
“It’s a snake.”
“It’s a wall.”
“It’s a rope.”
“It’s a fan.”
“It’s a tree.”
“It’s insulin resistance.”
I’ve always been fascinated by those describing a “new finding” in medicine. I am reminded of the story of 5 men who, never having seen an elephant before, were blindfolded and asked to describe what he discovered. However, each man was introduced to a different part of the elephant. Each of them had a dramatically different description of the elephant and each made a conclusion that was very different from the others.
What is fascinating, is that we usually make our “blindfolded comparisons” to those things we have seen or about which we have some descriptive understanding. Observing and describing human physiology is much like examining an elephant while blindfolded for the first time.
This week’s “blind-folded finding” is what has been interpreted by some as “insulin resistance” made worse by a ketogenic diet. Really? This perked my curiosity, because I’ve personally been following a low-carbohydrate/ketogenic diet for years and have thousands of patients doing the same. To this day, I’ve never seen insulin resistance “get worse.” In fact, it gets better. Clinically, it seems to take about 18-24 months to improve, but, it usually gets better.
THE QUESTION –
I’ve had three people from around the world contact me this week and ask why, after being on a ketogenic diet and “in ketosis,” they suddenly get a notably large blood glucose spike when they cheat. By notably large, I mean that their blood sugars rise to over 200 mg/dl within 2 hours of a carbohydrate containing meal. Now, they admit to rapid glucose recovery within an hour or two, and their hemoglobin A1c levels are subjectively normal (less than 5.6%). The worry is “am I becoming diabetic?” They also complain that after having been in ketosis for longer than 3-4 months, they cannot get their fasting blood sugars below 100 mg/dl.
Those asking me the question about this anomalous “physiological insulin resistance” referred to a couple of off-the-cuff blogger’s posts from 2-3 years ago referencing a few small studies (some of which were very poorly designed) [here, here, here & here] in the journals from 10-20 years ago. These articles describe a physiologic response interpreted as worsening “insulin resistance.” However, if you understand what is actually occurring in the Ketonian (yes, I made that term up – there will soon be a whole village of us), I see it as a normal physiologic response. It is misinterpreted by those who’ve never actually seen long term ketogenic physiology, as anomalous, in the average human.

THE ANSWER –
I’ve been seeing this slight elevation in fasting blood sugar with normal or low normal HbA1c in myself and many of my patients for quite some time. However, I never saw it as “insulin resistance” worsening. Clinically, when I tease out the food logs, it usually ends up being protein intake is too high, the person is using a sweetener or creamer causing rebound morning glucose elevation or, in those with low normal HbA1c’s (4.3-5.6%), it is in actuality a protective mechanism of “physiologic glucose sparing” in the keto-adapted individual (1, 2).
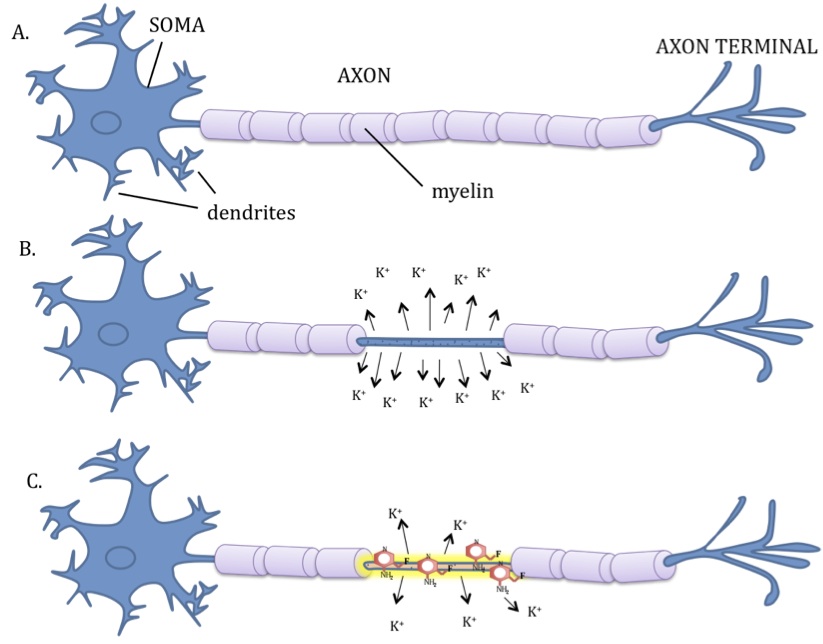
It can very easily be explained when one understands how ketones are actually used in the keto-adapted individual. First, a wonderful figure below (Thank you for pointing me to this one, Dr. Peter Attia) found in Dr. Veech et. al.’s paper (3) gives us an overview of how ketones skirt the TCA cycle within the mitochondria of the cell, causing inhibition of pyruvate dehydrogenase leading to glucose sparing by the cells of the brain that still require it’s availability (Oh, by the way, this is how we survived harsh winters and famines).
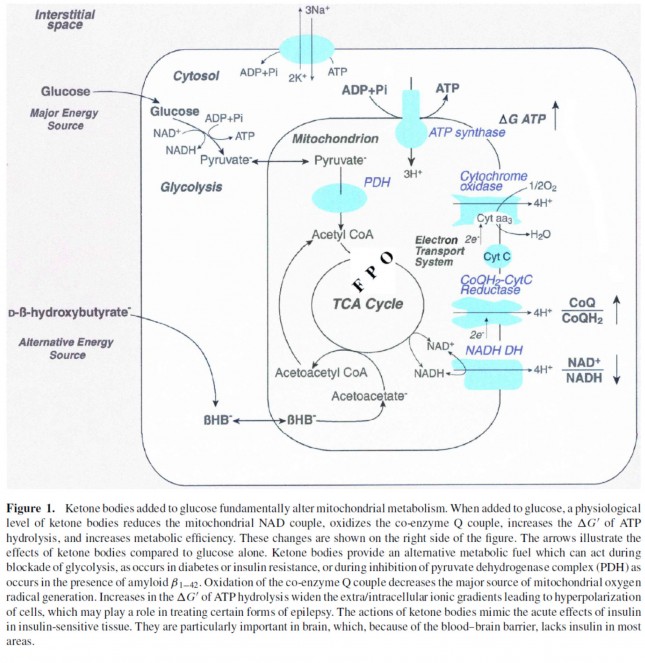
From the Figure 1 above, you can see that beta-hydroxybuterate [BHB (a ketone)] is converted to acetoacetyl CoA leading to the production of pyruvate, block-aiding additional glycolysis or inhibiting further glucose production at the liver level. Because the muscle tissues become more adept at using BHB, GLUT receptors are down-regulated at the muscle level as a person becomes more keto-adapted. Although we still have much to learn about the keto-adapted state, we know that this occurs more prominently in the muscle tissues than in the gut and brain. This fascinating glucose sparing phenomenon, has been interpreted by some as “worsening insulin resistance.”
Not to worry, glucose sparing is rapidly reversible and transitory within 1-3 days of increasing carbohydrate intake above 100-150 grams per day (1). It is also why those who become keto-adapted get a carbohydrate hangover including headache, stomach cramps, diarrhea, and malaise lasting 8-24 hours after cheating.
Is this bad? Absolutely not! It is NORMAL! (It’s just that most people, physicians included don’t know what the normal physiology of the Ketonian should look like.) Is it going to kill you, cause a stroke or give you a heart attack? Absolutely not. The elevated BHB actually increases production of adiponectin, leucine & glutathione that have antioxidant properties protecting one from transient inflammatory rises in blood sugar, enhancing insulin’s effect on the muscle, and preserving muscle mass while allowing for fat metabolism (4, 5, 6).
THE TAKE-HOME MESSAGE –
First, don’t cheat if you don’t want to see transient rises in blood sugar and experience the wonders of a carbohydrate hangover and some mild reactive hypoglycemia (low blood sugar) after the fact.
Second, if you’ve been in ketosis for longer than 3-4 months, and you absolutely must get another two or three hour oral glucose tolerance test (OGTT), you might want to increase your carbohydrate intake to 50-100 grams per day 1-3 days before the test to avoid an anomalous spike in blood glucose. (One OGTT was enough for me . . . but hey, some of us are gluttons for punishment.)
Third, enjoy your eggs, pass the bacon and stir me up some Keto//OS.

