A number of patients come in to the office struggling with loosing weight. When I review their dietary journals with them, I notice that many of them never stop eating fruit (because, fruit is good for you, right?!). Well, lets put it this way:
One banana for breakfast is equal to . . .
. . . just over seven (7) teaspoons of sugar.
Count them . . . seven (7) teaspoons.
If your eating a banana for breakfast, it is halting your weight loss for up to 12 hours. Give the banana’s to the monkeys and cook up some sausage and eggs for breakfast tomorrow.
Now you have to watch your salt ingredients too. Store bought salts are starting to add dextrose for flavor. Dextrose is just another word for SUGAR!! Aaarrrrhhhhh!! Why do you need to add sugar to your salt? You don’t. Throw out any salt that contains dextrose. It will raise your cholesterol and cause weight gain.
Never noticed this until it was pointed out by Maria Emmerich. Thanks, Maria.
A few of my patients have come in struggling with their weight this week, following what they assumed to be a low carbohydrate diet. They were eating yogurt for breakfast, a chicken salad for lunch, and chicken and vegetables for dinner. A true low carbohydrate diet is ketogenic (it derives fuel from ketones) and is the byproduct of fatty acid metabolism. That means your fuel is coming from fat, not protein or carbohydrate. The presence of glucose, fructose, lactose or other sugars (or many sugar alcohols) shut fatty acid metabolism down and halt the process of weight loss and frequently increase weight gain. Too much protein does the same thing. A chicken salad is not ketogenic. It may be low carb, but without adequate fat, the absence of glucose drives the body to use protein as it’s primary fuel source. It is essential to maintain ketosis that a low carbohydrate diet moderate the protein and increase the fats to upwards of 60-70% of the total caloric intake.
Bacon is a 50/50 food. (I’m not talking about turkey bacon . . . that’s not real bacon). Each slice of real bacon is at a minimum 3 grams (50%) fat, and 3 grams (50%) protein. No carbs there, either.
So, if you’re struggling with your weight loss on a low carb diet . . . your first step should be “BLT” it!
Did you fall off the low-carbohydrate wagon this week? Did those donuts just call out your name as you walked by the bakery in the grocery store? Maybe you feel like you were shot out of the carbohydrate cannon, landing in the nearby Potato County? If so, you probably had a relapse. You were doing so well, then all the sudden, your will-power caved.
Relapse is not uncommon when making a dietary lifestyle change. What causes relapse? I often see people relapse back to the Standard American Diet, the SAD diet, because of a number of reasons.
Neuro-hormones of Hunger
First, it is important to recognize that there are a milieu of neuro-hormones that drive hunger cravings or suppression. Anything that triggers a change in these hormone levels can cause the carbohydrate cravings to kick in . . . and you find yourself stuffing yourself with “carbage.”
Second, is boredom. Many people find an increased nervousness when they get bored. They find that eating, with it’s calming parasympathetic nervous system effect, diminish the nervousness that arises out of boredom. They often create a near Pavlov’s type trigger to eat when they experience boredom and it is quickly interpreted as hunger. There is actually a release of endorphin associated with eating and chewing that suppresses stress and or anxiety. Reduction of stress, exercise, and journal writing have been found to help patient’s reduce the food cravings associated with boredom. It is important to have “rescue foods” like string cheese, a handful of almonds, beef jerky, or “fat bombs” available that can be used when you experience these symptoms.
Following the line of triggers, Pavlov demonstrated that repeated actions associated with rewarding consequences will form a physiologic trigger. Frequently. our desire to eat carbohydrates (“carb cravings”) are often tied to triggers. For example, growing up in my home as a child, our family frequently would relax by watching prime-time television while eating a large bowl of popcorn and a Pepsi. To this day, whenever I turn on the television in the evening, I get cravings for carbohydrates. It is important to look at what you were doing or what was going on around you at the time the craving occurred. Substitution of foods has helped to solve these cravings by replacing the popcorn and Pepsi with pork rinds and Diet Dr. Pepper. (Don’t cringe, pork rinds and guacamole tastes fantastic and is a very low carbohydrate substitute that works for me.)
Lastly, many patients fall off the wagon when they visit or have a meal with family. They are often made to feel guilty if they don’t eat Aunt Velda’s homemade chocolate chip cookies. They are afraid of offending their relatives if they don’t partake of those tasty cookies. The challenge is that cheating by eating the cookies causes an insulin spike and leads to 24-72 hours of carbohydrate cravings thereafter. Are those cookies worth 72 hours of carbohydrate cravings? Maybe. But it is important to consider helping Aunt Velda to understand what those cookies will do to you, and that you still care for Aunt Velda even if you don’t eat her chocolate chip cookies.
