

Category: Fat
Do You Still Have Your Favorite Red Dress?
Pass on the pretzels and the peanuts. We’ve got what you really need.

Keep following your ketogenic or carnivorous lifestyle and don’t throw that red dress out. We have your 20 minute treatment waiting for you at the office. . . EMSculpt Neo
Overcoming a Weight Loss Stall On a Ketogenic Diet
What do you do when you hit a weight loss stall while living a ketogenic lifestyle? Find out below. Dr. Nally goes into detail on the multiple causes of stalling while following a low-carbohydrate or ketogenic lifestyle. He dispels the myths around counting calories and macros. And, he discussed the basics of overcoming a stall.
Help Dr. Nally have time to make more great videos: https://www.patreon.com/docmuscles
What You MUST Know about Total Cholesterol & LDL-C on a Ketogenic Diet
Is following your Total Cholesterol and LDL-C really that important?
You may be quite surprised.
Watch as we discuss the important markers of heart disease and vascular disease risk. We will talk about how these markers can help you understand what your body is doing in the process of making or reversing atherosclerosis (plaque in the vessels). And, should you really be taking that STATIN (cholesterol lowering) drug? Get the scoop here as Dr. Nally very simply points out how the right diet can and will lower your cholesterol without the use of medications.
Research in the last 10 years points to the small-dense LDL particle as the atherogenic component of cholesterol (Hoogeveen RC et al., Arterioscler Thoromb Vasc Biol, 2014 May; Ivanova EA et al., Oxidative Med Cell Longevity, 2017 Apr). Studies in the last five years have identified that elevated small-dense LDL cholesterol correlates much more closely with risk for inflammation, heart disease and vascular disease (Williams PT, et al. Atherosclerosis. 2014 April; 233(2): 713-720.)
Recent research in the last three years demonstrates that small dense LDL cholesterol is a better marker for prediction of cardiovascular disease than total LDL-C (Hoogeveen RC et al., Arterioscler Thromb Vasc Biol. May 2014, 34(5): 1069-1077l; Ivanova EA et al., Oxidative Med Cell Longev. 2017).
Additionally, higher LDL-C is actually predictive of longer life and has been demonstrated to correlate with longevity (Ravnskov U et al., BMJ Open, 2016 Jun 12;6(6): e010401). And, a low LDL-C actually increases risk of early mortality (Schwartz I et al., Lancet 2001, 358: 351-55).
It is commonly understood that LDL-C will rise with increased saturated fat intake on a ketogenic diet. This has been know and reported in the scientific literature for over twenty years. This is to be expected, because LDL-C is really a measurement of three different LDL sub-particles (“big fluffy, medium, and small dense”). Increased saturated fat intake, while at the same time lowering carbohydrate intake, actually causes a shift in these low density particles to a bigger “fluffier” particle conformation (Griffin BA et al., Clin Sci (Lond), 1999 Sep).
The 2015 British Medical Journal, referenced above, analyzed the relevant 19 peer reviewed medical articles that included over 68,000 participants. This review showed that there is no association of high LDL-C with mortality (meaning that an elevated LDL-C does not lead to an increased risk of death from heart or vascular disease). I realize that, in stark opposition to the landmark review above, The American Heart Association’s Presidential Advisory published their position in the June 20, 2017 issue of Circulation. They stated that saturated fat is the cause of increased LDL-C and they further extrapolated that elevated LDL-C is associated with an increase in death by cardiovascular disease. This boldfaced claim is only based on one single small four year (2009-2013) literature review completed by the World Health Organization with a total of only 2353 participants, most of these studies only lasting 3-5 weeks (not nearly long enough to see fully effective cholesterol changes) and none of which had any focus on carbohydrate intake, insulin levels or LDL sub-particle measurement (Mensink RP, Geneva: WHO Library Cataloguing-in-Publication Data, 2016).
Based upon the most current scientific evidence above and my clinical experience, the large body of evidence above demonstrates the use of total cholesterol and LDL-C to determine vascular disease risk to be ineffective tools. A low carbohydrate/ketogenic diet lowers small dense LDL cholesterol, triglycerides and blood sugar and in many cases, the use of cholesterol drug (STATIN) therapy is not needed and ineffective in comparison with a ketogenic/carbohydrate restricted lifestyle.
All About Fat on a Ketogenic Diet (Can You Eat Too Much Fat?)
Catch my new video. I go into depth regarding why the type of fat you eat is very important on a ketogenic lifestyle. I reviews the effects of short, medium and long chain fats and how they are absorbed and used. We talk about starting a ketogenic diet and answer multiple viewer questions. Check it out!

The Shovel will Fail You in Obesity, Finances & Life
A few years ago, my family and I set out to build a pond.
I have always loved Koi and the serenity of a Koi pond in my own back yard was very enticing. I spent about a year planning my design and the location. I dreamed of a serene evening after a very long, hectic day seeing patients relaxing beside the pond. The sound of trickling water, the occasional splash from fish, the cool breeze passing over the mist from a water-fall would sooth my soul after a busy day in the office.
I envisioned the perfect area. An unused access path, previously worn by the previous owner with truck and trailer traffic, beside my now expanded patio. Twenty feet wide, thirty feet long and four feet deep. . . that seems just perfect.
I pulled out my shovel and set about digging. Eager to begin and filled with the energy of the final product, I set to digging. What could be so hard about digging my own pond? Think of the exercise I will be getting. Thoughts spurred me on.
Minutes later, chest heaving, face glistening with sweat, I stared in dismay at the ground. All I had to show for my wild digging was a small 1/2 inch dent in the dusty Arizona top soil.
Sonoran Clay
Over time, calcium-carbonate, along with other minerals, accumulates and dissolves into the topsoil of the very arid regions of Arizona Sonoran Desert. It forms a two to three-foot layer of soil called “caliche.” Periodic rains carry the calcium as far as three feet down into the soil, then the water rapidly evaporates in the blistering Arizona heat. This often forms two to three feet of soil that is “literally” harder than concrete.

With tremendous zeal, a great deal of sweat and a round of painful blisters, I broke my third shovel on this impenetrable ground. I realized this was much more difficult than I thought. I pulled out the back-hoe attachment for my small farm tractor. After a few hours and few gallons of diesel fuel later, still very little progress occurred.
Multiple weekends and evenings of digging in the Arizona caliche left me with three broken shovels, a ruptured hydrolic line in my tractor, anger that my expensive back-hoe attachment didn’t work, and only a small dent in the ground near my patio. Even the brute force from the tractor would not budge the clay. I wondered if dynamite would be effective? (My wife would have none of this idea).
With my exuberance quashed, I concluded that this would require much more measured exhuming.
Escape From the Prison
We often imagine, with great delight, the removal or destruction of that which enslaves or imprisons us. We dream that just a little sweat, exertion of a few shovel scoops of dirt and the foundation to our prison of obesity, addiction, debt, and depression are exposed. A few extra scoops and we imagine freedom from that prison cell.
If only I had a jack hammer and a bigger, more powerful scoop, I imagine . . . I could make short work of these manacles that bind me.
But, our manacles and prison cells do not so easily give way.
The failings of our sharpened spades and powerful back-hoes form a new, even stronger fetter – the belief that our prison cell is unbreakable, that our challenge is just too great. These failings usually leave a person cured of any further desire to break free. It quashs the dream and solidifying the depression of stagnation.
The in-fecundity of my shovel, no matter the strength and effort put behind it, was not cause to quit. It was life’s lesson that prisons and shackles often only need a simple tool.
Enter the pick-axe. During this process my wife said, “Honey, why don’t you use the pick in the garage?”
“If my shovel and the back-hoe didn’t work, there was no way I was going to break through this clay with a pick axe.” That was absurd, I thought.
Yet when I humbled myself to try, it was simple. The pick-axe was unpretentious. This simple tool allowed for an almost effortless stroke to a small area of weakness in the caliche. A large flake of soil would pop free with each stroke. The process was repeated.

Scale by scale, the dragon’s flank was exposed. Careful work of the pick-axe began to loosen layer after layer, section after section, pellicle after pellicle. Yes, it was slow work. But, each swing was a small victory.
At each little victory, my heart would leap, the dream would become ever clearer.
Working this magic again and again until finally the specter was weakened enough to pull out the shovel. And, further work, allowed for bringing back the powerful back-hoe, in gratifying scoops.
The excavation that I thought would take two months took me fourteen. But, it was gratifying.

I learned a powerful lesson. Wherever life has pinned you, fettered you or barred you in, put down the shovel, and pick up the pick-axe. Second, if you really listen, your spouse may point out the tool you really need. Don’t be afraid to chip away at it a piece at a time.

Finances
Stop waiting for the sharper shovel or the bigger back-hoe to dig yourself out of your harrowing debt, mega mortgage, or your income dwarfing spending. The jackpot or financial windfall won’t come. While others await the jackpot, put down your shovel and shoulder your pick-axe.
- Pick one small debt and begin to pick at it by applying just a little extra each month until it is gone.
- Cancel your extra cable, sell the motorcycle and payoff the 21% interest credit card.
- If you must, pick up a side-hustle for extra to sharpen the pick.
Once you’ve lifted one flake, chip away at the next. Making progress will make it easier to continue. It doesn’t matter how long it takes, just keep at it.
Marriage
You long for resolution of the apathy, progressive resentment and mutual stalemate that permeates your relationship. You look in vain for the bigger shovel that will uncover the treasure that years of apathy have buried. You long to uncover your dreams and needs that have been covered and hardened under the clay of resentment. The shovel and the back-hoe won’t help you here.
Drop the shovel. Shoulder your pick-axe.
- Kiss your wife every time you leave, even if it’s just for a ten minutes to run to the convenience store.
- Hold her for five seconds longer every time you hug.
- Find a gift you can give her once a week, just because.
- Put down your phone and look her in the eyes when she talks to you and listen. Really listen and the flakes of hard clay will unveil the beauty of her soul.
- Find a way to praise her every day, even if it is through a simple text.
Health
You long to rid yourself of your addiction to sugar, bread, stress, and sleep deprivation. You’ve tried to scoop them out of your life. You even hired a trainer with some muscle to force you to change. You’ve tried in vain to save yourself from yourself.
Trying to use the shovel here is like trying to use the shovel on steel forged walls of your life’s prison fortress. Forget the shovel. Shoulder your pick-axe.
- Start with one meal and make some substitutions. My dietary plan can help you with this.
- Go to bed an hour earlier. Really, you’ll be surprised that the focus you have will more than compensate for the hour of lost time in the evening.
- Add a quality vitamin to your morning routine.
- Take ten minutes and do 20 push-ups and 20 sit-ups, then take a 10-minute walk.
- Simply remove the “white stuff” from your meals. You will be amazed at the results.
- Put down your phone for 30 minutes and read that book you’ve been meaning to read, instead of surfing Facebook.
Grand-standing with your back-hoe doesn’t help you. Just swing the pick-axe once or twice. Simple daily picking with the sharp point weakens the hardest of ground and the prison walls in our lives. It takes time, so be patient.
Find the weak point, apply the pick. Day by day, little by little you will be free.

I’ve been there. I’m with you. Keep me posted on your journey.
If you’re looking for a program that teaches you how to do this, check out my membership site.

Long-Term Weight Loss: Why So Many Fail
Over fifty years of data have demonstrated that creating energy deficit through the reduction in caloric intake is effective in reducing weight. . . However, it is only for the short term (1, 2). The biggest challenge physicians face in the treatment of obesity is that calorie restriction fails when it comes to long-term weight loss.
Isn’t Fasting Effective in Long-Term Weight Loss?
With the craze and popularity of intermittent fasting, some have claimed that intermittent fasting is more effective in weight reduction. Recent results demonstrate that this may also be incorrect. In the short term evaluation of caloric restriction and intermittent fasting, reduction in 15-20 lbs of weight is effectively seen and the highly publicized Biggest Loser’s losing ~ 120 lbs. Intermittent fasting and alternate day fasting have been shown to be more effective in lowering insulin levels and other inflammatory markers in the short term.
There is, however, controversy over maintaining weight loss beyond 12 months in the calorie restriction, intermittent and alternate day fasting groups. Forty different studies in a recent literature review, thirty-one of those studies looking at forms of intermittent fasting, demonstrate that the majority of people regain the weight within the first 12 months of attempting to maintain weight loss(3, 5). This is, also, what I have seen for over 18 years of medical practice.
Is Calorie Restriction the Only Way to Lose Fat?
Numerous “experts” claim that the only way to reduce fat is “caloric deficit.” Variations through the use of intermittent, long-term or alternate day fasts can be found all over the internet. In regards to calorie restriction, these “experts” with nothing more than a personal experience and a blog to back their claims preach this louder than the “televangelists” preach religion. Based on the faith that many place in this dogma, it could be a religion. What causes belief in this dogma is that weight and fat loss actually does occur with caloric restriction to a point. The average person will lose 20-25 lbs, however, within 12 months of achieving this goal, most people regain all the weight. (No one ever mentions the almost universal problem with long-term weight loss, especially those “experts.”)
Prolonged calorie restricted fasts, intermittent fasts, and alternate day fasts are often grouped together into the fasting approach, causing significant confusion among those that I speak to and counsel in my office. There is great data that alternate day fasts do not have the reduction in resting energy expenditure that prolonged fasting, intermittent fasting and calorie restriction cause. However, none of these approaches appears to solve the problem of weight re-gain after long-term (12-24 months into maintenance) weight loss (3). And, a recent study of 100 men participating in alternate day fasting showed that there was a 38% dropout rate, implying that without close supervision and direction, maintenance of this lifestyle is not feasible for over 1/3rd of those attempting it.
Long-Term Weight Loss Failure Brings Tears
Failure on calorie restricted diets, low fat diets, and intermittent fasting diets with weight regain at twelve to twenty-four months is the most common reason people end up in my office in tears. They’ve fasted, starved themselves, calorie restricted, tried every form of exercise, and still regained the weight. Trainers, coaches and “experts” have belittled them for “cheating” or just not keeping to the diet. Yet, we know that calorie restriction and intermittent fasting cause a rebound in leptin, amilyn, peptid YY, cholecystikinin, insulin, ghrelin, gastric inhibitory peptide and pancreatic poly peptide by twelve months causing ineffective long-term weight loss (6). The dramatic rise in these hormones stimulates tremendous hunger, especially from ghrelin and leptin.

Although less problematic in alternate day fasting, these calorie restricted approaches also cause dramatic slowing of the metabolism at the twelve month mark. In many cases, the metabolic rate never actually returns to baseline, creating even more difficulty in losing further weight or even maintaining weight (6).

