman’s conclusion above. It did not show any statistically significant evidence that following a low-fat or caloric restricted diet had any effect upon obesity (29). Other nutritional experts from the Salt Institute and the National Health Coalition have expressed their support for significant changes to the USDA Dietary Guidelines (30). The Weston A. Price Foundation, which according to its website is “dedicated to restoring nutrient-dense foods to the human diet through education, research and activism,” also supports the view that the current USDA Dietary Guidelines have been a significant cause of obesity and have been an active voice promoting legislative change (31).
On the other hand, the Sugar Association has issued statements that sugar is not the cause of obesity and “continually eating too much food and sedentary lifestyles are the major contributing factors to increasing rates of obesity – not sugar intake” (32). In addition, the American Beverage Association has stated that sugars are not the problem with obesity, but instead, “overweight and obesity are a result of an imbalance between calories consumed and calories burned” (33).
Attempts at modifying the Farm Bill with legislation like the 2012 DeMint Amendment (SA 2276 ) were supported by both Arizona Senators McCain (R-AZ) and Kyl (R-AZ) with a “Yes” vote, as well as Senators Ayotte (R-NH), Brown (R-MA), Burr (R-NC), Coats (R-IN), Coburn (ROK), Cornyn (R-TX), DeMint (R-SC), Graham (R-SC), Hatch (R-UT), Heller (R-NV), Johnson (R-WI), Lee (R-UT), McConnell (R-KY), Murkowski (R-AK), Paul (R-KY), Rubio (R-FL), Sessions (R-AL), and Toomey (R-PA). However, because of a large lobbying agricultural coalition, it was voted down (34). Changing farm subsidies will be a great challenge as 40% of the farmers in the U.S. now have some degree of dependence upon these subsidies. The following agricultural groups have historically had significant monetary interest in the farm subsidies that these amendments would affect:
- American Beekeeping Federation
- American Farm Bureau Federation American Mushroom Institute
- American Sheep Industry Association American Soybean Association
- National Cattlemen’s Beef Association National Corn Growers Association National Cotton Council
- National Council of Farmer Cooperatives National Farmers Union
- National Milk Producers Federation National Pork Producers Council
- National Potato Council
- National Sorghum Producers
- National Watermelon Association
- Produce Marketing Association
- United Dairymen of Arizona
- United Egg Producers
- United Fresh Produce Association
- Western Peanut Growers Association
The following groups have formed coalitions in support of the Farm Bill: Health/Food Justice/Farm Group partnerships, Specialty Crop Farm Bill Alliance, Community Food Security Coalition, Center for a Livable Future at Johns Hopkins University, Collaboration for a Healthy Sustainable Food System, and the Healthy Farms, Healthy People: A Farm & Food Policy Summit for a Strong America.
The American Heart Association’s position is that the Farm Bill needs to be modified to include increased access to fruits and vegetables (35). The American Medical Association’s position in 2008 and 2011 has been for cutting the size and budget of the current Farm Bill (36). The American Osteopathic Association does not currently have a formal position on the Farm Bill.
If certain crops like corn or wheat were no longer subsidized,drastic changes will be likely in the food manufacturing industry, which would likely be the largest proponent against change. Unintended consequences of modifying the Farm Bill and not extending its subsidies could have the short term effect of escalating the price of a number of commodities to two to three times their current price. For example, the price of milk would increase to $6-$8 dollars a gallon without federal subsidies (37). This would likely deter the use of carbohydrates containing dairy products, but may also increase the price of meats and cheeses as well.
The USDA’s Rural Development Progress Report claims that the subsidies it distributed “saved more than 75,000 jobs” in 2006 and over 400,000 jobs in 2011 (38), (39). They claim that without federal farm subsidiesthere would be significant loss of jobs; however, studies from the Cato Institute actually show the opposite.
“Job gains are weak and population growth is actually negative in most of the counties where farm payments are the biggest share of income. Job growth is decidedly weak in the counties most dependent on farm payments. The vast majority of such counties (483) had job gains below the 19 percent national average from 1992 to 2002. A considerable number (167) had outright job losses over the period. In short, farm payments are not yielding robust economic and population gains in the counties where they should have the greatest impact. If anything, the payments appear to be linked with sub-par economic and population growth. To be sure, this quick comparison cannot answer whether growth would have been even weaker in the absence of the payments. Still, farm payments appear to create dependency on even more payments, not new engines of growth” (40).