References:
- Kinzig KP, Honors MA, Hargrave SL. Insulin sensitivity and glucose tolerance are altered by maintenance on a ketogenic diet. Endocrinology 151: 3105–3114, 2010.
-
Veech RL, Chance B, Kashiwaya Y, Lardy HA, Cahill GF Jr. Ketone bodies, potential therapeutic uses. IUBMB Life. 2001 Apr;51(4):241-7.
- Jarrett SG, Millder JB, Liang LP, Patel M. The ketogenic diet increases mitochondiral glutathione levels. J Neurochem. 2008 Aug; 106(3): 1044-51.
- Rauch JT et al. The effects of ketogenic dieting on skeletal muscles and fat mass. J Int Soc Sports Nutr. 2014; 11(Suppl 1): P40
- Manninen AH. Very low carbohydrate diets and preservation of muscle mass. Neut Metab (London). 2006; 3:9


















































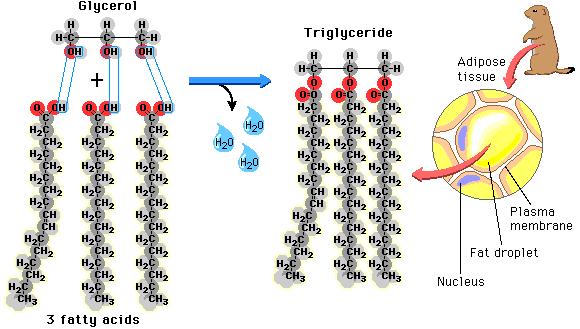 as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
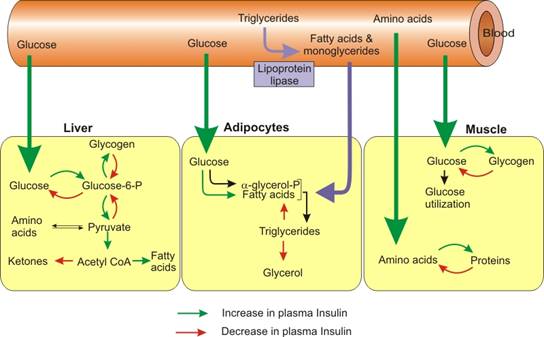 before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).
before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).

{kind=link}