Is Gastric Bypass or Gastric Sleeve the Solution?
Gastric bypass and the gastric sleeve procedures have been touted as the solution to this problem, as they decrease ghrelin, however, 5-10 years later, these patients are also back in my office. They find that 5-10 years after these procedures the weight returns, cholesterol and blood pressure rise, and diabetes returns. These hormones kick into high gear, stimulating hunger in the face of a slowed metabolism, that to date, has been the driver for weight regain in the majority of people. People find it nearly impossible to overcome the hunger. You may have experienced this, I know I have.
It’s the Hormones, Baby!
So, what is the answer? It’s the hormones. (WARNING – You’ll hear that when your wife is pregnant, too, gentlemen). We are hormonal beings, both in weight gain, and in pregnancy. Trying to preach calorie control to a hormonal being is like showing up at the brothel to baptize the staff. You might get them into the water, but you’re probably not getting them returning weekly to church or pay a tithe.
 So, how do you manipulate the hormones in a way to control the rebounding hunger and suppression of metabolism? This is where we put a bit of twist on the knowledge we’ve gained from alternate day fasting. Recent research shows that “mild” energy deficit in a pulsatile manner, that has the ability to mimicking the body’s normal bio-rhythm’s is dramatically effective in reducing weight and maintaining normal hormonal function without cause of rebound metabolic slowing (4).
So, how do you manipulate the hormones in a way to control the rebounding hunger and suppression of metabolism? This is where we put a bit of twist on the knowledge we’ve gained from alternate day fasting. Recent research shows that “mild” energy deficit in a pulsatile manner, that has the ability to mimicking the body’s normal bio-rhythm’s is dramatically effective in reducing weight and maintaining normal hormonal function without cause of rebound metabolic slowing (4).
Pulsed Mild Energy Restriction
What does this mean in layman’s terms? It means that if we provide a diet that maintains satiety hormones while providing a period of baseline total energy expenditure needs and a period of mildly reduce caloric intake in a pulsed or cyclic manner, greater weight loss occurs and there is no rebound of weight 1-2 years later.
The main reason I’ve not jumped on the intermittent fasting band wagon is the shift in leptin, amylin, ghrelin and GLP-1 signaling that regularly occurs at the 6-12 month mark. The rebound of these hormones causes weight re-gain and is what prevents successful long-term weight loss. A number of people come to my office and tell me they couldn’t follow a ketogenic diet, so they’re doing intermittent fasting and it works . . . for a while. Then, they end up in my office having hit a plateau or fallen off the wagon and regained all the weight. They are completely confused and don’t understand what happned. Most of them are convinced it’s their thyroid or cortisol and they’ve seen every naturopath and functional medicine doctor in town.
What people really need is a simple approach to long-term weight loss without having to spend the night in the physiology lab every two weeks sleeping under a ventilated hood system.
The Ketogenic Lifestyle is a Pulsed Energy Lifestyle
- First, it is essential to turn off the insulin load. Insulin is the master hormone. This is done by a ketogenic lifestyle that restricts carbohydrates.
- Second, providing adequate protein to supply maintenance of muscle and testosterone is key.
- Third, providing adequate fat is the simple way to maintain leptin, ghrelin, amylin, GLP-1 (among the others) and long-term weight loss. Can you eat too much fat? Of course you can. But, because each of us have differing levels of stress and activity each day, this fat intake becomes the lever for hunger control.
- Fourth, the use of exogenous ketones ensures easily accessible ketone (short chain fatty acids) to modulate adipose (white fat) signaling of the liver without large caloric intake through the portal vein by first pass of liver metabolism. The ketones also help stabilize the gut bacteria. The combination of hormone balance between the liver and fat cells and improvement of gut bacteria suppresses key hunger hormones and aids glucose regulation between the fatty tissues and the liver. Ketones, both endogenous and exogenous, suppress production of TNF-alpha, IL-6, resistin, and stabilize production of adiponectin and leptin from the adipose cells (7, 8, 9).
In my office, once we calculate the basic protein needs daily, we start with a 1:1 ratio of protein to fat. Then, the fat is adjusted up or down based on hunger. Remember, hunger occurs, because your body produces hormones. The addition of fat to a diet that is not stimulating large amounts of insulin resets the hormone patterns back to normal without causing weight gain.
Give Obese People Fat Ad Libitum?
“Sure, Dr. Nally, but what about those people who don’t know if they are hungry, bored, stressed or just have a bacon fixation? You can’t just give them all the fat they want?!”
Why not? Implying that people aren’t smart enough to know when they are full is a bit of a fascist philosophy, don’t you think?
Do people over eat? Sure they do. But, I’ve found that when you give people an antidote to hunger (using fat intake in the presence of stabilized insulin levels) over a few months, people begin to recognize true hunger from other forms of cravings. This is especially true when they keep a diet journal. This gives people the ability to begin listening to their own bodies, responding accordingly and governing their stress, eating, exercise and activity. Keeping a diet journal is key to long-term weight loss. And, isn’t helping people use their own agency to improve their health really what we’re trying to do?
Interestingly, doing this over the years seems to line up with the findings of this year’s MATADOR study in the International Journal of Obesity. They found that mild intermittent energy restriction of about 30-33% for two weeks, then interrupting this with two weeks of a diet that was energy balanced for needs improved both short and long-term weight loss efficiency (4). In looking at my, and my patient’s diet journals, this energy restriction of about 1/3 of needed calories cyclically seems to happens naturally with a ketogenic lifestyle, without even counting calories. (Calories are a swear-word in my office).
What does the correct long-term wight loss program look like in a diet or meal plan? Well, you’ll have to join the Ketogenic Lifestyle 101 Course to see what that really means to you individually. I look forward to seeing you there.
Want to find out more about the Ketogenic Lifestyle 101 course? CLICK HERE.
Have you read my book The Keto Cure? Get a signed copy from me by clicking HERE.
References:
- Bronson FH, Marsteller FA. “Effect of short-term food deprivation on reproduction in female mice.” Biol Reprod. Oct 1985; 33(3): 660-7. https://www.ncbi.nlm.nih.gov/pubmed/4052528?dopt=Abstract&holding=npg
- Connors JM, DeVito WJ, Hedge GA. “Effects of food deprivation on the feedback regulation of the hypothalamic-pituitary-thyroid axis of the rat.” Endocrinology. Sep 1985. 117(3): 900-6. https://www.ncbi.nlm.nih.gov/pubmed/3926471?dopt=Abstract&holding=npg
- Seimon RV, Roekenes JA, Zibellini J, Zhu B, Gibson AA, Hills AP, Wood RE, King NA, Byrne NM, Sainsbury A. “Do intermittent diets provide physiological beneftis over continuous diets for weight loss? A systematic review of clinical trials.” Mol Cell Endo. 15 Dec 2015. 418(2): 153-172. https://www.sciencedirect.com/science/article/pii/S0303720715300800
- Byrne NM, Sainsbury A, King NA, Hills AP, Wood RE. “Intermittent energy restriction improves weight loss efficiency in obese men: the MATADOR study.” Int J Obes. 2018. 42:129-138. https://www.nature.com/articles/ijo2017206
- Trepanowski JF, Kroeger CM, Barnosky A. “Effect of Alternate-Day Fasting on Weight Loss, Weight Maintenance, and Cardioprotection Among Metabolically Healthy Obese Adults.” JAMA Intern Med. Jul 2017. 177(7): 930-938. https://jamanetwork.com/journals/jamainternalmedicine/article-abstract/2623528?redirect=true
- Sumithran P, Prendergast LA, Delbridge E, Purcell K, Shulkes A, Kriketos A, Proietto J. “Long-term persistence of hormonal adaptations to weight loss.” N Engl J Med. 27 Oct 2011. 365: 1597-1604. http://www.nejm.org/doi/full/10.1056/NEJMoa1105816
- Asrih M et al., “Ketogenic diet impairs FGF21 signaling and promotes differential inflammatory responses in the liver and white adipose tissue.” PlosOne. 14 May 2015. Open Access. https://doi.org/10.1371/journal.pone.0126364
- Veniant MM et al. “FGF21 promotes metabolic homeostasis via white adipose and leptin in mice.” PlosOne. Jul 2012. Open access. https://doi.org/10.1371/journal.pone.0040164
- Whittle AJ, “FGF21 conducts a metabolic orchestra and fat is a key player.” Endocrinology. 1 May 2016. 157(5): 1722-1724.
SculpSure Non-Invasive Fat Reduction
I am excited to announce that we just added the SculpSure Laser to our treatment offerings at Nally Family Practice. Many of my patient’s have very successfully lost weight with a ketogenic lifestyle; and I am still a strong advocate of a ketogenic lifestyle for maintenance of health, weight and over-all wellness.
After years of carrying extra weight, a number of my patients still struggle with that last stubborn problem areas like the belly and love handles. I’ve been waiting for over 15 years for technology to catch up to treat theses areas, . . . and now it has. 
Introducing SculptSure, the non-invasive fat reduction laser that can customize fat reduction in the problem spots.


Call our office today to schedule your consultation with Dr. Nally and his staff to find out if SculpSure is right for you!
(623) 584-7805
Why Be In Ketosis? Part VII – cGMP (Making Fat Burning Efficient)
Many people ask me, “Dr. Nally, why should I always be in ketosis even if I burn fat and lose weight without restricting carbohydrates as much as you do?”
The answer is fat burning efficiency. Shifting into ketosis changes your ability to burn fat, and do it efficiently by turning on cGMP in the adipocyte. I explain how below:
Enjoy!! You can click the link below to ramp up your ketosis through the use of exogenous ketones at DynamicKetones.com. Yes, I make a profit from the sale of exogenous ketones, but I just gave you the magic bullet for opening up the adipocyte for FREE!
Merry Christmas!
Is Your Sweetener Making you FAT?
I am frequently asked about the sweeteners that can be used with a low carbohydrate diet. There are a number of sweeteners available that are used in “LowCarb” pre-processed foods like shakes or bars, or in cooking as alternatives to sugar; however, many of them raise insulin levels without raising blood sugar and are not appropriate for use with a true low-carbohydrate/ketogenic diet. You can see and print the article I published clarifying which sweeteners you can use and which ones to avoid in the menu bar above “Sour Truth About Sweeteners” and you can watch last night’s periscope below:
Enjoy!!
Thinking Outside of the Box

The image above has nine dots within a square. Your task, using only four lines is to connect ALL nine dots WITHOUT ever raising your pen, pencil or finger (Please don’t use a sharpie on your computer screen . . . it doesn’t come off).
You may have seen this puzzle previously . . . it’s made its rounds in corporate training circles. But the underlying principle remains true. The solution requires you to expand your thinking or to “think outside the box.”
Whenever you find yourself on the side of the majority, it is time to pause and reflect. (Mark Twain)
Why should we limit ourselves to thinking outside the box. Can’t we just get rid of the box?
True discovery consists in seeing what everyone has seen . . . then, thinking what no one has thought.
{kind=link}
The answer can be found when those four lines are used beyond the box our mind creates:

What good has the box done us? People were burned at the stake because they refused to believe the Earth was not the center of the universe. People were beheaded because they had a sneaking suspicion that the world was not flat.
Why is it so very hard to accept that our weight gain and diabetes are driven by a hormonal signal, and not by gluttony or caloric intake of fat? The definition of insanity is doing the same thing repetitively and expecting a different outcome. How long have you been restricting calories and fat with only minimal or no improvement in your weight, blood sugar, cholesterol or general feeling of health?
The main problem with the current thought model, or dogma, on the obesity’s cause is that it does not account for metabolic syndrome. Metabolic syndrome is insulin resistance. It is an over production of insulin in the presence of ANY form of carbohydrate (sugar or starch).
In the practice of medicine over the last 15 years, I noticed that a very interesting pattern emerged. There was always a spike in fasting and postprandial insulin levels 5-10 years prior to the first abnormal fasting and postprandial blood sugars. These patients were exercising regularly and eating a diet low in fat. But they saw continued weight gain and progressed down the path of metabolic syndrome. 10-15 years later, they fall into the classification of type II diabetes. What I now lovingly refer to as stage IV insulin resistance.
The only thing that seems to halt this progressive process with any degree of success is carbohydrate restriction. Fasting insulin levels return to normal, weight falls off, and the diseases of civilizations seem to disappear as insidiously as they arose.
So you tell me, is the world flat? Is the Earth the center of the universe?

What is a low carbohydrate or ketogenic diet? 15 years of practical in the trenches experience have helped me develop a very simple program to help you lose and maintain your weight. Access to this program, video help and access to blog articles at your fingertips are offered through my online membership site.
You can also hear me each week a I discuss low carbohydrate, paleolithic and ketogenic diets with the Legendary Jimmy Moore on KetoTalk.com
Definition of Insanity: Cutting Calories/Restricting Fat & Expecting Weight Loss
Have you been cutting your calories and reducing fat and exercising your brains out and still not seeing the needle on the scale move that much? Persistently and repetitively performing an action that doesn’t produce the desired result is insanity. Cutting calories and reducing fat while expecting weight loss is akin to pouring water in the gas tank of your car and expecting it to run smoothly. Why do we do it? Are the 53, 000, 000 people with health club and gym memberships this year really insane?
This evening on PeriScope we touch on fat phobic insanity and the limiting step that actually turns weight gain on or off. (We knew about this in the 1960’s, we just ignored it.)
You can see tonight’s PeriScope with the rolling chat-box questions here at Katch.me/docmuscles. Or, you can watch the video stream below:
The only way to successfully loose weight is to modify or turn off the mechanisms that stimulate fat storage. For years we have been told that this was just a problem of thermodynamics, meaning the more calories you eat, the more calories you store. The solution was, thereby, eat less calories or exercise more, or both. We are taught in school that a 1 gram of carbohydrate contains 4 kcal, 1 gram of protein contains 4 kcal, and 1 gram of fat contains 9 kcal.
If you ascribe to the dogma that weight gain or loss is due to thermodynamics, then it’s easy to see that cutting out fat (the largest calorie containing macro-nutrient) would be the best way limit calories. For the last 65 years, we as a society have been doing just that, cutting out fat, exercising more (with the idea of burning off more calories) and eating fewer calories.
What has this dogma done for us? It’s actually made us fatter! (1)

Some may argue that we really aren’t eating fewer calories and exercising more. But most people I have seen in my office have tried and tried and tried and failed and failed and failed to loose weight with this methodology. In fact, the majority of my patients attempt caloric restriction, exercise and dieting multiple times each year with no success. The definition of insanity is “doing the same thing over and over and expecting a different result.”
Most of my patients are not insane, they recognize this and stop exercising and stop restricting calories . . . ’cause they realized, like I have, that it just doesn’t work!
If you’re one that is still preaching caloric restriction and cutting out fat, I refer you to the figure above and the definition of insanity . . . your straight-jacket is in the mail.
So, if reducing the calories in our diet and exercising more is not the mechanism for turning on and off the storage of fat, then what is?
Before I can explain this, it is very important that you appreciate the difference between triglycerides and free fatty acids. These are the two forms of fat found in the human body, but they have dramatically different functions. They are tied to how fat is oxidized and stored, and how carbohydrates are regulated.
Fat stored in the adipose cells (fat cells) 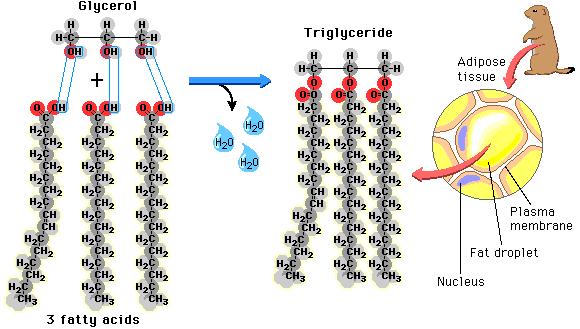 as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
(“What! Fat comes from sugar?! How can this be?!!“)

