

In the last two decades, it has become more and more clear that the average American has trouble facing reality. The average American has trouble facing truth. It affects each of us, and it is affecting physicians, nurses and health professionals individually.
At least once a week, one of my patient’s refuses to get on the scale. Why would you visit the doctor to improve your health, and yet refuse to look at a measure of health? Yet, that is the accepted culture of today.
Language of Euphemism
Another evidence of this can be seen in the changes to our language. Our language has become flowered with euphemism and politically correct phrases. It is why we have a whole generation hyper-focused on “cancel culture.” People have set aside their faith to live by their feelings. People no longer accept another’s right to share their perspective or express themselves, especially if it hurts another’s feelings. We’ve created soft language that has taken the life out of life and medicine.
Shell Shock to PTSD
An example of this change is the softening of language describing what happens to a persons nervous system when in combat. During World War I from 1914 to 1918, if a soldier’s nervous system became overwhelmed due to the fatigue, stress and horror of battle it was called “shell shock.” The term describes the power and struggle that occurs with this overwhelming stress. The word almost echos the rattle of a cannon on one’s soul. Men would return home with hysteria, muscle contractions, heart palpitations, dizziness, depression, blindness, paralysis, insomnia, loss of appetite, flashbacks, nightmares or unable to speak without any physical damage to explain the symptoms. Because little was understood about the cause, it was seen as a sign of emotional weakness. Many were even branded as deserters or cowards because of the condition shell shock would cause. At the end of the war, 80,000 men were diagnosed with shell shock in the British Army medical facilities.
But instead of addressing the pain and addressing the trauma, we buried it under the jargon and euphemisms. After the second world war in 1945, we toned the term down because we didn’t want to hurt anyone’s feelings describing them as “shell shocked.” So, we called it “Battle Fatigue.” It is the same problem, overwhelming a person’s emotional coping mechanisms and nervous system with stress to the point of failure, but “battle fatigue” just sounded better, and softer.
Enter the Korean War of 1950-1951. Actually, we softened that too. It wasn’t really a war, we were told, and our leaders turned it from war into a softer more acceptable “Korean Conflict.” Men and women who encountered the same overpowering effects on the nervous system from witnessing the horror of battle, death and destruction were told they had “operational exhaustion.” This was an even softer term that allowed for a further avoidance of the truth.
Five years later, the U.S. entered a 19 year “conflict” with Vietnam. The politicians of the time didn’t want to call it war either. The same trauma causing shell shock in World War I was experienced by men and women in Vietnam. Seeing the horrors of battle on a daily basis and only being allowed to police those attacking you with guerrilla warfare in a foreign country led to severe trauma in many of our soldiers. Fighting was intense and millions of people were killed including 60,000 U.S. soldiers. Yet, we further softened the term “operational exhaustion” with the same symptoms of shell shock to “Post-traumatic Stress Syndrome (PTSD).” (Hey, at least they added a hyphen, right?)
Waking The Tiger – Working Through Trauma
Trauma is trauma, no matter how or where you experience it. Because of it’s complexities, the treatment of trauma can’t be addressed here, but according to Peter Levine in his book Waking the Tiger, trauma, no matter what the cause, must be worked through. Peter Levine does a wonderful job in explaining this in his second follow up book In An Unspoken Voice. There are additional treatments for burnout. The brain has a consistent pattern that it follows to resolve trauma and burnout. If that pattern is disrupted, shell shock, battle fatigue, operational exhaustion or PTSD ensues.
Elizabeth Metraux describes this in her 2018 article this way:
“I was on my honeymoon in Colombia when I first became aware of the true extent of my post-traumatic stress disorder. My husband and I were walking across a smooth, granite platform to take a closer look at a fountain in downtown Cartagena. As we neared the structure, mist from the fountain’s jets dampened the ground at my feet.
“I froze, paralyzed with fear by a flashback — my first — triggered by something as ordinary as wet pavement on a warm day.
“Two years earlier, I was working in civic engagement efforts in Baghdad. One morning, as I walked across a smooth, granite platform toward my apartment, gunfire erupted. I tried to run, but my flip-flops bested me on the pavement, still damp from an early mopping. I slipped and fell backward, hitting my head hard enough to knock me out. When I opened my eyes minutes later, the platform was covered with my blood.
“That happened 15 years ago this week, those Ides of March when American forces invaded Iraq.
“Back home in the U.S., it was clear to those around me that I had PTSD. It wasn’t until six months after my honeymoon, however, that I had the courage to acknowledge that I needed help. It’s not easy seeing your own weaknesses, much less conceding them. But when my habitual glass of wine with dinner became a bottle, and fireworks left me sore and sleepless for days, it was hard to fight the signs.
“Celexa for guilt. Ambien for sleep. Therapy for months. My psychologist and primary care physician spoke regularly to coordinate my care. Most importantly, family and friends became members of my care team. Isolation is a trauma victim’s ill-advised drug of choice, one my loved ones and clinicians wouldn’t let me take.”
Most Physicians Suffer from Moral Trauma combined with PTSD
What concerns me is that many of today’s heath-care workers, physicians and nurses, suffer from PTSD and moral trauma. Dr. Metraux goes on to describe a conversation she has that is reminiscent of many recent conversations I’ve had with my colleagues:
“A few weeks ago, I was talking with a physician who served our country in Iraq. We chatted nostalgically about the taste of sand and shawarma before he said something that gave me pause: ‘You know, I’d go back to the field any day. Beats practicing in my clinic.’
“‘Why’s that?’ I asked.
“’I didn’t become a doc to put up with billing codes and power struggles. I thought that PTSD would hit when I came home from Fallujah. It’s so much worse when I come home from the office. Truth is, I’ve lost my sense of purpose.’”
Physician burnout is easily chalked up to the 4-8 minute hurried visit with 30-40 patients per day, and the additional 6-8 hours spent each day entering patient information into an electronic medical record, combined with the life-and-death decisions this profession requires routinely every day. Add to it a time when a physicians and nurses are called upon to be the only people in the clinics and hospitals taking care of a viral infection still unknown in its full spectrum. But, that doesn’t even scratch the surface.
Thousands of Tiny Betrayals of Purpose
The real cause of injury is the fear created by a society that doesn’t really want to hear or face the truth, and the hundreds and thousands of tiny betrayals of purpose that occur every day in the clinic or the hospital. Most physicians find themselves expressing horror and disgust at how far they’ve been steered away from their primary purpose of taking care of people. Clinicians and nurses, much like combat veterans, are forced to take actions every day that contradict their core purpose – sometimes compulsory, sometimes voluntary. It causes a slow imperceptible unwinding of character.
The 4-8 minute visit means the physician can’t take time to build a real relationship with you or take care of the whole person whose real diagnosis can’t be logged into a computer. The 8 hours of daily charting requires the clinicians eyes to be taken off their patients, missing the humanity that brought us to the work in the first place. The government mandated “quality metrics” imposed on every patient encounter by Medicare, Medicaid and intrusive insurance plans that crowds out the deeper connection with patients to help them manage triggers, feel truly cared for and navigate treatments. Each of these are a “tiny betrayals of purpose,” 30-40 times a day over the course of weeks and months and years. When you subconsciously betray yourself with every interaction you have throughout the day, it adds up.
Medicine now requires clinicians to practice in a manner inconsistent with their values, because it saves costs, increases access and improves quality, . . . maybe. Then, add a new virus with an unknown morbidity, mortality and infectivity to the spectrum without a clear treatment protocol. Then add to that layers of bureaucratic regulation and mandates around treatment and insurance.
In 20 years of medical practice, including battlefield medicine, I’ve never seen physicians express public fear, angst and fatigue in the course of their duty. I’ve seen it every day in the last year.
We Lose a Physician Every Day
Since 2018, over 400 physicians committed suicide per year. Every day, at least one physician commits suicide (Tanwar D, Amer Psych Asso 2018 Annual Meeting). That is the highest rate of suicide in any profession. 40 suicides per 100,000 is twice that of the general population. This rate is higher than the military. The claim is that doctors are under-treated or untreated for their depression. It is more than that. Doctors and nurses alike are experiencing “shell shock,” or in today’s vernacular, “post-traumatic stress disorder” and being force to live, work and function all while suffering with subconscious moral injury. It goes untreated and unrecognized.
It’s why your doctor is curt with you. It’s why he or she can only spend five minutes with you in the exam room. It’s why you get the sense of fear from them when dealing with COVID-19. It’s why there is confusion about wearing masks and why so many physicians struggle to keep up with the ever changing science. It’s why 30% of them are divorced. It’s why 73% of the physicians and 50% of nurses you meet are effected by burnout, trauma and PTSD.
The challenge, is it’s only going to get worse before it gets better. Some will leave medicine, some will leave life. Others will suffer until it kills them. Unless, you and I change it. Until then, society will be offended.