As of 2010, obesity costs about $73.1 billion per year in lost productivity in the United States (43). The worsening obesity epidemic poses further workforce productivity losses up to 20% more by 2030. Even small improvements in obesity will improve workforce productivity and has substantial potential for savings. Currently, the Affordable Care Act allows employers to charge obese employees 30-50% more for health insurance. Without correcting this epidemic, it may be impossible for many to afford health care, opting out to pay the less expensive tax penalty. This would have the effect of increasing commercial premiums across the country, feasibly pushing private insurance companies out of business and forcing a single payer governmental system.
Recommendations
This brief points out that the overall U.S. healthcare costs associated with obesity have increased by 68% in the last fourteen years. It provides evidence that using current dietary low-fat caloric restriction guidelines show poor statistically significant improvements in obesity. And it provides evidence that obesity is not caused by excessive caloric intake and fat, but by insulin response to carbohydrate intake. Lastly, this analysis provides evidence that the Farm Bill propagates continued worsening obesity rates in the US by providing access to cheap, fattening food.
The USDA 2011 Dietary Guidelines need to be revised to reflect current evidence-based obesity prevention and weight reduction research. The guidelines should include information about limiting the intake of foods high in carbohydrates.
The food subsidy extension provided in the American Taxpayer Relief Act of 2012 was extended five years by the Agricultural Act of 2014. Had it been allowed to expire, it would have saved the country over $200 billion over the next ten years. However, because of so many entitlements involved in this bill, the House and Senate convened in Conference that resulted in a compromise of only $23 billion dollars in spending reductions, the first SNAP reforms since 1996 reducing waste, but did nothing in eliminating subsidies that drive or influence eating behavior (46).
When significant price changes occur, eating behavior will change. As the price of fattening carbohydrates increases, people will eat less of them, leading to a national decrease in obesity and overweight. The current reforms did nothing that will change our dietary behavior.
References
1. Cornell University. Obesity accounts for 21 percent of U.S. health care costs, study finds. Science Daily. [Online] April 9, 2012. [Cited: January 5, 2013.] http://www.sciencedaily.com/releases/2012/04/120409103247.htm.
2. Annual Medical Spending Attributable To Obesity: Payer-And Service-Specific Estimates. Eric A Finkelstein, Justin G Trogdon, Joel W Cohen and William Dietz. Health Affairs, 28, Bethesda, MD : Project HOPE, 2009, Vol. 5. 10.1377/hlthaff.28.5.w822.
3. Begley, Sharon. As America’s Waistline Expands, Costs Soar. Reuters. [Online] Thompson Reuters, April 30, 2012. [Cited: January 5, 2013.] http://www.reuters.com/article/2012/04/30/us-obesity-idUSBRE83T0C820120430.
4. Ungar, Rick. Obesity Now Cost Americans More In Healthcare Spending Than Smoking. Forbes. [Online] 4 30, 2012. [Cited: January 5, 2013.] http://www.forbes.com/sites/rickungar/2012/04/30/obesity-now-costs-americans-more-in-healthcare-costs-than-smoking/.
5. Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesity in the United States, 2009–2010. NCHS data brief, no 82. Hyattsville, MD : National Center for Health Statistics, 2012, 2012.
6. Poverty and Obesity: The Role of Energy Density and Energy Costs. A Drewnowski, SE Specter. s.l. : American Journal of Clinical Nutrition, 2004, Vols. 79:6-16.
7. Laprete, Jay. U.S. Farm Bill. Times Topics. [Online] The New York Times, December 31, 2012. [Cited: February 11, 2013.] http://topics.nytimes.com/top/reference/timestopics/subjects/f/farm_bill_us/index.html?offset=0&s=newest.
8. SNAP to Health. U.S. Farm Bill: Frequently Asked Questions. SNAP to Health. [Online] CSPC / Snap to Health, 2013. [Cited: February 11, 2013.] http://www.snaptohealth.org/farm-bill-usda/u-s-farm-bill-faq/.
9. USDA. Agricultural Marketing Service. Commodity Purchasing. [Online] January 22, 2013. [Cited: February 10, 2013.] http://www.ams.usda.gov/AMSv1.0/ams.fetchTemplateData.do?template=TemplateQ&navID=Commodity%20Purchasing%20Main%20Page&rightNav1=Commodity%20Purchasing%20Main%20Page&topNav=&leftNav=CommodityPurchasing&page=CommodityPurchasing&resultType=&acct=cmdtyprchs.