We all know that glucose derived from sugar is taken up by the cells from the blood stream and used for fuel, however, when too much glucose is in the blood stream or the blood sugar increases above the body’s comfort zone (60-100 ng/dl), the body stores the excess. The process is called de novo lipogenesis, occurring in the liver and in the fat cells themselves, fancy Latin words for “new fat.” It occurs with up to 30% (possibly more if you just came from Krispy Kream) of the of the carbohydrates that we eat with each meal. De novo lipogenesis speeds up as we increased the carbohydrate in our meal and slows down as we decrease the carbohydrate in our meal. We’ve known this for over 50 years, since it was published by Dr. Werthemier in the 1965 edition of the Handbook of Physiology (2).
While we know that fat from our diet and fat from our food is stored as triglyceride, it has to enter and exit the fat cell in the form of fatty acids. They are called “free fatty acids” when they aren’t stuck together in a triglyceride. In their unbound state, they can be burned as fuel for the body within the cells. I like to think of the free fatty acids as the body’s “diesel fuel” and of glucose as the body’s version of “unleaded fuel.” The free fatty acids can easily slip in and out of the fat cell, but within the adipose cell, they are locked up as triglycerides and are too big to pass through the cell membranes. Lipolysis is essentially unlocking the glycerol from the free fatty acids and allowing the free fatty acids to pass out of the fat cell. Triglycerides in the blood stream must also be broken down into fatty acids 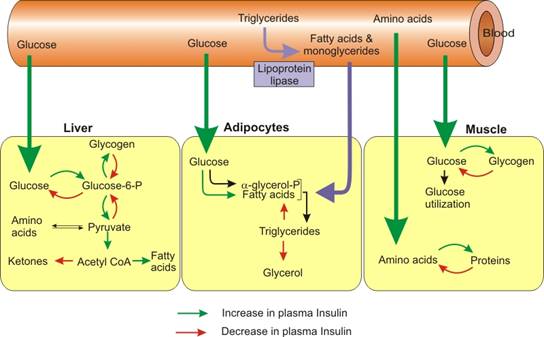 before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).
before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).
So when carbohydrates increase in the diet, the flow of fat into the fat cell increases, and when carbohydrates are limited in the diet, the flow of fat out of the fat cells increases.
Summarizing the control mechanism for fat entering the fat cell:
- The Triglyceride/Fatty Acid cycle is controlled by the amount of glucose present in the fat cells (conversion to glycerol phosphate) and the amount of insulin in the blood stream regulating the flow of fatty acid into the fat cell
- Glucose/Fatty Acid cycle or “Randle Cycle” regulates the blood sugar at a healthy level. If the blood glucose goes down, free fatty acids increase in the blood stream, insulin decreases, and glycogen is converted to glucose in the muscle and liver.
These two mechanisms ensure that there is always unleaded (glucose) or diesel fuel (free fatty acids) available for every one of the cells in the body. This provides the flexibility to use glucose in times of plenty, like summer time, and free fatty acids in times of famine or winter when external sources of glucose are unavailable.
The regulation of fat storage, then, is hormonal, not thermodynamic. Unfortunately, we’ve know this for over 65 years and ignored it.
We’ve ignored it for political reasons, but that’s for another blog post . . .
References:
1. James, W. J Intern Med, 2008, 263(4): 336-352
2. Wertheimer, E. “Introduction: A Perspective.” Handbook of Physiology. Renold & Cahill. 1965.
3. Taubs, G. “The Carbohydrate Hypothesis, II” Good Calorie, Bad Calorie. Random House, Inc. 2007, p 376-403.
Why the Calorie is NOT King
Today in the office I had the calorie conversation again . . . three times. We have an entire society with a very influential health and fitness industry built around the almighty calorie. Has it helped? Looking at our 5 year obesity outcomes. It hasn’t helped a bit. In fact, it is worse. In 1985 only 19% of U.S. adults were obese.
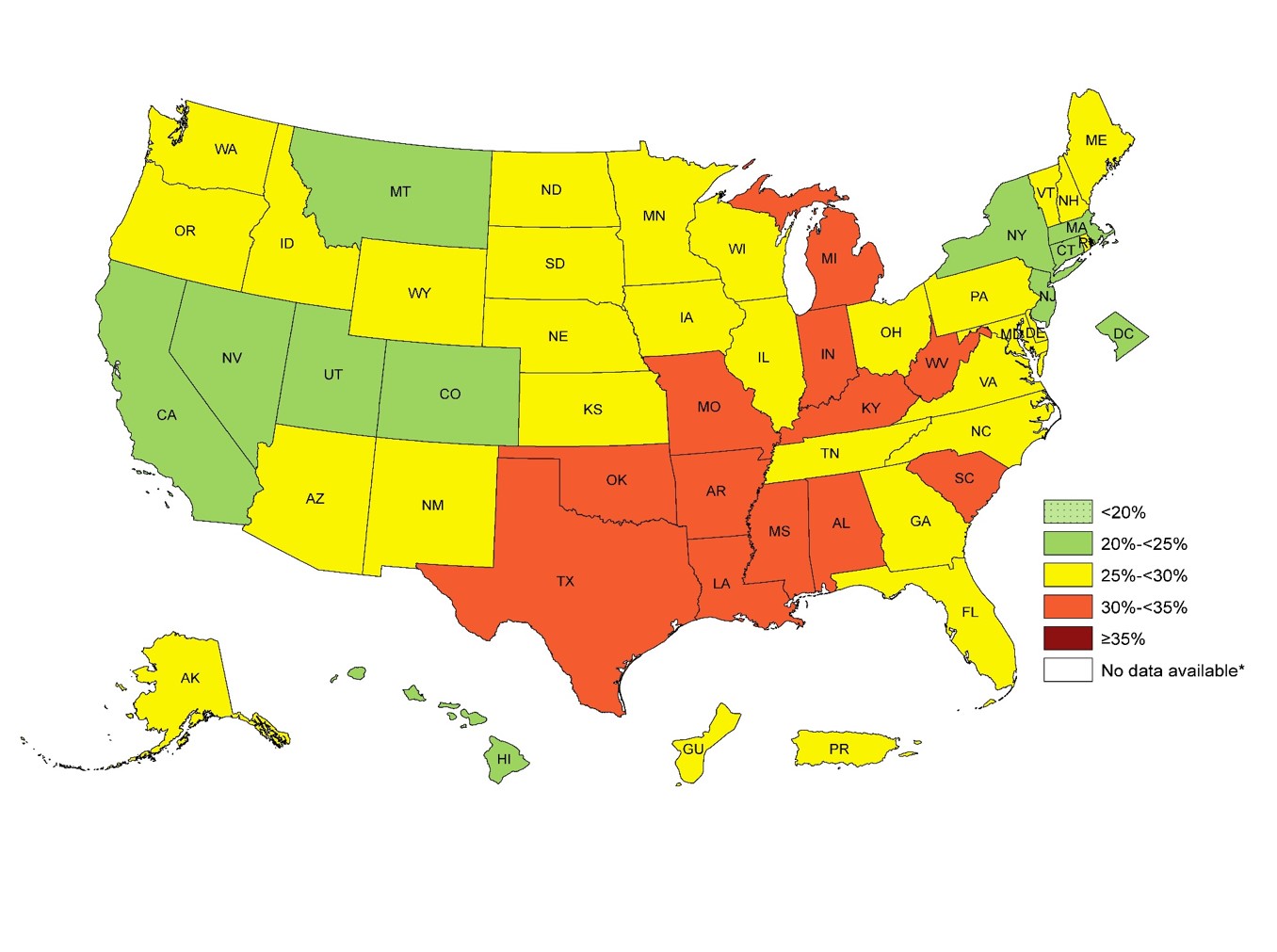
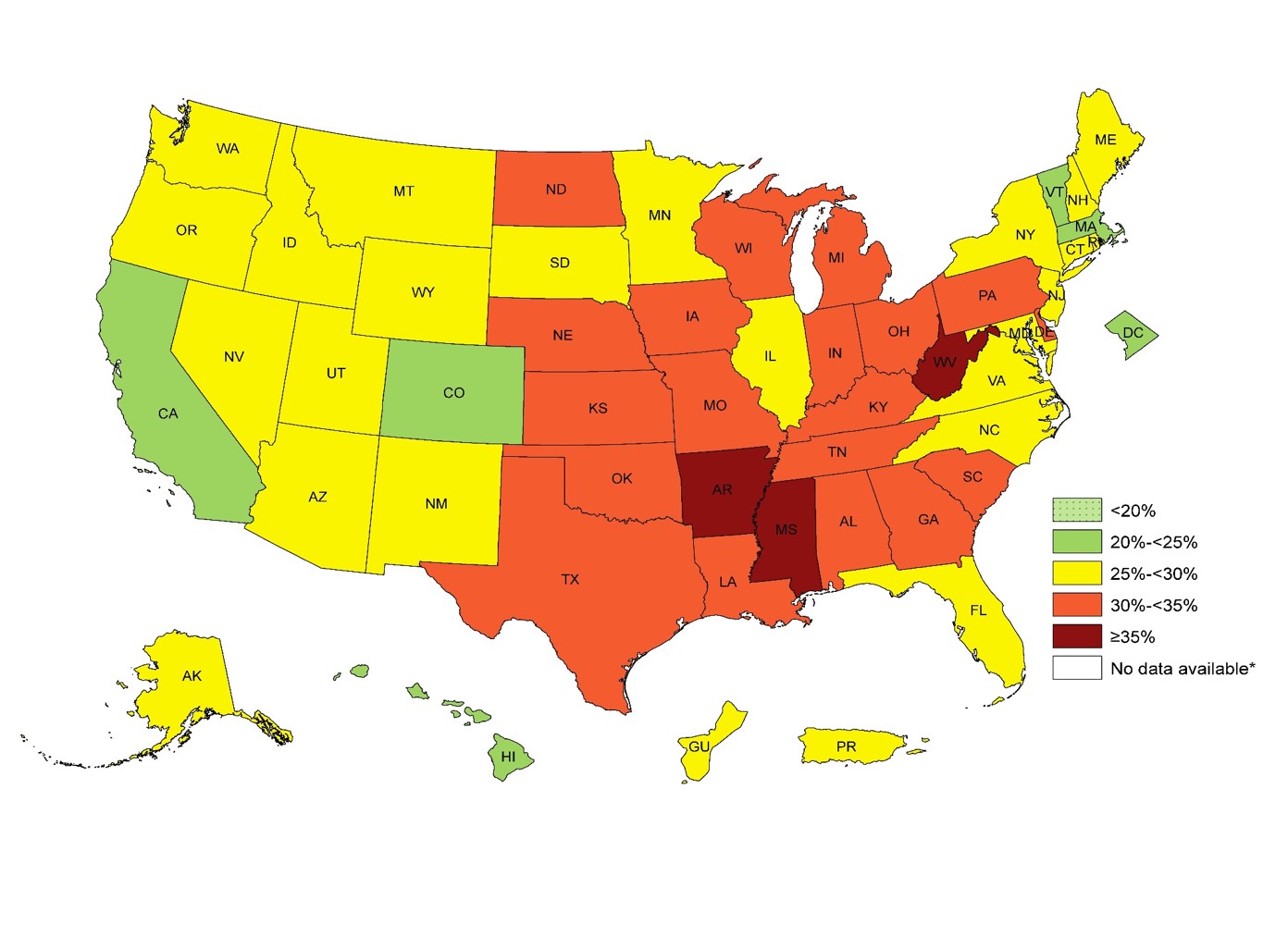
In 2014, 34.5% of U.S. adults were obese. The numbers this year are approaching 35.6% You can see the dramatic increase in obesity by 1-3% every year for the last 5 years in the CDC images above.
For over 50 years we have been told that caloric restriction and fat restriction is the solution. But by the numbers above, the 58 million people in the U.S. utilize a gym or health club to burn off those calories aren’t seeing the success that they should be expecting.
Why? Because the calorie is NOT king. What do I mean by that? We don’t gain weight because of the thermogenic dogma we’ve been taught for the last 50 years. Our weight gain is driven by a hormone response to food. Hear more about why the calorie is NOT king on tonight’s PeriScope. You can Katch it here with all the live stream comments and hearts at Katch.me/docmuscles.
Or you can watch the video without the comments here:
Pre-, Post-Workout Meal on Ketosis. Is it Important?
Today’s Periscope was an exciting one. Do you really need a pre- or post-workout shake or meal? How much protein do you need? What’s the difference between ketosis and ketoacidosis? Is Dr. Nally a ketogenic cheerleader? Get your answers to these and many more questions asked by some wonderful viewers this evening on today’s PeriScope.
https://katch.me/embed/v/5def6bce-4f67-363a-b5f9-3bbec8a8aea2?sync=1
Be sure to check out Dr. Nally’s new podcast called “KetoTalk with Jimmy and the Doc” with the veteran podcaster Jimmy Moore on KetoTalk.com. The first podcast will be available on December 31, 2015. KetoTalk with Jimmy and the Doc will be available for download for free on iTunes.
Stay tuned . . . !
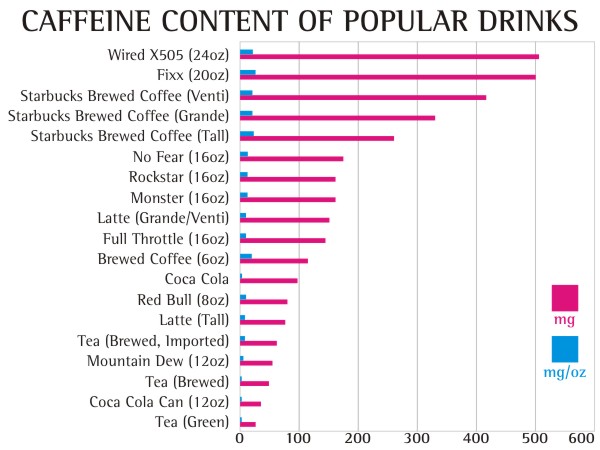
Caffeine . . . Weight Loss Wonder Boy or Sneaky Scoundrel?
I’ve been looking for the answer for quite some time. . . what role does caffeine play in your and my weight management journey? The answer gave me a headache. . . literally and figuratively.
As many of you, including my office staff, know, I love my Diet Dr. Pepper (and my bacon). I found that being able to sip on a little soda throughout the day significantly helped the carbohydrate cravings and munchies during a busy and stressful day at the office. Diet Dr. Pepper contains caffeine, however, I wasn’t really worried. Caffeine has been well know to have a thermogenic effect which increases your metabolism and has been thought for many years to help with weight loss among the weight loss community.
Diet Dr. Pepper is, also, one of only four diet sodas on the grocery store shelves that doesn’t contain acesulfame potassium (click here to see why most artificial sweeteners cause weight gain). The four diet sodas that I have been comfortable with my patients using are Diet Dr. Pepper, Diet Coke, Diet Mug Root-beer and Diet A&W Cream Soda. These are the last four hold out diet sodas that still use NutraSweet (aspartame) as the sweetener. Most of the soda companies have switched the sweetener in their diet sodas to the insulinogenic acesulfame potassium because it tastes more natural and aspartame has been given a media black eye of late. However, NutraSweet (aspartame) is the only sweetener that doesn’t spike your insulin or raise blood sugar (click here to find out why that is important).
Yes, I know. The ingestion of 600 times the approved amount of aspartame causes blindness in lab rats (but we’re not lab rats, and . . . have you ever met someone that drinks 600 Diet Dr. Peppers in a day? The lethal dose of bananas, which are high in potassium that will stop your heart, is 400). Aspartame can also exacerbate headaches in some (about 5% of people) and I’ve had a few patients with amplified fibromyalgia symptoms when they use aspartame. But for most of us, its a useful sweetener that doesn’t spike your insulin response, halting or causing weight gain.
But, over the last few years, I’ve noticed that increased amounts of Diet Dr. Pepper & Diet Coke seem to cause plateauing of weight and decreasing the ability to shift into ketosis, especially mine. I’ve also noticed (in my personal n=1 experimentation) that my ability to fast after using caffeine regularly seems to be less tolerable, causing headaches and fatigue 8-10 hours into the fast, symptoms that don’t seem to let up until eating. Through the process of elimination, caffeine seems to be the culprit.
 After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the August 2004 Diabetes Care Journal screamed for my attention.
After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the August 2004 Diabetes Care Journal screamed for my attention.
It appears that caffeine actually stimulates a glucose and insulin response through a secondary mechanism. The insulin surge and glucose response is dramatically amplified in patients who are insulin resistant. Caffeine doesn’t effect glucose or insulin if taken while fasting; however, when taken with a meal, glucose responses are 21% higher than normal, and insulin responses are 48% higher in the insulin resistant patient. Caffeine seems to only effect the postprandial (2 hours after a meal) glucose and insulin levels. The literature shows mixed responses in patients when caffeine is in coffee or tea, probably due to the effect of other organic compounds (1).
Caffeine also diminishes insulin sensitivity and impairs glucose tolerance in normal and already insulin resistant and/or obese patients. This is seen most prominently in patients with diabetes mellitus type II (stage IV insulin resistance). Caffeine causes alterations in glucose homeostasis by decreasing glucose uptake into skeletal muscle, thereby causing elevations in blood glucose concentration and causing an insulin release (2-6).
Studies show that caffeine causes a five fold increase in epinephrine and a smaller, but significant, norepinephrine release. The diminished insulin sensitivity and exaggerated insulin response appears to be mediated by a catacholamine (epinephrine, norepinephrine & dopamine) induced stress response (5). Caffeine has a half life of about 6 hours, that means the caffeine in your system could cause a catacholamine response for up to 72 hours depending upon the amount of caffeine you ingest (7).
The reason for my, and other patient’s, headaches and fatigue after a short fast was due to the exaggerated stress hormone response. Increased levels of insulin were induced by a catacholamine cascade after caffeine ingestion with a meal, dramatically more amplified in a person like me with insulin resistance. The caffeine with the last meal cause hypoglycemia 5-7 hours into the fasting, leading to headaches and fatigue that are only alleviated by eating.
Even when not fasting, the caffeine induced catacholamine cascade causes up to 48% more insulin release with a meal, halting weight loss and in some cases, causing weight gain.
Caffeine is not the “Wonder-Boy” we thought it was.
How much caffeine will cause these symptoms? 50 mg or more per day can have these effects.
Ingestion of caffeine has the following effects:
- 20-40 mg – increased mental clarity for 2-6 hours
- 50-100 mg – decreased mental clarity, confusion, catacholamine response
- 250-700 mg – anxiety, nervousness, hypertension & insomnia
- 500 mg – relaxation of internal anal sphincter tone (yes . . . you begin to soil yourself)
- 1000 mg – tachycardia, heart palpitations, insomnia, tinnitus, cognitive difficulty.
- 10,000 mg (10 grams) – lethal dose (Yes, 25 cups of Starbucks Coffee can kill you)
The equivalent of 100 mg of in a human was given to a spider, you can see the very interesting effect on productivity. How often does the productivity of the day feel like the image below?

