

A few years ago, my family and I set out to build a pond.
I have always loved Koi and the serenity of a Koi pond in my own back yard was very enticing. I spent about a year planning my design and the location. I dreamed of a serene evening after a very long, hectic day seeing patients relaxing beside the pond. The sound of trickling water, the occasional splash from fish, the cool breeze passing over the mist from a water-fall would sooth my soul after a busy day in the office.
I envisioned the perfect area. An unused access path, previously worn by the previous owner with truck and trailer traffic, beside my now expanded patio. Twenty feet wide, thirty feet long and four feet deep. . . that seems just perfect.
I pulled out my shovel and set about digging. Eager to begin and filled with the energy of the final product, I set to digging. What could be so hard about digging my own pond? Think of the exercise I will be getting. Thoughts spurred me on.
Minutes later, chest heaving, face glistening with sweat, I stared in dismay at the ground. All I had to show for my wild digging was a small 1/2 inch dent in the dusty Arizona top soil.
Sonoran Clay
Over time, calcium-carbonate, along with other minerals, accumulates and dissolves into the topsoil of the very arid regions of Arizona Sonoran Desert. It forms a two to three-foot layer of soil called “caliche.” Periodic rains carry the calcium as far as three feet down into the soil, then the water rapidly evaporates in the blistering Arizona heat. This often forms two to three feet of soil that is “literally” harder than concrete.

With tremendous zeal, a great deal of sweat and a round of painful blisters, I broke my third shovel on this impenetrable ground. I realized this was much more difficult than I thought. I pulled out the back-hoe attachment for my small farm tractor. After a few hours and few gallons of diesel fuel later, still very little progress occurred.
Multiple weekends and evenings of digging in the Arizona caliche left me with three broken shovels, a ruptured hydrolic line in my tractor, anger that my expensive back-hoe attachment didn’t work, and only a small dent in the ground near my patio. Even the brute force from the tractor would not budge the clay. I wondered if dynamite would be effective? (My wife would have none of this idea).
With my exuberance quashed, I concluded that this would require much more measured exhuming.
Escape From the Prison
We often imagine, with great delight, the removal or destruction of that which enslaves or imprisons us. We dream that just a little sweat, exertion of a few shovel scoops of dirt and the foundation to our prison of obesity, addiction, debt, and depression are exposed. A few extra scoops and we imagine freedom from that prison cell.
If only I had a jack hammer and a bigger, more powerful scoop, I imagine . . . I could make short work of these manacles that bind me.
But, our manacles and prison cells do not so easily give way.
The failings of our sharpened spades and powerful back-hoes form a new, even stronger fetter – the belief that our prison cell is unbreakable, that our challenge is just too great. These failings usually leave a person cured of any further desire to break free. It quashs the dream and solidifying the depression of stagnation.
The in-fecundity of my shovel, no matter the strength and effort put behind it, was not cause to quit. It was life’s lesson that prisons and shackles often only need a simple tool.
Enter the pick-axe. During this process my wife said, “Honey, why don’t you use the pick in the garage?”
“If my shovel and the back-hoe didn’t work, there was no way I was going to break through this clay with a pick axe.” That was absurd, I thought.
Yet when I humbled myself to try, it was simple. The pick-axe was unpretentious. This simple tool allowed for an almost effortless stroke to a small area of weakness in the caliche. A large flake of soil would pop free with each stroke. The process was repeated.

Scale by scale, the dragon’s flank was exposed. Careful work of the pick-axe began to loosen layer after layer, section after section, pellicle after pellicle. Yes, it was slow work. But, each swing was a small victory.
At each little victory, my heart would leap, the dream would become ever clearer.
Working this magic again and again until finally the specter was weakened enough to pull out the shovel. And, further work, allowed for bringing back the powerful back-hoe, in gratifying scoops.
The excavation that I thought would take two months took me fourteen. But, it was gratifying.

I learned a powerful lesson. Wherever life has pinned you, fettered you or barred you in, put down the shovel, and pick up the pick-axe. Second, if you really listen, your spouse may point out the tool you really need. Don’t be afraid to chip away at it a piece at a time.