10. Environmental Working Group. United States Summary Information. EWG Farm Subsidies. [Online] 2012. [Cited: February 10, 2013.] http://farm.ewg.org/region.php?fips=00000.
11. Monke, Jim. Farm Commodity Programs: Base Acreage and Planting Flexibility. Washington, DC : Congressional Research Services, 2003.
12. Arizona Farm Bureau Federation. AG Facts. Arizona Farm Bureau. [Online] 2013. [Cited: February 15, 2013.] http://www.azfb.com/ag-facts.html.
13. Children of the Corn: The Renewable Fuels Disaster. The American. [Online] American Enterprise Institute, January 4, 2012. [Cited: February 15, 2013.] http://www.american.com/archive/2012/january/children-of-the-corn-the-renewable-fuels-disaster.
14. USDA Food & Nutrition Service. National School Lunch Program. USDA Food & Nutrition Serivce. [Online] June 21, 2012. [Cited: February 15, 2013.] http://www.fns.usda.gov/cnd/lunch/.
15. U.S. Department of Agriculture (USDA). USDA 2010 Dietary Guidelines. USDA Center for Nutrition Policy and Promotion: Dietary Guidelines for Americans. [Online] U.S. Government Printing Office, January 31, 2011. [Cited: January 5, 2013.] http://www.cnpp.usda.gov/Publications/DietaryGuidelines/2010/PolicyDoc/Chapter2.pdf.
16. ABC News. ABC News. Medical Unit. [Online] ABC News Internet Ventures, September 30, 2012. [Cited: April 14, 2013.] http://abcnews.go.com/blogs/health/2012/09/30/school-lunch-showdown-850-calorie-meals-compared/.
17. Ohio State University. Food Stamp Use Linked To Weight Gain, Study Finds. Science Daily. [Online] August 12, 2009. [Cited: April 13, 2013.] http://www.sciencedaily.com /releases/2009/08/090810122139.htm.
18. Food Prices and Obesity: Evidence and Policy Implications for Taxes and Subsidies. L Powell, F Chalupka. 1, Illinois : The Milbank Quarterly by Wiley Periodicals Inc, 2009, Vol. 87.
19. Jessica Todd, Biing-Hwan Lin. Amber Waves Online Magazine. U. S. Department of Agriculture Economic Research Service. [Online] September 2012. [Cited: February 10, 2013.] http://www.ers.usda.gov/amber-waves/2012-september/what-role-do-food-and-beverage-prices.aspx.
20. American Taxpayer Relief Act of 2012. U.S. Government Printing Office. [Online] Jan 12, 2012. [Cited: February 10, 2013.] http://www.gpo.gov/fdsys/pkg/BILLS-112hr8enr/pdf/BILLS-112hr8enr.pdf.
21. Bruch, Hilde. The Importance of Overweight. Michigan : Norton, University of Michigan, 1957.
22. Taubs, Gary. Good Calories, Bad Calories: Fats, Carbs, and the Controversial Science of Diet and Health. New York : Anchor Books, 2007. 978-1-40000-3346-1.
23. Role of Insulin in Endgenous Hypertriglyceridemia. GM Reave, RL Lerner, MP Stern, JW Farquhar. s.l. : Journal of Clinical Investigation, 1967, Vols. 46(II):1756-67.
24. High-Carb Diets Questioned. Kolata, G. 235(4785):164, s.l. : Science, 1987, Vol. 9.
25. U.S. Department of Health and Human Services. The Surgeon General’s Call to Action to Prevent and Decrease Overweight and Obesity. Washington, D.C. : U.S. Government Printing Office, 2001.
26. Global Burden of Obesity in 2005 and Projections to 2030. T Kelly, W Yang, C-S Chen, K Reynolds and J He. 8 July 2008, New Orleans : International Journal of Obesity, 2008, Vols. 32, 1431–1437. doi:10.1038/ijo.2008.102.
27. In The Face Of Contradictory Evidence: Report Of The Dietary Guidelines For Americans Committee. Adele H Hite, Richard D Feinman, Gabriel E Guzman, Morton Satin, Pamela Schoenfeld, Richard J Wood. 10, s.l. : Nutrition, 2010, Vol. 26. DOI: 10.1016/j.nut.2010.08.012.
28. A Dugan, F Newport. Gallup Wellbeing. Gallup. [Online] August 17, 2012. [Cited: April 13, 2013.] http://www.gallup.com/poll/156710/americans-say-low-fat-diet-better-low-car.aspx.