Beware that caffeine is now being added to a number of skin care products including wrinkle creams and makeup. Yes, caffeine is absorbed through the skin, so check the ingredients on your skin care products.
Diet Dr. Pepper, my caffeine delivery system of choice, has slightly less caffeine (39 mg per 12 oz can or 3.25 mg per oz) than regular Dr. Pepper. I found myself drinking 2-3 liters of Diet Dr. Pepper per day (long 16-18 hour work days in the office). After doing my research, I realized that my caffeine tolerance had built up to quite a significant level (230-350 grams per day).
So, a few weeks ago, I quit . . . cold turkey.
Did I mention the 15 withdrawal symptoms of caffeine? (8)
- Headache – behind the eyes to the back of the head
- Sleepiness – can’t keep your eyes open kind of sleepiness
- Irritability – everyone around you thinks you’ve become a bear
- Lethargy – feels like your wearing a 70 lb lead vest
- Constipation – do I really need to explain this one?
- Depression – you may actually feel like giving up on life
- Muscle Pain, Stiffness, Cramping – feel like you were run over by a train
- Lack of Concentration – don’t plan on studying, doing your taxes or performing brain surgery during this period
- Flu Like Illness – sinus pressure and stuffiness that just won’t clear
- Insomnia – you feel sleepy, but you can’t sleep
- Nausea & Vomiting – You may loose your appetite
- Anxiety – amplified panic attacks or feeling like the sky is falling
- Brain Fog – can’t hold coherent thoughts or difficulty with common tasks
- Dizziness – your sense of equilibrium may be off
- Low Blood Pressure & Heart Palpitations – low pressure and abnormal heart rhythm
I experienced 13 of the 15 that lasted for 4 days. I do not recommend quitting cold turkey unless you have a week off and someone to hold your hand, cook your meals and dose your Tylenol or Motrin. My wife thought I was dying. . . I thought I was dying on day two. I actually had a nightmare about buying and getting into my own coffin. It can take up to three weeks to completely recover from caffeine withdrawal.
The other way to quit is to decrease your caffeine intake by 50 mg every two days. That means decrease caffeine by:
- 1 can of soda every two days
- 1/4 cup of coffee every day
- 1/2 can of Energy Drinks every two days
- 1 cup of tea every two days
The benefit of this method is that withdrawal symptoms are much less severe without the caffeine headache and the ability to remain productive. It will take longer, but quitting cold turkey is not a pretty picture. Been there . . . done that, . . . and I’m not going back. I actually lost another half inch off my waistline by day 5 of caffeine discontinuation.
What is the take home message here? If you have any degree of insulin resistance, caffeine makes it worse and will amplify your weight gain as well as decrease the productivity of your day.
References:
- Lane JD, Barkauskas CE Surwit RS, Feinglos MN, Caffeine Impairs Glucose Metabolism in Type II Diabetes, Diabetes Care August 2004 vol. 27 no. 8 2047-2048; doi:10.2337/diacare.27.8.204
- Jankelson OM, Beaser SB, Howard FM, Mayer J: Effect of coffee on glucose tolerance and circulating insulin in men with maturity-onset diabetes. Lancet 1: 527–529, 1967
- Graham TE, Sathasivam P, Rowland M, Marko N, Greer F, Battram D: Caffeine ingestion elevates plasma insulin response in humans during an oral glucose tolerance test. Can J Physiol Pharmacol 79:559–565, 2001
- Greer F, Hudson R, Ross R, Graham T: Caffeine ingestion decreases glucose disposal during a hyperinsulinemic-euglycemic clamp in sedentary humans.Diabetes 50:2349–2354, 2001
- Keijzers GB, De Galan BE, Tack CJ, Smits P: Caffeine can decrease insulin sensitivity in humans. Diabetes Care 25:364–369, 2002
- Petrie HJ, et al. Caffeine ingestion increases the insulin response to an oral-glucose-tolerance test in obese men before and after weight loss. American Society for Clinical Nutrition. 80:22-28, 2004
- Evans SM, Griffiths RR, Caffeine Withdrawal: A Parametric Analysis of Caffeine Dosing Conditions, JPET April 1, 1999 vol. 289no. 1 285-294
- Noever R, Cronise J, Relwani RA. Using spider-web patterns to determine toxicity. NASA Tech Briefs April 29,1995. 19(4):82. Published in New Scientist magazine, 29 April 1995
How Do You Know if You’re Insulin Resistant?
How do you know if you're insulin resistant? What questions need to be asked? What should your numbers be? And, many other great ketosis questions. Also, why does Dr. Nally look like he has dirt on his chin? See it here . . .
What Lab Testing Do You Need to Start Your Weight Loss Journey?
What laboratory testing is necessary when you start your weight loss journey on a Ketogenic, Low-Carbohydrate, Paleolithic or any other dietary changes? Why do you need them and what are you looking for? We discuss these questions and others on today’s PeriScope. Lots of questions from around the world to day . . . this one lasted a bit longer than normal . . . 45 minutes to be specific. But it’s a good one because of all of your fantastic questions! You really don’t want to miss this one.
You can see the video below or watch the video combined with the rolling comments here on Katch.me/docmuscles.
A list of the labs that we discussed are listed below:
- Fasting insulin with 100 gram 2 or 3 hour glucose tolerance test with insulin assay every hour
- CMP
- CBC
- HbA1c
- Leptin
- Adiponectin
- C-Peptid
- NMR Liprofile or Cardio IQ test
- Lipid Panel
- Urinalysis
- Microalbumin
- Apo B
- C-reactive protein
- TSH
- Thyroid panel
- Thyroid antibodies
- AM Cortisol
This list will at least get one started, provide the screening necessary to identify insulin resistance (Diabetes In-Situ), Impaired fasting glucose, diabetes and allow for screening for a number of the less common causes of obesity.
I would highly recommend that you get these through your physician’s office so that appropriate follow up can be completed. These labs will need to be interpreted by your physician, someone who understands and is familiar with various causes of obesity.
Until next time . . .
Chewing the Phat with Dr. Nally (The Psychology of Fat & Many Other Questions)
Join me as we chew the phat of ketogenic lifestyles PeriScope style and answer many questions like, “Why do I get ‘hangry’?” What causes hypoglycemia? How many times a day should I eat? and many more . . .
We talk briefly about why 60% of people with insulin resistance may need methylated folic acid to help with B vitamin absorption/use and where it can be found. (See me recent article about this called The Power of a Good Vitamin.)
You can see the whole PeriScope conversation on Katch.me/docmuscles with the comments scrolling or you can see the video stream below:
Thanks for visiting!!!
The Truth is . . . Caloric Restricted Exercise Won’t Work
This post isn’t going to win me any friends . . . in fact, mentioning this topic a few days ago has already angered a number of them and resulted in an online tongue lashing by a few others. However, I can’t resist. And, based on some very persuasive data and personal experience, I don’t care.

Truth is truth . . . it doesn’t change no matter how you spin it, or attempt to fit it into your paradigm. The problem is what we have accepted in the last 40-50 years as “the scientific truth about getting healthy” is far from truth. By getting healthy, I’m implying the application of main-stream methods accepted to lose weight, reduce cholesterol, improve blood pressure and reduce your risk of heart disease and diabetes. 
For the last 40 years we’ve been told that the only way to get and live healthy is to restrict our calories. This main-streamed advise continues even today in our USDA 2010 Dietary Guidelines. And, if you ascribe to this futile dogma propagated since the 1970’s, then you’ll know that the “only acceptable way” to do this is to “eat less fat” (because fat is the most caloric dense of the macro-nutrients, right?) and to “exercise more” (because that’s how we burn calories, right?!) Well, that’s what I thought, too. And that  is the health prescription I doled out to my-self and to all of my patients for the first 8 years of my practice.
is the health prescription I doled out to my-self and to all of my patients for the first 8 years of my practice.
Interestingly, most of them, including myself, took that prescription of a caloric restricted diet of 1200-1500 calories per day and exercise 3-6 days a week for 30-60 minutes and ran with it. Personally, I restricted calories to 1200-1500 per day and began running triathlons. I performed cardiac monitored running, swimming and cycling for an hour a day during the week and 2 hours on the weekend. I lifted weights 2-3 days per week as well. Guess what it got me?  Fat.
Fat.
It raised my triglycerides by 100 points, elevated my LDL-C and increased my waistline by 3 inches. Yes, I gained weight. But, hey, my doctor was happy because my HDL-C went up by 4 points.
I saw this identical pattern with 3/4ths the patients in my office. A fourth of my patient’s (the group without any genetic insulin resistance) saw weight loss and improvement in their cholesterol profiles, but the rest didn’t. I had the exciting opportunity to introduce the saddened and discouraged 3/4ths of my patients to STATIN drugs and blood pressure medications. My average patient’s gained 2-3% of their body fat each year. Those that exercised like fiends were lucky if their weigh gain just stabilized. 
What I saw in my office over a period of eight years was that exercise and caloric restriction didn’t work. But I couldn’t say that, because that goes against everything your 8th grade health teacher taught you. It contradicted your neighborhood dietitian, and it spat in the face of the food pyramid and the USDA Guidelines. The Government wrong? Never. . . . Speaking contradictory of the calorie-in/calorie-out exercise dogma was heresy, right? Contradict, Dr. Ornish, wouldn’t be heard of?!!
If I’ve learned one thing in my medical career, it is this: “Don’t be afraid to question everything” – even Dr. Dean Ornish, the USDA and the American Heart Association. And, fascinatingly, I’m not the only on that did.
——
——
Three Massive Studies did just that . . . question whether this exercise and caloric restriction dogma really works. This is what applying exercise and caloric cutting did for almost 67,000 people between 1972 and 2010 – little to nothing.
WHAT?!! Nothing?! You can’t be serous?
The first of these trials was the MRFIT (Multiple Risk Factor Intervention) Trial. It started in 1972, looking at 12,866 men with high risk for heart disease and followed them over seven years. All of them were placed on caloric restricted low fat diets and encouraged to exercise. It demonstrated that low fat diets and exercise FAILED to reduce weight or stop coronary artery disease in 100% of the cases. Don’t believe me? Read it for yourself (JAMA. 1982; 248 (12):1465-1477).
The second of these trials was the Women’s Health Initiative (WHI). This study started in 1991 and followed 48,835 women (yes, that’s a small city of women) for eight years. They didn’t believe the MRFIT results apparently, so they had a low fat (caloric restricted) arm and a control arm [the SAD diet (Standard American Diet)]. The women on the low fat arm lost a whooping 0.4 kg over the 8 year period (JAMA. 2006 Jan 4;295(1):39-49). 0.4 kg, really!?? That’s almost an entire pound of weight loss over 8 years. Quick, call Barnes & Noble so we can package that diet and sell it on Opra!! (Oh, wait, the news media was a little embarrassed by the findings and never really mentioned them.)
Lastly, if research on 60,000 men and women wasn’t enough to demonstrate what most primary care physicians seen in their offices daily, we had to do the Look AHEAD Study (Action for Health in Diabetes). This study started in 2001 and was supposed to run for 13.5 years. It studied 5,145 Type II diabetic patients with intensive lifestyle intervention. These patients were placed on intensive caloric and fat restriction of 1200-1800 calories per day with exercise and behavioral counseling. It was so unsuccessful, that they stopped the trial at 9.6 years – cause it wasn’t working.
The patients did lose some weight through Look AHEAD . . . an average of 6% of their body fat (That means you would have lost 15.6 lbs over 9 years if you weighed 260 lbs. Successful? . . . NOT). What made this trial worse is that it didn’t improve risk for coronary artery disease and people didn’t live longer (N Engl J Med 2013; 369:145-154). They just got the exciting chance to eat cardboard for 9 years of their lives. Sad. Very sad.

So, what does all this mean? Exercising your brains out at an expensive gym every morning won’t do much more than help you loose 1% of your body fat. It won’t increased your life span and it won’t decrease your risk of heart disease, despite what Dr. Ornish said. If you like spending $40 per month just to stare at sweaty fat bodies jumping up and down in spandex, by all means, please keep going to the gym. But I’d much rather spend that $40 on a nice rib eye steak at a restaurant staring at my wife. But, the benefits of saturated fat . . . that’s for another post.
Don’t get me wrong. I love lifting weights. I love riding my horse. I truly enjoy working in my yard. I even enjoy riding my bicycle. But I do these things now because they bring me peace, decrease my stress, and allow me to connect with nature. Believe me, there’s nothing natural about a 250 pound man in spandex staring at himself in a mirror repetitively lifting 30 pound bars of iron. But, we won’t go there.
My friends, and a few of my patients, get their knickers in a wad trying to decry the fact that I’m giving people a reason not to go running. Maybe I am. To be honest, there’s really only one reason I want to run, . . . and that’s when I’m being chased by a bear. But what good does it do to guilt a person into participation in an activity that isn’t really benefiting their health or help them lose weight, unless they really truly enjoy the activity for the sake of the activity?
Our health is not based upon a caloric scale of inputs and outputs. We are hormonal machines. We gain or lose weight and we gain or lose muscle based on powerful hormone signals, specifically insulin. Simple carbohydrate restriction has profound effects upon our weight, blood pressure, cholesterol and inflammatory states. Until we each come to grips with the fact that the food we eat triggers hormone responses in our bodies, we will continue down the path of diseases of civilization. Hippocrates summed it up when he said, “Let food be thy medicine, and let medicine be thy food.”
Tiffini’s Fat Bombs
There are a number of recipes for “Fat Bombs” on the internet, but this one is my wife’s version. These have been a lifesaver for starting and maintaining a Low-Carbohydrate or Ketogenic diet over the last few years. They are fantastic mid-meal or anytime Low-Carb snacks, full of satiating fat, that really help during the holidays. I mentioned Fat Bombs to my patients in my Low-Carb Group Visit Class today and I promised to post them here:

Fat Bombs:
1 stick of real Butter softened
1 cup Coconut Oil
1/2-2/3 cup Erythritol
1 tsp liquid Stevia
1/3 cup Cocoa Powder
1 cup Peanut Butter or Almond Butter
2 cups chopped Macadamia Nuts or slivered Almonds
1-2 cups of Coconut
Mix together and place 1-2 table spoon sized scoops in small muffin tin or on wax paper. Must be kept refrigerated to remain firm.
Enjoy!!
Don't Fear Fat
Don’t fear the fat. If you haven’t seen the movie Cereal Killers, you should watch it by clicking here. D.J. O’Neill ditches wheat and sugar in a food plan consisting of 70% fat – under the guidance of legendary South African Sports Scientist Prof. Tim Noakes.
101 Uses for Bacon . . .