Finances
Stop waiting for the sharper shovel or the bigger back-hoe to dig yourself out of your harrowing debt, mega mortgage, or your income dwarfing spending. The jackpot or financial windfall won’t come. While others await the jackpot, put down your shovel and shoulder your pick-axe.
- Pick one small debt and begin to pick at it by applying just a little extra each month until it is gone.
- Cancel your extra cable, sell the motorcycle and payoff the 21% interest credit card.
- If you must, pick up a side-hustle for extra to sharpen the pick.
Once you’ve lifted one flake, chip away at the next. Making progress will make it easier to continue. It doesn’t matter how long it takes, just keep at it.
Marriage
You long for resolution of the apathy, progressive resentment and mutual stalemate that permeates your relationship. You look in vain for the bigger shovel that will uncover the treasure that years of apathy have buried. You long to uncover your dreams and needs that have been covered and hardened under the clay of resentment. The shovel and the back-hoe won’t help you here.
Drop the shovel. Shoulder your pick-axe.
- Kiss your wife every time you leave, even if it’s just for a ten minutes to run to the convenience store.
- Hold her for five seconds longer every time you hug.
- Find a gift you can give her once a week, just because.
- Put down your phone and look her in the eyes when she talks to you and listen. Really listen and the flakes of hard clay will unveil the beauty of her soul.
- Find a way to praise her every day, even if it is through a simple text.
Health
You long to rid yourself of your addiction to sugar, bread, stress, and sleep deprivation. You’ve tried to scoop them out of your life. You even hired a trainer with some muscle to force you to change. You’ve tried in vain to save yourself from yourself.
Trying to use the shovel here is like trying to use the shovel on steel forged walls of your life’s prison fortress. Forget the shovel. Shoulder your pick-axe.
- Start with one meal and make some substitutions. My dietary plan can help you with this.
- Go to bed an hour earlier. Really, you’ll be surprised that the focus you have will more than compensate for the hour of lost time in the evening.
- Add a quality vitamin to your morning routine.
- Take ten minutes and do 20 push-ups and 20 sit-ups, then take a 10-minute walk.
- Simply remove the “white stuff” from your meals. You will be amazed at the results.
- Put down your phone for 30 minutes and read that book you’ve been meaning to read, instead of surfing Facebook.
Grand-standing with your back-hoe doesn’t help you. Just swing the pick-axe once or twice. Simple daily picking with the sharp point weakens the hardest of ground and the prison walls in our lives. It takes time, so be patient.
Find the weak point, apply the pick. Day by day, little by little you will be free.

I’ve been there. I’m with you. Keep me posted on your journey.
If you’re looking for a program that teaches you how to do this, check out my membership site.



 So, how do you manipulate the hormones in a way to control the rebounding hunger and suppression of metabolism? This is where we put a bit of twist on the knowledge we’ve gained from alternate day fasting. Recent research shows that “mild” energy deficit in a pulsatile manner, that has the ability to mimicking the body’s normal bio-rhythm’s is dramatically effective in reducing weight and maintaining normal hormonal function without cause of rebound metabolic slowing (4).
So, how do you manipulate the hormones in a way to control the rebounding hunger and suppression of metabolism? This is where we put a bit of twist on the knowledge we’ve gained from alternate day fasting. Recent research shows that “mild” energy deficit in a pulsatile manner, that has the ability to mimicking the body’s normal bio-rhythm’s is dramatically effective in reducing weight and maintaining normal hormonal function without cause of rebound metabolic slowing (4).




























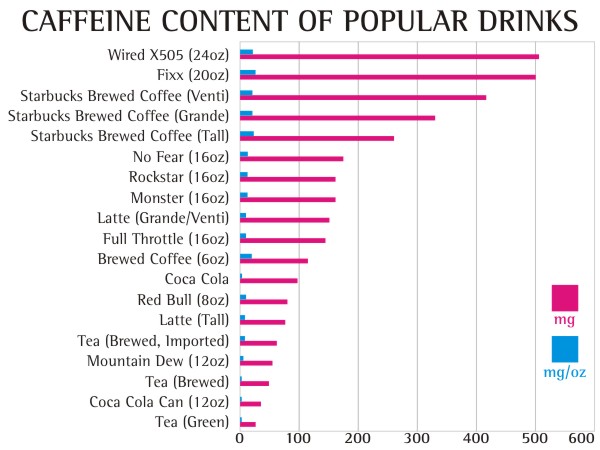
 After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the
After mulling through the last 10 years of caffeine research, most of which were small studies, had mixed results, used coffee as the caffeine delivery system (coffee has over 50 trace minerals that has the potential to skew the results based on the brand) and never seemed to ask the right questions, the ink from a study in the 





 That something else should be fat. Protein must be moderated, as it will also be stored as fat if you eat too much. So, if the carbohydrates are kept low, fat intake can be increased and the body will pick the fat it wants and essentially throw the rest out without raising cholesterol, causing weight gain or causing heart disease. This is why we want you to use good natural animal fats like butter, hard cheese, olive oil, coconut oil, avocado, etc. Look for fats highest in omega-3 fatty acids as these decrease inflammation and improved weight loss. Look for meats highest in fat like red meat (55% fat) and pork (45% fat). Take the food pyramid and flip it over.
That something else should be fat. Protein must be moderated, as it will also be stored as fat if you eat too much. So, if the carbohydrates are kept low, fat intake can be increased and the body will pick the fat it wants and essentially throw the rest out without raising cholesterol, causing weight gain or causing heart disease. This is why we want you to use good natural animal fats like butter, hard cheese, olive oil, coconut oil, avocado, etc. Look for fats highest in omega-3 fatty acids as these decrease inflammation and improved weight loss. Look for meats highest in fat like red meat (55% fat) and pork (45% fat). Take the food pyramid and flip it over.
 20% of women that I see in my practice who are over 55 years old, need some degree of estrogen replacement before they are able to lose weight. Estrogen plays a very large role in regulation of the metabolism and when deficient, causes weight retention or weight gain. Talk to your doctor about the risks and benefits of estrogen for you individually in this situation.
20% of women that I see in my practice who are over 55 years old, need some degree of estrogen replacement before they are able to lose weight. Estrogen plays a very large role in regulation of the metabolism and when deficient, causes weight retention or weight gain. Talk to your doctor about the risks and benefits of estrogen for you individually in this situation.











{kind=link}