29. Low-fat dietary pattern and weight change over 7 years: the Women’s Health Initiative Dietary Modification Trial. . Howard BV, Manson JE, Stefanick ML, et al. s.l. : JAMA, 2006, Vols. 295:39-49. doi:10.1001/jama.295.1.39.
30. Healthy Nation Coalition. Healthy Nation Coalition. Healthy Nation Coalition. [Online] Adrienne Larocque, PhD, 2012. [Cited: March 8, 2013.] http://www.forahealthynation.org/.
31. Judith McGeary, Esq. Legislative Updates. The Weston A. Price Foundation. [Online] December 11, 2012. [Cited: March 9, 2013.] http://www.westonaprice.org/legislative-updates/policy-update-farm-bill-and-gmos.
32. The Sugar Association. Sugar and Your Diet. Sugar.org. [Online] 2012. [Cited: March 9, 2013.] http://www.sugar.org/sugar-and-your-diet/caloric-intake.html.
33. American Beverage Association. Obesity. American Beverage Association. [Online] 2013. [Cited: March 9, 2013.] http://www.ameribev.org/nutrition–science/obesity/.
34. Library of Congress. S.Amdt.2276 to S.3240. Congress.Gov. [Online] March 8, 2013. [Cited: March 9, 2013.] http://beta.congress.gov/amendment/112th-congress/senate-amendment/2276.
35. The American Heart Association. Policy Brief – The Farm Bill. The American Heart Association. [Online] 2012. [Cited: April 14, 2013.] http://www.heart.org/idc/groups/heart-public/@wcm/@adv/documents/downloadable/ucm_429110.pdf.
36. AMA: Report of Reference Committee . Malechek, Lindsay. 2011.
37. Wolf, Jim. Senate, House agriculture committees in deal to avert milk price spike. Reuters. Sun, Dec 30, 2012, 2012.
38. USDA. USDA Rural Progress Report. USDA. [Online] December 2006. [Cited: April 14, 2013.] http://www.rurdev.usda.gov/rd/pubs/2005_06_Prog_Report.pdf.
39. —. USDA Rural Developement 2011 Progress Report. USDA Rural Developement. [Online] December 2011. [Cited: April 14, 2013.] http://www.rurdev.usda.gov/Reports/RD%20Progress%20Report%202011–Smallest(2).pdf.
40. Slivinski, Stephen. Rural Subsidies. Cato Institute. [Online] July 2009. [Cited: March 9, 2013.] http://www.downsizinggovernment.org/agriculture/rural-subsidies.
41. Obesity prevention: the role of policies, laws and regulations. Swinburn, Boyd A. New Zeland : BioMed Central Ltd., 208, Vol. 5:12. 10.1186/1743-8462-5-12.
42. Begley, Sharon. As America’ss Waistline Expands, Costs Soar. Reuters. [Online] Thompson Reuters, April 30, 2012. [Cited: January 5, 2013.] http://www.reuters.com/article/2012/04/30/us-obesity-idUSBRE83T0C820120430.
43. The Costs of Obesity in the Workplace. E Finkelstein, M DiBonaventura, S Burgess, B Hale. 10, Illinois : Lippincott Williams & Wilkins, 2010, Vol. 52. doi: 10.1097/JOM.0b013e3181f274d2.
44. Rudd Center For Food Policy & Obesity. Search Legislation Database. Yale Rudd Center. [Online] Rudd Center, 2013. [Cited: January 5, 2013.] http://www.yaleruddcenter.org/legislation/search.aspx.
45. Walsh, Bryan. “Ending The War on Fat.” TIME Magazine. June 12, 2014.
46. Lucas, Frank D. “Agricultural Act Summary.” House Agricultural Committee. [Online] Jan 29, 2014. [Cited June 28, 2014.] http:// http://agriculture.house.gov/farmbill



























 On the contrary, you owe the world something. You owe it your time, talent and energy so that no one will be at war, in sickness and in loneliness as we have been in the past. In other words, grow up, stop being a crybaby, get out of your dream world and develop a backbone and not a wishbone. Motivation is a fire from within. If someone else tries to light that fire under you, chances are, it will only burn very briefly. Start behaving like a responsible person. You are important and you are needed. It’s too late to sit around and wait for somebody to do something someday. Someday is now, and that somebody is you.