Relapse
 Did you fall off the low-carbohydrate wagon this week? Did those donuts just call out your name as you walked by the bakery in the grocery store? Maybe you feel like you were shot out of the carbohydrate cannon, landing in the nearby Potato County? If so, you probably had a relapse. You were doing so well, then all the sudden, your will-power caved.
Did you fall off the low-carbohydrate wagon this week? Did those donuts just call out your name as you walked by the bakery in the grocery store? Maybe you feel like you were shot out of the carbohydrate cannon, landing in the nearby Potato County? If so, you probably had a relapse. You were doing so well, then all the sudden, your will-power caved.
Relapse is not uncommon when making a dietary lifestyle change. What causes relapse? I often see people relapse back to the Standard American Diet, the SAD diet, because of a number of reasons.

First, it is important to recognize that there are a milieu of neuro-hormones that drive hunger cravings or suppression. Anything that triggers a change in these hormone levels can cause the carbohydrate cravings to kick in . . . and you find yourself stuffing yourself with “carbage.”
Second, is boredom. Many people find an increased nervousness when they get bored. They find that eating, with it’s calming parasympathetic nervous system effect, diminish the nervousness that arises out of boredom. They often create a near Pavlov’s type trigger to eat when they experience boredom and it is quickly interpreted as hunger. There is actually a release of endorphin associated with eating and chewing that suppresses stress and or anxiety. Reduction of stress, exercise, and journal writing have been found to help patient’s reduce the food cravings associated with boredom. It is important to have “rescue foods” like string cheese, a handful of almonds, beef jerky, or “fat bombs” available that can be used when you experience these symptoms.
Following the line of triggers, Pavlov demonstrated that repeated actions associated with rewarding consequences will form a physiologic trigger. Frequently. our desire to eat carbohydrates (“carb cravings”) are often tied to triggers. For example, growing up in my home as a child, our family frequently would relax by watching prime-time television while eating a large bowl of popcorn and a Pepsi. To this day, whenever I turn on the television in the evening, I get cravings for carbohydrates. It is important to look at what you were doing or what was going on around you at the time the craving occurred. Substitution of foods has helped to solve these cravings by replacing the popcorn and Pepsi with pork rinds and Diet Dr. Pepper. (Don’t cringe, pork rinds and guacamole tastes fantastic and is a very low carbohydrate substitute that works for me.)
Lastly, many patients fall off the wagon when they visit or have a meal with family. They are often made to feel guilty if they don’t eat Aunt Velda’s homemade chocolate chip cookies. They are afraid of offending their relatives if they don’t partake of those tasty cookies. The challenge is that cheating by eating the cookies causes an insulin spike and leads to 24-72 hours of carbohydrate cravings thereafter. Are those cookies worth 72 hours of carbohydrate cravings? Maybe. But it is important to consider helping Aunt Velda to understand what those cookies will do to you, and that you still care for Aunt Velda even if you don’t eat her chocolate chip cookies.
In many families, food is often associated with love. “If you don’t eat the food I made for you, you don’t really love me” is an underlying tone that can be found in many family dynamics that I see in my office. Some times bringing your own low-carb chocolate chip cookies, and offering one to Aunt Velda, will stimulate a conversation about your dietary changes and diffuse the guilt and offence that might arise.
Often, knowing what will cause you to fall off the wagon, helps to keep you on the wagon. What challenges have you had staying on the wagon?
Stress . . . . The Weight Loss Killer
Has your weight loss plateaued? Are you struggling to meet your weight loss goals? Have you struggled to lose weight in spite of doing everything “correctly?” Are you still struggling with those last few pounds?
You’re not alone. Many of my patients, myself included, have found themselves “stuck” in their weight loss progression. There are a number of reasons you may not be loosing weight, but one that I am seeing more and more frequently is “Pseudo-Cushings’s Syndrome.” Pseudo-Cushing’s Syndrome is a physiologic
hypercortisolism (high level of cortisol) that can be caused by a number of problems:
- Physical stress
- Severe bacterial or fungal infection
- Malnutrition or Intense chronic exercise
- Psychological stress – including untreated or under-treated depression, anxiety, post-traumatic stress, or dysthymia (chronic melancholy)
- Alcoholism
The psychiatric literature suggest that up to 80% of people with depressive disorders have increased cortisol secretion (1,2,3). 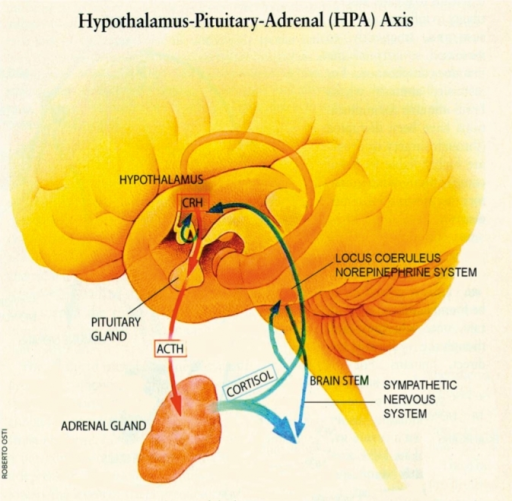 People with significant stressors in their life have been show to have a raised cortisol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing an over production of cortisol and normalization of their cortisol levels occurs after resolution of the stressor. This cortisol response is not high enough to lead to a true Cushing’s Syndrome, but effects ones ability to loose weight.
People with significant stressors in their life have been show to have a raised cortisol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing an over production of cortisol and normalization of their cortisol levels occurs after resolution of the stressor. This cortisol response is not high enough to lead to a true Cushing’s Syndrome, but effects ones ability to loose weight.
I suspect this is becoming more prevalent due to the high paced, high-stress, always on, plugged in, 24 hour information overload lives we live.
What is cortisol? It is a steroid hormone made naturally in the body by the adrenal cortex (outer portion of the adrenal gland). Cortisol is normally stimulated by a number of daily activities including fasting, awakening from sleep, exercise, and normal stresses upon the body. Cortisol release is highest in the morning, helping to wake us up, and tapers into the afternoon. Cortisol plays a very important role in helping our bodies to regulate the correct type (carbohydrate, fat, or protein) and amount of fuel to meet the bodies physiologic demands that are placed upon it at a given time (4,5,6).
 Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues and turns on the maturation process of adipocytes (fat cells). In the process, it suppresses the immune system to decrease inflammation during times of stress (7,8,9). In the short run, this is an important process, however, when cortisol production is chronically turned up, it leads to abnormal deposition of fat, increased risk of infection, impotence, abnormal blood sugars, head
Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues and turns on the maturation process of adipocytes (fat cells). In the process, it suppresses the immune system to decrease inflammation during times of stress (7,8,9). In the short run, this is an important process, however, when cortisol production is chronically turned up, it leads to abnormal deposition of fat, increased risk of infection, impotence, abnormal blood sugars, head
aches, hypertension and ankle edema, to name a few.
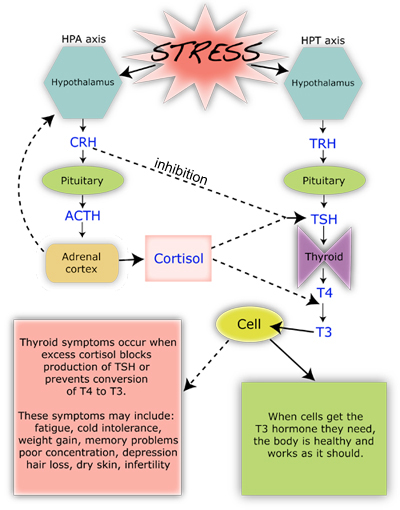
The chronic elevation in cortisol directly stimulates an increase in insulin by increasing the production of glucose in the body, and cortisol blockaids the thyroid axis. Both of these actions halt the ability to loose weight, and drive weight gain.
Cortisol also increases appetite (10). That’s why many people get significant food cravings when they are under stress (“stress eaters”). Cortisol also indirectly affects the other neuro-hormones of the brain including CRH (corticotrophin releasing hormone), leptin, and neuropeptide Y (NPY). High levels of NPY and CRH and reduced levels of leptin have also been shown to stimulate appetite (10-11).
How do you test for Pseudo-Cushing’s Disease?
Testing can be done by your doctor with a simple morning blood test for cortisol. If your cortisol is found to be elevated, it needs to be repeated with an additional 24 hour urine cortisol measurement to confirm the diagnosis. If Cushing’s Syndrome is suspected, some additional blood testing and diagnostic imaging will be necessary.
How do you treat it?
First, the stressor must be identified and removed. Are you getting enough sleep? Is there an underlying infection? Is there untreated anxiety or depression present? Are you over-exercising? These things must be addressed.
Second, underlying depression or anxiety can be treated with counseling, a variety of weight neutral anti-depressant medications or a combination of both. Many of my patients find that meditation, prayer, and journaling are tremendous helps to overcoming much of the anxiety and depression they experience.
Third, adequate sleep is essential. Remove the television, computer, cell phone, iPad or other electronic distraction from the bedroom. Go to bed at the same time and get up at the same time each day. Give yourself time each day away from being plugged in, logged in or on-line.
Fourth, mild intensity (40% of your maximal exertion level) exercise 2-3 days a week was found to lower cortisol; however, moderate intensity (60% of your maximal exertion level) to high intensity (80% of your maximal exertion level) exercise was found to raise it (12). A simple 20 minute walk, 2-3 times per week is very effective.
So, the take home message . . . It’s not the stress that’s killing us, it’s our reaction to it.
References:
- Pfohl B, Sherman B, Schlechte J, Winokur G. Differences in plasma ACTH and cortisol between depressed patients and normal controls. Biol Psychiatry 1985; 20:1055.
- Pfohl B, Sherman B, Schlechte J, Stone R. Pituitary-adrenal axis rhythm disturbances in psychiatric depression. Arch Gen Psychiatry 1985; 42:897.
- Gold PW, Loriaux DL, Roy A, et al. Responses to corticotropin-releasing hormone in the hypercortisolism of depression and Cushing’s disease. Pathophysiologic and diagnostic implications. N Engl J Med 1986; 314:1329.
- Ely, D.L. Organization of cardiovascular and neurohumoral responses to stress: implications for health and disease. Annals of the New York Academy of Sciences (Reprinted from Stress) 771:594-608, 1995.
- McEwen, B.S. The brain as a target of endocrine hormones. In Neuroendocrinology. Krieger and Hughs, Eds.: 33-42. Sinauer Association, Inc., Massachusetts, 1980.
- Vicennati, V., L. Ceroni, L. Gagliardi, et al. Response of the hypothalamic- pituitary-adrenocortical axis to high-protein/fat and high carbohydrate meals in women with different obesity phenotypes. The Journal of Clinical Endocrinology and Metabolism 87(8) 3984-3988, 2002.
- Wallerius, S., R. Rosmond, T. Ljung, et al. Rise in morning saliva cortisol is associated with abdominal obesity in men: a preliminary report. Journal of Endocrinology Investigation 26: 616-619, 2003.
- Epel, E.S., B. McEwen, T. Seeman, et al. Stress and body shape: stress-induced cortisol secretion is consistently greater among women with central fat.
Psychosomatic Medicine 62:623-632, 2000. - Tomlinson, J.W. & P.M. Stewart. The functional consequences of 11_- hydroxysteroid dehydrogenase expression in adipose tissue. Hormone and Metabolism Research 34: 746-751, 2002.
- Epel, E., R. Lapidus, B. McEwen, et al. Stress may add bite to appetite in women: a laboratory study of stress-induced cortisol and eating behavior.Psychoneuroendocrinology 26: 37-49, 2001.
- Cavagnini, F., M. Croci, P. Putignano, et al. Glucocorticoids and neuroendocrine function. International Journal of Obesity 24: S77-S79, 2000.
- Hill EE, Zack E, Battaglini C, Viru M, Vuru A, Hackney AC. Exercise and circulating cortisol levels: the intensity threshold effect. J Endocrinol Invest. 2008. Jul;31(7):587-91.
The Obesity Paradox: The Intersection Where Agricultural Policy Contradicts Health Policy
Intent
The intent of this brief is to analyze the burden of obesity in the United States and to recommend policy changes to reduce the medical costs of obesity imposed upon the individual and country as a whole.
Introduction
Conventional fat reduction/caloric restriction guidelines for the treatment of obesity and associated cardiovascular disease, diabetes, cancer, and hypertension have been recommended since the early 1970’s. Because these guidelines are based on questionable evidence, the cost of obesity has dramatically risen to almost 21% of overall health care costs in the United States (1). This brief will analyze the current medical cost of obesity and will explain why the current obesity reduction guidelines perpetuate the problem. In addition, the brief will examine the impact of government agricultural policy on dietary habits, and will recommend changes to farm subsidy legislation in order to reduce the incidence of obesity and decrease costs to the healthcare system.
History & Background
The Cost of Obesity on the Nation
 As of 2012, obesity accounts for nearly 21% of overall health care costs in the United States. An obese person incurs $2741 more in medical expenses per year than his or her non-obese counterpart (1). Medicare spending has increased per person per year by $600 for each obese beneficiary (includes out-patient and prescription drugs) and Medicaid beneficiary prescription drug spending increased by $230 per year per obese person. Private insurance has increased by $248 for prescription drugs and $443 for in-patient services for each obese beneficiary per year (2). That adds up to $190.2 billion spent annually on obesity-related medical problems (3). This is a drastic change. Health care costs related to obesity were $85.7 billion (9.1% of overall health care costs) in 2006 and $61.2 billion (6.5% of overall health care costs) in 1998 (4).
As of 2012, obesity accounts for nearly 21% of overall health care costs in the United States. An obese person incurs $2741 more in medical expenses per year than his or her non-obese counterpart (1). Medicare spending has increased per person per year by $600 for each obese beneficiary (includes out-patient and prescription drugs) and Medicaid beneficiary prescription drug spending increased by $230 per year per obese person. Private insurance has increased by $248 for prescription drugs and $443 for in-patient services for each obese beneficiary per year (2). That adds up to $190.2 billion spent annually on obesity-related medical problems (3). This is a drastic change. Health care costs related to obesity were $85.7 billion (9.1% of overall health care costs) in 2006 and $61.2 billion (6.5% of overall health care costs) in 1998 (4).
 The most recent Center for Disease Control statistics reveal that 35.7% of the U.S. adult population is currently obese and another 33% is overweight. Over 78 million adults and 12.5 million children are obese (5). The addition of 30 million people to the health care roles (current estimation of the Affordable Care Act including Medicaid expansion) means that an estimated $27 billion (in 2012 dollars) more will be spent per year on obesity-related health care costs.
The most recent Center for Disease Control statistics reveal that 35.7% of the U.S. adult population is currently obese and another 33% is overweight. Over 78 million adults and 12.5 million children are obese (5). The addition of 30 million people to the health care roles (current estimation of the Affordable Care Act including Medicaid expansion) means that an estimated $27 billion (in 2012 dollars) more will be spent per year on obesity-related health care costs.
Impact of Government Policy on Consumption
The ‘Farm Bill’ was originally enacted as part of President Franklin D. Roosevelt’s Agricultural Adjustment Act of 1933, which provided subsidies to American farmers in the midst of the Great Depression. Since that time the federal government has paid farmers not to grow seven specific crops – known as commodities – with the intent of decreasing the supply, increasing the demand, and thereby raising the price (7). Dr. Susan Blumenthal, former Assistant Surgeon General and current SNAP to Health project director, writes, “The Farm Bill has since expanded to include many different categories or ‘titles.’ The last bill to be authorized, in 2008, had 15 titles, including nutrition (food stamps), crop subsidies, conservation, livestock, crop insurance and disaster assistance. The 2008 Farm Bill approved $300 billion in spending: 67% was spent on food stamps; 15% on agricultural subsidies; 9% on conservation; and 8% on crop insurance” (8).
The U.S. Department of Agriculture (USDA) Subsidy Programs tend to favor, either directly or indirectly, foods that increase obesity and other diseases. These subsidies support commodity crops, specialty crops, dairy products, livestock, and federal purchase programs. Their justification is that they help to stabilize prices in agricultural commodity markets by balancing supply and demand (9). Between 1995 and 2011, $277.3 billion were given in farm subsidies to almost 40% of U.S. farmers. Arizona received $1.1 billion (mainly for cotton); however, only 7% of Arizona farms received subsides during this period (10). These subsidies are incentives to grow and produce specific commodities that have a higher monetary return. Subsidies also act as a disincentive for farmers to grow fruits and vegetables which fall under the “specialty crops” category. This restricts both small and large farmers from diversifying their crops, and limits fruit and vegetable production (11).
Arizona farms received $25.3 million in dairy subsidies from 1995-2011 and $29.5 million in livestock subsidies during that same period (9). Arizona ranks 2nd nationally in its production of cantaloupe & honeydew melons, head & leaf lettuce, spinach, broccoli, cauliflower and lemons, all of which are “specialty crops” and do not receive subsidies (12). The most recent statistics show that the top five states receiving subsidies are Iowa, Texas, Illinois, Nebraska and Minnesota, with Kansas coming in at a close sixth. The majority of these subsidies are for corn ($81.7 billion), soybeans ($26.4 billion), rice ($13.3 billion) and wheat ($34.4 billion) from 1995-2011 (10). It is important to note that the Renewable Fuel Standard of 2012 (legislation protecting the corn-ethanol lobby) mandates that 37% of the corn harvest be used in ethanol production (13).
The food subsidies above have been in place since the Food, Conservation & Energy Act of 2002 and renewed in 2008. They were only to be available for a period of five additional years and were set to expire September 30, 2012. However, the American Taxpayer Relief Act of 2012 (H.R. 8), enacted by Congress and signed into law by President Barack Obama, included provisions that extended these subsidies until September 30, 2013 (20).
For many low-income Americans and especially children, federal programs have a direct and significant influence on food choices.  Over 30 million children receive government subsidized school lunch through National School Lunch Program (NSLP) administered by the USDA Food and Nutrition Service (14). USDA-purchased meats, dairy products, grains, fruits, and vegetables are supplied to schools for use in meal programs. Current school lunch recommendations on calorie intake set by the USDA and The Healthy, Hunger-Free Kids Act of 2010mandate school lunches provide 650-850 calories per meal to the 30 million children currently enrolled in this program (15). Interestingly, that is the same caloric count of a Big Mac®, small fry and Diet Coke® from McDonalds® (16). The rational for these purchase decisions are based upon agricultural support goals and adherence to national dietary guidelines (14). A study published in the journal Economics and Human Biology reveals that a person’s body mass index (BMI) increased faster if that personwere on food stamps, and the BMI increased at a faster rate while on the Supplemental Nutrition Assistance Program (SNAP). “We can’t prove that the Food Stamp Program causes weight gain, but this study suggests a strong linkage,” said Jay Zagorsky, co-author of the study and a research scientist at Ohio State University’s Center for Human Resource Research (17). However, much of the food available through the SNAP programs are refined, subsidized high-carbohydrate containing foods.
Over 30 million children receive government subsidized school lunch through National School Lunch Program (NSLP) administered by the USDA Food and Nutrition Service (14). USDA-purchased meats, dairy products, grains, fruits, and vegetables are supplied to schools for use in meal programs. Current school lunch recommendations on calorie intake set by the USDA and The Healthy, Hunger-Free Kids Act of 2010mandate school lunches provide 650-850 calories per meal to the 30 million children currently enrolled in this program (15). Interestingly, that is the same caloric count of a Big Mac®, small fry and Diet Coke® from McDonalds® (16). The rational for these purchase decisions are based upon agricultural support goals and adherence to national dietary guidelines (14). A study published in the journal Economics and Human Biology reveals that a person’s body mass index (BMI) increased faster if that personwere on food stamps, and the BMI increased at a faster rate while on the Supplemental Nutrition Assistance Program (SNAP). “We can’t prove that the Food Stamp Program causes weight gain, but this study suggests a strong linkage,” said Jay Zagorsky, co-author of the study and a research scientist at Ohio State University’s Center for Human Resource Research (17). However, much of the food available through the SNAP programs are refined, subsidized high-carbohydrate containing foods.
The price of food influences an individual’s consumption choices (6). Foods that are refined contain increased amounts of sugar or high-fructose corn syrup. These foods contain more caloric density and are often cheaper and more easily accessible. These are foods that are usually found in the center of the grocery store and frequently on sale at the end-caps of each isle. Nutrient-dense, higher fiber foods are frequently associated with higher prices and are consumed less often. These are the foods you usually find around the peripheral areas of the grocery store (fruits, vegetables, etc.) Current food subsidy policy found in the Food, Conservation and Energy Act of 2008 extension mandated by the American Taxpayer Relief Act of 2012 drives up the price of fruits, vegetables, and meats. This policy also turns people toward lower cost foods that are higher in simple carbohydrates and caloric density. Thus, current policy is actually making obesity worse and making America fatter. Research completed at the University of Illinois at Chicago reveals that small taxes or price changes do not produce a change in a person’s BMI; however, more significant price change has a measurable and significant effect on weight in both adults and children. Price increases of 100-150% have been shown to change purchasing behavior and thereby affect health (18). An example of this is the tax levied on cigarette smoking.
The USDA disagrees with the amount of influence they have over the individual American’s food choices. They state openly on their website that “Some public health advocates have argued that falling real, or inflation-adjusted, prices for many high-calorie foods encourage people to buy and consume more of these foods, leading to poor diet quality and rising rates of obesity. A closer look at how consumers respond to food price variation–over time, across geographic markets, in different types of stores, and in response to taxes and subsidies–reveals how food prices affect people’s food choices, and their waistlines. In short, price matters, but not very much, and it is not the only factor” (19).
Why Current Dietary Guidelines Have Not Been Effective
Why do we get fat? Why have we not been successful in losing weight via diet and exercise? The obesity paradox was described by Jules Hirsch of Rockefeller University, who proposed two opposing hypotheses:
- “Obesity is the result of a willful descent into self-gratification” implying that we gain weight because we over-eat (caloric excess) leading to caloric imbalance.
- “Alternative hypothesis is that there is something ‘biologic’ about obesity, some alteration of hormones, enzymes or other biochemical control systems which leads to obesity” (22).
The 1977 Dietary Goals for the United States – the first comprehensive statement by any branch of the federal government about the American diet – supported the first theory. The Guidelines were heavily influenced by the American Heart Association’s position that fat intake alone would cause heart disease. The USDA 2011 Dietary Guidelines imply that the “people who are the most successful at achieving and maintaining a healthy weight do so through continued attention to consuming only enough calories from foods and beverages to meet their needs and by being physically active.” (15)
Current research contradicts the caloric restriction or “calorie in – calorie out” theory. Scientific evidence clearly demonstrates the domino effect of carbohydrate or starch intake increasing insulin levels which thereby stimulates obesity by raising cholesterol and triglyceride levels. Time Magazine recently published evidence that the longstanding recommendations to “eat less high-fat red meat, eggs and dairy and replace them with more calories from fruits, vegetables and especially carbohydrates” is now seen as incorrect (45). Even our medical textbooks from 1965, like the introductory chapter of the Handbook of Physiology, make it clear that carbohydrate intake cause weight gain and raise triglyceride and cholesterol levels (22), (23), (24).