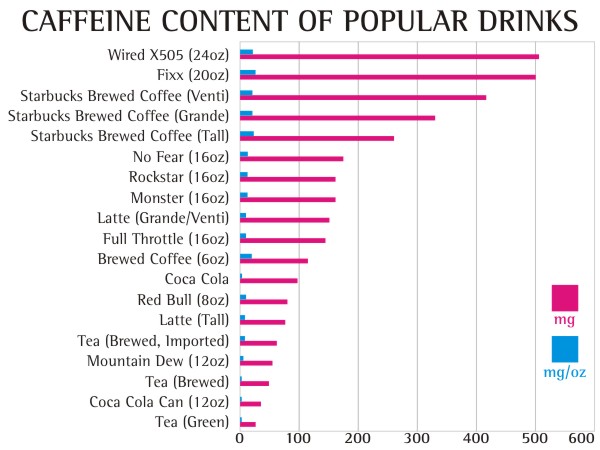
 After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the
After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the 


 People with significant stressors in their life have been show to have an increased corsiol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing a daily, cyclic over production of cortisol and then normalization of cortisol after resolution of the stressor. This cortisol response is not high enough to lead to a true
People with significant stressors in their life have been show to have an increased corsiol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing a daily, cyclic over production of cortisol and then normalization of cortisol after resolution of the stressor. This cortisol response is not high enough to lead to a true  Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids or proteins into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues (by stimulating insulin production) and turns on the maturation process of adipocytes (it makes your fat cells age – nothing like having old fat cells, right?!) In the process, cortisol suppresses the immune system through an inhibitory effect designed to decrease inflammation during times of stress (7,8,9). If this was only occurring once in a while, this cascade of hormones acts as an important process. However, when cortisol production is chronically turned up, it leads to abnormal deposition of fat (weight gain), increased risk of infection, impotence, abnormal blood sugars, brain fog, head
Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids or proteins into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues (by stimulating insulin production) and turns on the maturation process of adipocytes (it makes your fat cells age – nothing like having old fat cells, right?!) In the process, cortisol suppresses the immune system through an inhibitory effect designed to decrease inflammation during times of stress (7,8,9). If this was only occurring once in a while, this cascade of hormones acts as an important process. However, when cortisol production is chronically turned up, it leads to abnormal deposition of fat (weight gain), increased risk of infection, impotence, abnormal blood sugars, brain fog, head