On the contrary, you owe the world something. You owe it your time, talent and energy so that no one will be at war, in sickness and in loneliness as we have been in the past. In other words, grow up, stop being a crybaby, get out of your dream world and develop a backbone and not a wishbone. Motivation is a fire from within. If someone else tries to light that fire under you, chances are, it will only burn very briefly. Start behaving like a responsible person. You are important and you are needed. It’s too late to sit around and wait for somebody to do something someday. Someday is now, and that somebody is you.

 ulated by drinking them.
ulated by drinking them.




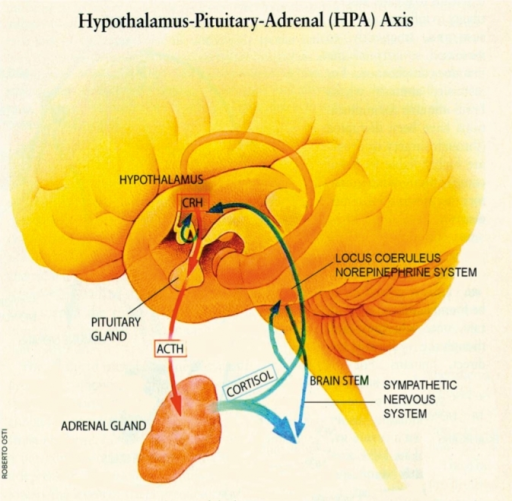 People with significant stressors in their life have been show to have a raised cortisol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing an over production of cortisol and normalization of their cortisol levels occurs after resolution of the stressor. This cortisol response is not high enough to lead to a true
People with significant stressors in their life have been show to have a raised cortisol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing an over production of cortisol and normalization of their cortisol levels occurs after resolution of the stressor. This cortisol response is not high enough to lead to a true 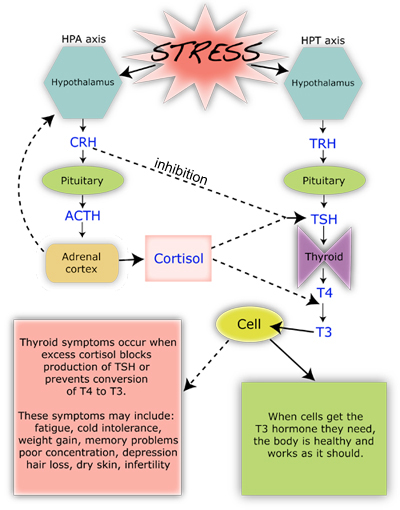 Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues and turns on the maturation process of adipocytes (fat cells). In the process, it suppresses the immune system to decrease inflammation during times of stress (7,8,9). In the short run, this is an important process, however, when cortisol production is chronically turned up, it leads to abnormal deposition of fat, increased risk of infection, impotence, abnormal blood sugars, head
Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues and turns on the maturation process of adipocytes (fat cells). In the process, it suppresses the immune system to decrease inflammation during times of stress (7,8,9). In the short run, this is an important process, however, when cortisol production is chronically turned up, it leads to abnormal deposition of fat, increased risk of infection, impotence, abnormal blood sugars, head




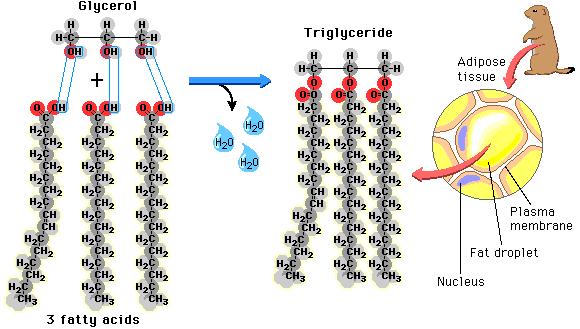 as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
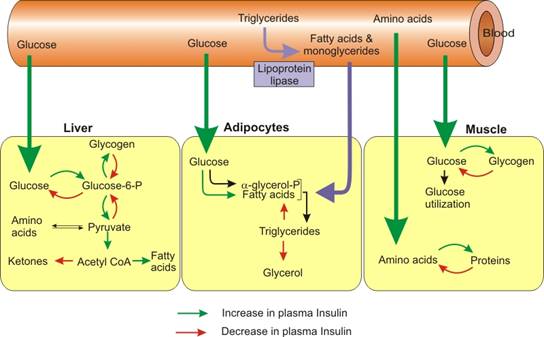 before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).
before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).