Current Policy
The current version of the Farm Bill was set to expire September 30th, 2013. If it had been allowed to expire, the results would have returned us to the 1949 Farm Bill legislation and theoretically double the price of milk. However, this would have had the effect of freeing up over $5 billion dollars of federal spending per year and would also lead to decreased consumption of a major source of carbohydrates in the standard American diet like wheat and corn. Senator Debbie Stabenow (D-MI), and chairwoman of the Senate Agriculture Committee, had repeatedly said she was opposed to an extension; however, she agreed to a compromise extending the bill for another year to help the farmers experiencing serious drought conditions in 2012 (7). Two additional extensions were passed in the House and Senate, but because these differed so significantly, it was referred to a House-Senate Conference Committee to work out the compromise details. With only $23 billion in spending reductions, The Agricultural Act of 2014 was passed on January 29, 2014 (46).
Outcomes and Stakeholders
 If the United States continues its current course, up to 58% of the population will be obese by 2030 (26). Many believe that the USDA Dietary Guidelines are to blame. Richard David Feinman, President of the Nutrition and Metabolism Society and Professor of Cell Biology at SUNY Downstate Medical Center said, “The previous Guidelines have not worked well. It is unreasonable to ask the Dietary Guidelines Advisory Committee (DGAC) to audit its own work. An external panel of scientists with no direct ties to nutritional policy would be able to do a more impartial evaluation of the data. This would be far better for everyone.” (27) A recent Gallup Poll reveals that 63% of Americans believe the USDA Guidelines that a low fat, calorie restricted diet will help in reduction of obesity, and the same study showed that 48% of Americans worry about their weight “all of the time or some of the time” (28). Recent evidence from the Women’s Health Initiative Dietary Modification Trial studying 49,000 women supports Dr. Feinman’s conclusion above. It did not show any statistically significant evidence that following a low-fat or caloric restricted diet had any effect upon obesity (29). Other nutritional experts from the Salt Institute and the National Health Coalition have expressed their support for significant changes to the USDA Dietary Guidelines (30). The Weston A. Price Foundation, which according to its website is “dedicated to restoring nutrient-dense foods to the human diet through education, research and activism,” also supports the view that the current USDA Dietary Guidelines have been a significant cause of obesity and have been an active voice promoting legislative change (31).
If the United States continues its current course, up to 58% of the population will be obese by 2030 (26). Many believe that the USDA Dietary Guidelines are to blame. Richard David Feinman, President of the Nutrition and Metabolism Society and Professor of Cell Biology at SUNY Downstate Medical Center said, “The previous Guidelines have not worked well. It is unreasonable to ask the Dietary Guidelines Advisory Committee (DGAC) to audit its own work. An external panel of scientists with no direct ties to nutritional policy would be able to do a more impartial evaluation of the data. This would be far better for everyone.” (27) A recent Gallup Poll reveals that 63% of Americans believe the USDA Guidelines that a low fat, calorie restricted diet will help in reduction of obesity, and the same study showed that 48% of Americans worry about their weight “all of the time or some of the time” (28). Recent evidence from the Women’s Health Initiative Dietary Modification Trial studying 49,000 women supports Dr. Feinman’s conclusion above. It did not show any statistically significant evidence that following a low-fat or caloric restricted diet had any effect upon obesity (29). Other nutritional experts from the Salt Institute and the National Health Coalition have expressed their support for significant changes to the USDA Dietary Guidelines (30). The Weston A. Price Foundation, which according to its website is “dedicated to restoring nutrient-dense foods to the human diet through education, research and activism,” also supports the view that the current USDA Dietary Guidelines have been a significant cause of obesity and have been an active voice promoting legislative change (31).
On the other hand, the Sugar Association has issued statements that sugar is not the cause of obesity and “continually eating too much food and sedentary lifestyles are the major contributing factors to increasing rates of obesity – not sugar intake” (32). In addition, the American Beverage Association has stated that sugars are not the problem with obesity, but instead, “overweight and obesity are a result of an imbalance between calories consumed and calories burned” (33).
Attempts at modifying the Farm Bill with legislation like the 2012 DeMint Amendment (SA 2276 ) were supported by both Arizona Senators McCain (R-AZ) and Kyl (R-AZ) with a “Yes” vote, as well as Senators Ayotte (R-NH), Brown (R-MA), Burr (R-NC), Coats (R-IN), Coburn (ROK), Cornyn (R-TX), DeMint (R-SC), Graham (R-SC), Hatch (R-UT), Heller (R-NV), Johnson (R-WI), Lee (R-UT), McConnell (R-KY), Murkowski (R-AK), Paul (R-KY), Rubio (R-FL), Sessions (R-AL), and Toomey (R-PA). However, because of a large lobbying agricultural coalition, it was voted down (34). Changing farm subsidies will be a great challenge as 40% of the farmers in the U.S. now have some degree of dependence upon these subsidies. The following agricultural groups have historically had significant monetary interest in the farm subsidies that these amendments would affect:
- American Beekeeping Federation
- American Farm Bureau Federation American Mushroom Institute
- American Sheep Industry Association American Soybean Association
- National Cattlemen’s Beef Association National Corn Growers Association National Cotton Council
- National Council of Farmer Cooperatives National Farmers Union
- National Milk Producers Federation National Pork Producers Council
- National Potato Council
- National Sorghum Producers
- National Watermelon Association
- Produce Marketing Association
- United Dairymen of Arizona
- United Egg Producers
- United Fresh Produce Association
- Western Peanut Growers Association
The following groups have formed coalitions in support of the Farm Bill: Health/Food Justice/Farm Group partnerships, Specialty Crop Farm Bill Alliance, Community Food Security Coalition, Center for a Livable Future at Johns Hopkins University, Collaboration for a Healthy Sustainable Food System, and the Healthy Farms, Healthy People: A Farm & Food Policy Summit for a Strong America.
The American Heart Association’s position is that the Farm Bill needs to be modified to include increased access to fruits and vegetables (35). The American Medical Association’s position in 2008 and 2011 has been for cutting the size and budget of the current Farm Bill (36). The American Osteopathic Association does not currently have a formal position on the Farm Bill.
If certain crops like corn or wheat were no longer subsidized,drastic changes will be likely in the food manufacturing industry, which would likely be the largest proponent against change. Unintended consequences of modifying the Farm Bill and not extending its subsidies could have the short term effect of escalating the price of a number of commodities to two to three times their current price. For example, the price of milk would increase to $6-$8 dollars a gallon without federal subsidies (37). This would likely deter the use of carbohydrates containing dairy products, but may also increase the price of meats and cheeses as well.
The USDA’s Rural Development Progress Report claims that the subsidies it distributed “saved more than 75,000 jobs” in 2006 and over 400,000 jobs in 2011 (38), (39). They claim that without federal farm subsidiesthere would be significant loss of jobs; however, studies from the Cato Institute actually show the opposite.
“Job gains are weak and population growth is actually negative in most of the counties where farm payments are the biggest share of income. Job growth is decidedly weak in the counties most dependent on farm payments. The vast majority of such counties (483) had job gains below the 19 percent national average from 1992 to 2002. A considerable number (167) had outright job losses over the period. In short, farm payments are not yielding robust economic and population gains in the counties where they should have the greatest impact. If anything, the payments appear to be linked with sub-par economic and population growth. To be sure, this quick comparison cannot answer whether growth would have been even weaker in the absence of the payments. Still, farm payments appear to create dependency on even more payments, not new engines of growth” (40).
As of 2010, obesity costs about $73.1 billion per year in lost productivity in the United States (43). The worsening obesity epidemic poses further workforce productivity losses up to 20% more by 2030. Even small improvements in obesity will improve workforce productivity and has substantial potential for savings. Currently, the Affordable Care Act allows employers to charge obese employees 30-50% more for health insurance. Without correcting this epidemic, it may be impossible for many to afford health care, opting out to pay the less expensive tax penalty. This would have the effect of increasing commercial premiums across the country, feasibly pushing private insurance companies out of business and forcing a single payer governmental system.
Recommendations
This brief points out that the overall U.S. healthcare costs associated with obesity have increased by 68% in the last fourteen years. It provides evidence that using current dietary low-fat caloric restriction guidelines show poor statistically significant improvements in obesity. And it provides evidence that obesity is not caused by excessive caloric intake and fat, but by insulin response to carbohydrate intake. Lastly, this analysis provides evidence that the Farm Bill propagates continued worsening obesity rates in the US by providing access to cheap, fattening food.
The USDA 2011 Dietary Guidelines need to be revised to reflect current evidence-based obesity prevention and weight reduction research. The guidelines should include information about limiting the intake of foods high in carbohydrates.
The food subsidy extension provided in the American Taxpayer Relief Act of 2012 was extended five years by the Agricultural Act of 2014. Had it been allowed to expire, it would have saved the country over $200 billion over the next ten years. However, because of so many entitlements involved in this bill, the House and Senate convened in Conference that resulted in a compromise of only $23 billion dollars in spending reductions, the first SNAP reforms since 1996 reducing waste, but did nothing in eliminating subsidies that drive or influence eating behavior (46).
When significant price changes occur, eating behavior will change. As the price of fattening carbohydrates increases, people will eat less of them, leading to a national decrease in obesity and overweight. The current reforms did nothing that will change our dietary behavior.
References
1. Cornell University. Obesity accounts for 21 percent of U.S. health care costs, study finds. Science Daily. [Online] April 9, 2012. [Cited: January 5, 2013.] http://www.sciencedaily.com/releases/2012/04/120409103247.htm.
2. Annual Medical Spending Attributable To Obesity: Payer-And Service-Specific Estimates. Eric A Finkelstein, Justin G Trogdon, Joel W Cohen and William Dietz. Health Affairs, 28, Bethesda, MD : Project HOPE, 2009, Vol. 5. 10.1377/hlthaff.28.5.w822.
3. Begley, Sharon. As America’s Waistline Expands, Costs Soar. Reuters. [Online] Thompson Reuters, April 30, 2012. [Cited: January 5, 2013.] http://www.reuters.com/article/2012/04/30/us-obesity-idUSBRE83T0C820120430.
4. Ungar, Rick. Obesity Now Cost Americans More In Healthcare Spending Than Smoking. Forbes. [Online] 4 30, 2012. [Cited: January 5, 2013.] http://www.forbes.com/sites/rickungar/2012/04/30/obesity-now-costs-americans-more-in-healthcare-costs-than-smoking/.
5. Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesity in the United States, 2009–2010. NCHS data brief, no 82. Hyattsville, MD : National Center for Health Statistics, 2012, 2012.
6. Poverty and Obesity: The Role of Energy Density and Energy Costs. A Drewnowski, SE Specter. s.l. : American Journal of Clinical Nutrition, 2004, Vols. 79:6-16.
7. Laprete, Jay. U.S. Farm Bill. Times Topics. [Online] The New York Times, December 31, 2012. [Cited: February 11, 2013.] http://topics.nytimes.com/top/reference/timestopics/subjects/f/farm_bill_us/index.html?offset=0&s=newest.
8. SNAP to Health. U.S. Farm Bill: Frequently Asked Questions. SNAP to Health. [Online] CSPC / Snap to Health, 2013. [Cited: February 11, 2013.] http://www.snaptohealth.org/farm-bill-usda/u-s-farm-bill-faq/.
9. USDA. Agricultural Marketing Service. Commodity Purchasing. [Online] January 22, 2013. [Cited: February 10, 2013.] http://www.ams.usda.gov/AMSv1.0/ams.fetchTemplateData.do?template=TemplateQ&navID=Commodity%20Purchasing%20Main%20Page&rightNav1=Commodity%20Purchasing%20Main%20Page&topNav=&leftNav=CommodityPurchasing&page=CommodityPurchasing&resultType=&acct=cmdtyprchs.
10. Environmental Working Group. United States Summary Information. EWG Farm Subsidies. [Online] 2012. [Cited: February 10, 2013.] http://farm.ewg.org/region.php?fips=00000.
11. Monke, Jim. Farm Commodity Programs: Base Acreage and Planting Flexibility. Washington, DC : Congressional Research Services, 2003.
12. Arizona Farm Bureau Federation. AG Facts. Arizona Farm Bureau. [Online] 2013. [Cited: February 15, 2013.] http://www.azfb.com/ag-facts.html.
13. Children of the Corn: The Renewable Fuels Disaster. The American. [Online] American Enterprise Institute, January 4, 2012. [Cited: February 15, 2013.] http://www.american.com/archive/2012/january/children-of-the-corn-the-renewable-fuels-disaster.
14. USDA Food & Nutrition Service. National School Lunch Program. USDA Food & Nutrition Serivce. [Online] June 21, 2012. [Cited: February 15, 2013.] http://www.fns.usda.gov/cnd/lunch/.
15. U.S. Department of Agriculture (USDA). USDA 2010 Dietary Guidelines. USDA Center for Nutrition Policy and Promotion: Dietary Guidelines for Americans. [Online] U.S. Government Printing Office, January 31, 2011. [Cited: January 5, 2013.] http://www.cnpp.usda.gov/Publications/DietaryGuidelines/2010/PolicyDoc/Chapter2.pdf.
16. ABC News. ABC News. Medical Unit. [Online] ABC News Internet Ventures, September 30, 2012. [Cited: April 14, 2013.] http://abcnews.go.com/blogs/health/2012/09/30/school-lunch-showdown-850-calorie-meals-compared/.
17. Ohio State University. Food Stamp Use Linked To Weight Gain, Study Finds. Science Daily. [Online] August 12, 2009. [Cited: April 13, 2013.] http://www.sciencedaily.com /releases/2009/08/090810122139.htm.
18. Food Prices and Obesity: Evidence and Policy Implications for Taxes and Subsidies. L Powell, F Chalupka. 1, Illinois : The Milbank Quarterly by Wiley Periodicals Inc, 2009, Vol. 87.
19. Jessica Todd, Biing-Hwan Lin. Amber Waves Online Magazine. U. S. Department of Agriculture Economic Research Service. [Online] September 2012. [Cited: February 10, 2013.] http://www.ers.usda.gov/amber-waves/2012-september/what-role-do-food-and-beverage-prices.aspx.
20. American Taxpayer Relief Act of 2012. U.S. Government Printing Office. [Online] Jan 12, 2012. [Cited: February 10, 2013.] http://www.gpo.gov/fdsys/pkg/BILLS-112hr8enr/pdf/BILLS-112hr8enr.pdf.
21. Bruch, Hilde. The Importance of Overweight. Michigan : Norton, University of Michigan, 1957.
22. Taubs, Gary. Good Calories, Bad Calories: Fats, Carbs, and the Controversial Science of Diet and Health. New York : Anchor Books, 2007. 978-1-40000-3346-1.
23. Role of Insulin in Endgenous Hypertriglyceridemia. GM Reave, RL Lerner, MP Stern, JW Farquhar. s.l. : Journal of Clinical Investigation, 1967, Vols. 46(II):1756-67.
24. High-Carb Diets Questioned. Kolata, G. 235(4785):164, s.l. : Science, 1987, Vol. 9.
25. U.S. Department of Health and Human Services. The Surgeon General’s Call to Action to Prevent and Decrease Overweight and Obesity. Washington, D.C. : U.S. Government Printing Office, 2001.
26. Global Burden of Obesity in 2005 and Projections to 2030. T Kelly, W Yang, C-S Chen, K Reynolds and J He. 8 July 2008, New Orleans : International Journal of Obesity, 2008, Vols. 32, 1431–1437. doi:10.1038/ijo.2008.102.
27. In The Face Of Contradictory Evidence: Report Of The Dietary Guidelines For Americans Committee. Adele H Hite, Richard D Feinman, Gabriel E Guzman, Morton Satin, Pamela Schoenfeld, Richard J Wood. 10, s.l. : Nutrition, 2010, Vol. 26. DOI: 10.1016/j.nut.2010.08.012.
28. A Dugan, F Newport. Gallup Wellbeing. Gallup. [Online] August 17, 2012. [Cited: April 13, 2013.] http://www.gallup.com/poll/156710/americans-say-low-fat-diet-better-low-car.aspx.
29. Low-fat dietary pattern and weight change over 7 years: the Women’s Health Initiative Dietary Modification Trial. . Howard BV, Manson JE, Stefanick ML, et al. s.l. : JAMA, 2006, Vols. 295:39-49. doi:10.1001/jama.295.1.39.
30. Healthy Nation Coalition. Healthy Nation Coalition. Healthy Nation Coalition. [Online] Adrienne Larocque, PhD, 2012. [Cited: March 8, 2013.] http://www.forahealthynation.org/.
31. Judith McGeary, Esq. Legislative Updates. The Weston A. Price Foundation. [Online] December 11, 2012. [Cited: March 9, 2013.] http://www.westonaprice.org/legislative-updates/policy-update-farm-bill-and-gmos.
32. The Sugar Association. Sugar and Your Diet. Sugar.org. [Online] 2012. [Cited: March 9, 2013.] http://www.sugar.org/sugar-and-your-diet/caloric-intake.html.
33. American Beverage Association. Obesity. American Beverage Association. [Online] 2013. [Cited: March 9, 2013.] http://www.ameribev.org/nutrition–science/obesity/.
34. Library of Congress. S.Amdt.2276 to S.3240. Congress.Gov. [Online] March 8, 2013. [Cited: March 9, 2013.] http://beta.congress.gov/amendment/112th-congress/senate-amendment/2276.
35. The American Heart Association. Policy Brief – The Farm Bill. The American Heart Association. [Online] 2012. [Cited: April 14, 2013.] http://www.heart.org/idc/groups/heart-public/@wcm/@adv/documents/downloadable/ucm_429110.pdf.
36. AMA: Report of Reference Committee . Malechek, Lindsay. 2011.
37. Wolf, Jim. Senate, House agriculture committees in deal to avert milk price spike. Reuters. Sun, Dec 30, 2012, 2012.
38. USDA. USDA Rural Progress Report. USDA. [Online] December 2006. [Cited: April 14, 2013.] http://www.rurdev.usda.gov/rd/pubs/2005_06_Prog_Report.pdf.
39. —. USDA Rural Developement 2011 Progress Report. USDA Rural Developement. [Online] December 2011. [Cited: April 14, 2013.] http://www.rurdev.usda.gov/Reports/RD%20Progress%20Report%202011–Smallest(2).pdf.
40. Slivinski, Stephen. Rural Subsidies. Cato Institute. [Online] July 2009. [Cited: March 9, 2013.] http://www.downsizinggovernment.org/agriculture/rural-subsidies.
41. Obesity prevention: the role of policies, laws and regulations. Swinburn, Boyd A. New Zeland : BioMed Central Ltd., 208, Vol. 5:12. 10.1186/1743-8462-5-12.
42. Begley, Sharon. As America’ss Waistline Expands, Costs Soar. Reuters. [Online] Thompson Reuters, April 30, 2012. [Cited: January 5, 2013.] http://www.reuters.com/article/2012/04/30/us-obesity-idUSBRE83T0C820120430.
43. The Costs of Obesity in the Workplace. E Finkelstein, M DiBonaventura, S Burgess, B Hale. 10, Illinois : Lippincott Williams & Wilkins, 2010, Vol. 52. doi: 10.1097/JOM.0b013e3181f274d2.
44. Rudd Center For Food Policy & Obesity. Search Legislation Database. Yale Rudd Center. [Online] Rudd Center, 2013. [Cited: January 5, 2013.] http://www.yaleruddcenter.org/legislation/search.aspx.
45. Walsh, Bryan. “Ending The War on Fat.” TIME Magazine. June 12, 2014.
46. Lucas, Frank D. “Agricultural Act Summary.” House Agricultural Committee. [Online] Jan 29, 2014. [Cited June 28, 2014.] http:// http://agriculture.house.gov/farmbill
The Fat Storage Control Mechanism
The only way to successfully loose weight is to modify or turn off the mechanisms that stimulate fat storage. For years we have been told that this was just a problem of thermodynamics, meaning the more calories you eat, the more calories you store. The solution was, thereby, eat less calories or exercise more, or both. We are taught in school that a 1 gram of carbohydrate contains 4 kcal, 1 gram of protein contains 4 kcal, and 1 gram of fat contains 9 kcal.
It’s easy to see that if I’m going to limit my calories, cutting out fat is the first step. For the last 65 years, we as a society have been doing just that, cutting out fat, exercising more and eating fewer calories. What has it done for us? It’s made us fatter! (1)
Some may argue that we really aren’t eating fewer calories and exercising more. But most people I have seen in my office have tried and tried and tried and failed and failed and failed to loose weight with this methodology. The definition of insanity is “doing the same thing over and over and expecting a different result.”
Most of my patients are not insane, they recognize this and stop exercising and stop restricting calories . . . ’cause they realized, like I have, that it just doesn’t work! If you’re one that is still preaching caloric restriction and cutting out fat, I refer you to the figure above and the definition of insanity . . .
So, if reducing the calories in our diet and exercising more is not the mechanism for turning on and off the storage of fat, then what is?
Before I can explain this, it is very important that you appreciate the difference between triglycerides and free fatty acids. These are the two forms of fat found in the human body, but they have dramatically different functions. They are tied to how fat is oxidized and stored, and how carbohydrates are regulated.
Fat stored in the adipose cells (fat cells) as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
(“What! Fat comes from sugar?! How can this be?!!“)
We all know that glucose derived from sugar is taken up by the cells from the blood stream and used for fuel, however, when too much glucose is in the blood stream or the blood sugar increases above the body’s comfort zone (60-100 ng/dl), the body stores the excess. The process is called de novo lipogenesis, occurring in the liver and in the fat cells themselves, fancy Latin words for “new fat.” It occurs with up to 30% (possibly more if you just came from Krispy Kream) of the of the carbohydrates that we eat with each meal. De novo lipogenesis speeds up as we increased the carbohydrate in our meal and slows down as we decrease the carbohydrate in our meal. We’ve known this for over 50 years, since it was published by Dr. Werthemier in the 1965 edition of the Handbook of Physiology (2).
While we know that fat from our diet and fat from our food is stored as triglyceride, it has to enter and exit the fat cell in the form of fatty acids. They are called “free fatty acids” when they aren’t stuck together in a triglyceride. In their unbound state, they can be burned as fuel for the body within the cells. I like to think of the free fatty acids as the body’s “diesel fuel” and of glucose as the body’s version of “unleaded fuel.” The free fatty acids can easily slip in and out of the fat cell, but within the adipose cell, they are locked up as triglycerides and are too big to pass through the cell membranes. Lipolysis is essentially unlocking the glycerol from the free fatty acids and allowing the free fatty acids to pass out of the fat cell. Triglycerides in the blood stream must also be broken down into fatty acids before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).
So when carbohydrates increase in the diet, the flow of fat into the fat cell increases, and when carbohydrates are limited in the diet, the flow of fat out of the fat cells increases.
Summarizing the control mechanism for fat entering the fat cell:
- The Triglyceride/Fatty Acid cycle is controlled by the amount of glucose present in the fat cells (conversion to glycerol phosphate) and the amount of insulin in the blood stream regulating the flow of fatty acid into the fat cell
- Glucose/Fatty Acid cycle or “Randle Cycle” regulates the blood sugar at a healthy level. If the blood glucose goes down, free fatty acids increase in the blood stream, insulin decreases, and glycogen is converted to glucose in the muscle and liver.
These two mechanisms ensure that there is always unleaded (glucose) or diesel fuel (free fatty acids) available for every one of the cells in the body. This provides the flexibility to use glucose in times of plenty, like summer time, and free fatty acids in times of famine or winter when external sources of glucose are unavailable.
The regulation of fat storage, then, is hormonal, not thermodynamic. Unfortunately, we’ve know this for over 65 years and ignored it.
We’ve ignored it for political reasons, but that’s for another blog post . . .
References:
1. James, W. J Intern Med, 2008, 263(4): 336-352
2. Wertheimer, E. “Introduction: A Perspective.” Handbook of Physiology. Renold & Cahill. 1965.
3. Taubs, G. “The Carbohydrate Hypothesis, II” Good Calorie, Bad Calorie. Random House, Inc. 2007, p 376-403.
Insulin Resistance and The Horse

As a family practice physician and bariatrician, my job is to examine and treat the “Diseases of Civilization.” The Diseases of Civilization are those diseases arising out of the changes induced by industrializing and modernizing a society of people. These include diseases like diabetes, dyslipidemia (abnormal cholesterol), heart disease, hypertension, gout, vascular disease, & stroke. It is interesting that the so called Diseases of Civilization didn’t really appear on the scene until the early 1900’s. Yes, we have now identified some of these diseases in the early Egyptians, but to my point, as a society modernizes or industrializes, certain types of disease begin to arise. The Canadian cardiologist William Osler, one of the founding professors of John’s Hopkins Hospital, documented the first “syndrome” associated with narrowing of the arteries causing heart disease at the turn of the 19th century, and in 1912, the American Cardiologist James Herrick is credited with the discovery that narrowed arteries cause angina, a form of chest pain with exertion.
Today we know that underlying each of these diseases is the phenomenon of insulin over production, which seems to arise between five and twenty years prior to the onset of the Diseases of Civilization. Metabolic Syndrome, Dysmetabolic Syndrome or Syndrome X is the name we’ve given to the presentation of three or more of these diseases at once in one person. There is still argument as to whether insulin over production is the chicken or the egg, but what I see clinically has convinced me that insulin is culprit.
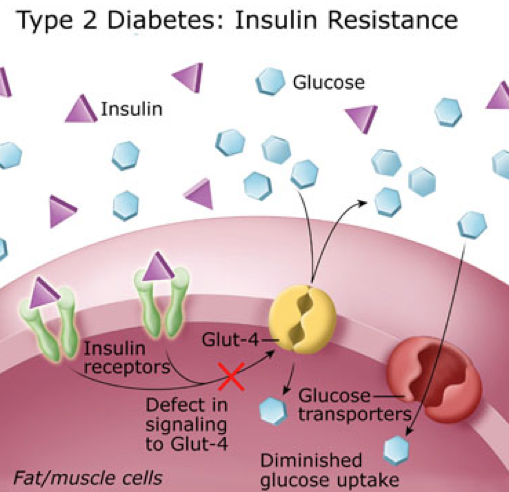
Insulin is a very powerful hormone that acts as a key, opening a door in just about every cell in the body, letting glucose (the primary form of fuel derived from carbohydrate) into the cell. For reasons that appear to be genetic, this key becomes “dull” in a portion of the population and does not unlock the door fast enough to lower the blood sugar. So, the body panics, and stimulates production of additional insulin, 2-10 times more in many people. However, the insulin that was produced initially, eventually kicks in. This extra insulin, acting at a slower rate, is the underlying culprit to the Diseases of Civilization.
How, you ask? Let me explain.
Insulin does more than just open the door for glucose.
1. Insulin causes weight gain. It turns on the storage of fat by activating an enzyme called lipoprotein lipase, pulling the triglycerides out of the cholesterol molecules and depositing them in the adipose tissue (fat cells).
2. Insulin raises cholesterol. It drives increased triglyceride production in the liver, especially in the presence of fructose.
3. Insulin triggers atherosclerosis. Triglycerides are essentially the passenger in the LDL (bad cholesterol) molecule. Higher triglycerides cause increased LDL production leading to increased atherosclerosis (narrowing of the arteries).
4. Insulin causes gout & kidney stones. Insulin increases uric acid production and in a round about way can increase calcium oxylate as well, increasing the risk of kidney stones and gout.
5. Insulin raises blood pressure. Insulin stimulates the retention of sodium, causing and increase in blood pressure.

6. Insulin makes inflammation worse. Insulin drives the inflammatory cascade and increases free radicals, and stimulates the inflammatory hormones causes arthritis, allergic rhinitis, psoriasis, dermatitis, and inflammatory bowel problems to be amplified.
My intent is not to demonize insulin. It is an essential hormone, however, when five to ten times the normal amount of insulin is being produced, you’re going to amplify the problems above by five to ten times normal. Type II Diabetes is really just a consequence of 15-20 years of over production of insulin.
This isn’t just something that affects humans. either. We have been seeing this in other species of the animal kingdom as well. Take for example my wife’s horse, Jazz. She’s a beautiful grey Arab/Saddle-Bred who kept having problems with laminitis, or more colloquially known as “founder.” Her diet consisted predominantly of alfalfa at the time, considered a moderate starch containing form of feed.
Laminitis is a progressively increasing tenderness to the hoof of horses or cattle that can be disabling and if not treated appropriately can cause permanent lameness in the animal. Recent literature in the veterinary world have identified that animal diets high in starch have a propensity to cause laminitis as well as colic. First identified in the equine community in the 1980’s with glucose tolerance tests, insulin resistance has been identified as a significant factor in hoof disease. The use of Corn, Oats, Barley or even Alfalfa as a primary form of feed for a horse with insulin resistance greatly increases the risk of laminitis.
Like Jazz, many horses in the arid Arizona climate are fed primarily with oats and alfalfa. Jazz was tested and found to have insulin resistance. Since Jazz has been placed on a much lower starch containing feed, she has had no further problems with laminitis. We converted all our horses to Bermuda grass.

Our family and our horses are all now on Low-Carb diets to some degree and have been for the last seven years. No further hoof problems with the horses, and 55 lbs of weight loss with normalization of cholesterol in their owner, me.

For those with interest, studies reveal feeds in order of the highest to lowest starch (carbohydrate) content to be: Sweet Feed, Corn, Oats, Barley, Wheat Bran, Beat Pulp, Alfalfa, Rice Bran, Soybean hulls, Bermuda Grass. Take a look the Low Carbohydrate help section in the menu above to see the carbohydrate content of many of the foods for human consumption.
It’s time we recognize that our diet and lifestyles have lead us to the Diseases of Civilization, and those diets and lifestyles have even effected our animals.
The Terminator is Obese?
 When you visit your doctor, he or she will probably measure your height and your weight. Then a Body Mass Index (BMI) will be calculated and placed on your chart. The BMI has actually become one of the standard “vital signs” required at a doctor visit over the last five years. This was not something that physicians started measuring on their own, it is a required measurement most health insurance plans insist upon before they will pay for the visit. BMI is an interesting and arguably worthless measurement. It was developed by a Belgian physicist by the name of Adolphe Quetelet some time between 1830-1850. Quetelet was a “Social Physicist,” trying to combine probability and statistics with the study of sociology (1). BMI was originally called the “Quetelet Index” and was designed specifically to measure averages among large populations in sociology or epidemiological studies (2).
When you visit your doctor, he or she will probably measure your height and your weight. Then a Body Mass Index (BMI) will be calculated and placed on your chart. The BMI has actually become one of the standard “vital signs” required at a doctor visit over the last five years. This was not something that physicians started measuring on their own, it is a required measurement most health insurance plans insist upon before they will pay for the visit. BMI is an interesting and arguably worthless measurement. It was developed by a Belgian physicist by the name of Adolphe Quetelet some time between 1830-1850. Quetelet was a “Social Physicist,” trying to combine probability and statistics with the study of sociology (1). BMI was originally called the “Quetelet Index” and was designed specifically to measure averages among large populations in sociology or epidemiological studies (2).
BMI = mass (kg) / [height (m)]²
However, it wasn’t Quetelet that got BMI placed on the medical chart. BMI was made popular by the infamous Ancel Keys (the same Ancel Keys responsible for the flawed Seven Countries Study) in his July 1972 article published in the Journal of Chronic Disease. Ancel Keys, himself, explicitly stated that BMI was designed specifically for population studies, and inappropriate for evaluation of individual health (2). But, because of the ease of measurement, and the fact that Life Insurance companies had been using BMI to set your insurance premiums since the 1970’s, Health Insurance companies adopted it as a measure of overall health. In 1985, because BMI found great favor in epidemiological research, the National Institutes of Health (NIH) adopted it as the method to identify and define obesity in patients. And, in 1998 the NIH identified the BMI cutoffs – 25 for overweight, 30 for obesity – as easy numbers that could be remembered and used to counsel patients on weight reduction and health.
 The problem with BMI is that it doesn’t actually identify a person with excessive fat accumulation. BMI is a height to weight ratio. It doesn’t account for fat at all. Using the NIH guidelines, the Terminator, with an estimated BMI of 31, would be considered obese. (You try telling the Terminator that he is obese, and see what happens.) Because, muscle weighs twice as much when compared to an identical volume of fat, Mr. Schwarzenegger (or anyone with increased muscle mass), will have a higher scale weight. This raises the BMI calculation, giving a false indication of increased health risk.
The problem with BMI is that it doesn’t actually identify a person with excessive fat accumulation. BMI is a height to weight ratio. It doesn’t account for fat at all. Using the NIH guidelines, the Terminator, with an estimated BMI of 31, would be considered obese. (You try telling the Terminator that he is obese, and see what happens.) Because, muscle weighs twice as much when compared to an identical volume of fat, Mr. Schwarzenegger (or anyone with increased muscle mass), will have a higher scale weight. This raises the BMI calculation, giving a false indication of increased health risk.
I was recently asked about a study published in The American Journal of Medicine that was recently commented on in Scientific American regarding BMI vs Muscle Mass as a predictor of longevity. The assumption is that just because your doctor measures BMI, it must be a great tool predicting health outcomes. The assumption is absolutely wrong. We know from multiple studies, including the article sited above, that increase muscle mass increases overall health, decreases the likelihood of insulin resistance and diabetes, reduces the risk of heart disease, and extends longevity. How can a measure of height to weight predict longevity? It can’t. The only reason BMI is on the medical chart, thanks to the NIH, is so that the physician gets paid.
In actuality, the most effective way of measuring a persons health is to simply measure body fat. This can easily be done by measuring waist circumference with an inexpensive tape measure. It can also be done with a simple bioelectrical impedance measurement. The gold standard for measuring body fat is to strip you down naked and dip you in a tub of water, measuring the water displacement. (I have very few patient’s that will return to my office after doing that, so we don’t use it very often, but it is effective).
The answer to the question is “NO,” the Terminator is NOT obese. And, if he shows up in my office, I’m not going to comment about his BMI.
1. Eknoyan, Garabed (2007). “Adolphe Quetelet (1796–1874)—the average man and indices of obesity”. Nephrology Dialysis Transplantation 23 (1): 47–51.
2. Keys, Ancel; Fidanza, Flaminio; Karvonen, Martti J.; Kimura, Noboru; Taylor, Henry L. (1972). “Indices of relative weight and obesity”. Journal of Chronic Diseases 25 (6–7): 329–43
The Self-Discipline Muscle
Many patients come to my office desiring to loose weight, but complain of no self-control. They feel they cannot loose weight because they don’t have the willpower. Willpower, or self-control, is an elusive and mysterious thing. “If only I had more self-control,” I hear people say, “I could . . . ” exercise regularly, eat right, avoid drugs and alcohol, save for retirement, stop procrastinating, achieve a noble goal, or loose weight. A 2011 American Psychological Association study reveals that almost 30% of those interviewed felt that lack of willpower was the greatest barrier to making a change in any of these areas.
So what is “willpower” or “self-control?” It is the ability to resist short-term temptations in order to fulfill a long-term goal. 
I meet and work with people every day who feel they have no willpower. In actuality, will power and self-control are learned behaviors that develop over time. Anyone can have willpower, you just have to understand how willpower in certain areas can be strengthened and what makes it weak. In fact, a 2005 study showed that self-discipline or willpower was more important than IQ in academic successes. This study also found that increased self-discipline lead to less binge eating, higher self-esteem, higher grade point averages, better relationship skills and less alcoholism. Fascinating isn’t it!?
The answer can be found in a quote from Henry P Liddon, “What we do upon some great occasion will probably depend on what we already are; and what we are will be the result of previous years of self-discipline.” This means that willpower or self-control can be learned or improved. How, you ask?
First, you must establish and write down a reason or motivation for change. In addition, that change must fulfill a clear goal. Just wanting to loose weight isn’t good enough. You have to be motivated because of a consequence that arises from the obesity or overweight. And, you “loosing weight” isn’t a clear goal. You must set a weight reduction goal. It has to be clearly written down with your motivational reason. Willpower or self-control cannot begin to form until these two steps occur.
Second, you must begin to monitor your behavior toward that goal. When it comes to weight loss, I ask every one of my patient’s to keep a diet journal. In this journal they are asked to write down every thing they eat and drink. The night before, they are to write down their plan for tomorrow’s meals, then the next evening, they account for their success or failure by journaling on that same page what they actually ate and drank, then after comparing what they did, they plan for tomorrow and journal why they were successful or why they weren’t. It’s the last part that is so powerful, a short 3-5 minutes of self-introspection. Self-introspection is the key to behavioral change. It is the key that allows a person to see their habits and then make very small changes that break bad habits, solidify good habits and strengthens willpower.
Third, willpower is developed over time. It is developed by being accountable to ones-self on very little things every single day. But it MUST be written down. If I planned to eat bacon and eggs for breakfast and I didn’t, why? When I look at my day, I may realize that I went to bed too late to get up early and cook bacon and eggs. So, instead, I ate a yogurt that was in the fridge. I am accountable to myself. If I plan to eat bacon and eggs tomorrow, I must either go to bed earlier, prepare them the night before, or throw out the yogurt . . . so not to be a temptation again. This is written down and I make a very small change tomorrow.
 Over time, this self-introspection becomes easier and easier, to the point that you do it sub-consciously. It is this sub-conscious self-introspection and change will be seen by others as self-control or willpower. Just like a working or strengthening a muscle, recording short goals and and accounting for them makes your self-discipline stronger. The self-discipline muscle becomes more powerful. In time, a split second decision not to binge on that piece of cake will be seen as strong willpower by those around you. You’ll recognize that it’s just flexing your self-discipline muscle.
Over time, this self-introspection becomes easier and easier, to the point that you do it sub-consciously. It is this sub-conscious self-introspection and change will be seen by others as self-control or willpower. Just like a working or strengthening a muscle, recording short goals and and accounting for them makes your self-discipline stronger. The self-discipline muscle becomes more powerful. In time, a split second decision not to binge on that piece of cake will be seen as strong willpower by those around you. You’ll recognize that it’s just flexing your self-discipline muscle.
So, my next question to you is . . . where’s your diet journal?
Low-Carb Diets . . . Bad For Health?