In many families, food is often associated with love. “If you don’t eat the food I made for you, you don’t really love me” is an underlying tone that can be found in many family dynamics that I see in my office. Some times bringing your own low-carb chocolate chip cookies, and offering one to Aunt Velda, will stimulate a conversation about your dietary changes and diffuse the guilt and offence that might arise.
Often, knowing what will cause you to fall off the wagon, helps to keep you on the wagon. What challenges have you had staying on the wagon?
Has your weight loss plateaued? Are you struggling to meet your weight loss goals? Have you struggled to lose weight in spite of doing everything “correctly?” Are you still struggling with those last few pounds?
You’re not alone. Many of my patients, myself included, have found themselves “stuck” in their weight loss progression. There are a number of reasons you may not be loosing weight, but one that I am seeing more and more frequently is “Pseudo-Cushings’s Syndrome.” Pseudo-Cushing’s Syndrome is a physiologic
hypercortisolism (high level of cortisol) that can be caused by a number of problems:
Physical stress
Severe bacterial or fungal infection
Malnutrition or Intense chronic exercise
Psychological stress – including untreated or under-treated depression, anxiety, post-traumatic stress, or dysthymia (chronic melancholy)
Alcoholism
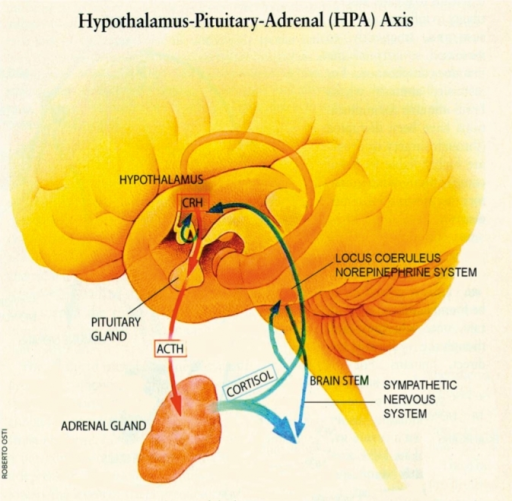
The psychiatric literature suggest that up to 80% of people with depressive disorders have increased cortisol secretion (1,2,3). People with significant stressors in their life have been show to have a raised cortisol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing an over production of cortisol and normalization of their cortisol levels occurs after resolution of the stressor. This cortisol response is not high enough to lead to a true Cushing’s Syndrome, but effects ones ability to loose weight.
I suspect this is becoming more prevalent due to the high paced, high-stress, always on, plugged in, 24 hour information overload lives we live.
What is cortisol? It is a steroid hormone made naturally in the body by the adrenal cortex (outer portion of the adrenal gland). Cortisol is normally stimulated by a number of daily activities including fasting, awakening from sleep, exercise, and normal stresses upon the body. Cortisol release is highest in the morning, helping to wake us up, and tapers into the afternoon. Cortisol plays a very important role in helping our bodies to regulate the correct type (carbohydrate, fat, or protein) and amount of fuel to meet the bodies physiologic demands that are placed upon it at a given time (4,5,6).
Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues and turns on the maturation process of adipocytes (fat cells). In the process, it suppresses the immune system to decrease inflammation during times of stress (7,8,9). In the short run, this is an important process, however, when cortisol production is chronically turned up, it leads to abnormal deposition of fat, increased risk of infection, impotence, abnormal blood sugars, head
aches, hypertension and ankle edema, to name a few.
The chronic elevation in cortisol directly stimulates an increase in insulin by increasing the production of glucose in the body, and cortisol blockaids the thyroid axis. Both of these actions halt the ability to loose weight, and drive weight gain.
Cortisol also increases appetite (10). That’s why many people get significant food cravings when they are under stress (“stress eaters”). Cortisol also indirectly affects the other neuro-hormones of the brain including CRH (corticotrophin releasing hormone), leptin, and neuropeptide Y (NPY). High levels of NPY and CRH and reduced levels of leptin have also been shown to stimulate appetite (10-11).
How do you test for Pseudo-Cushing’s Disease?
Testing can be done by your doctor with a simple morning blood test for cortisol. If your cortisol is found to be elevated, it needs to be repeated with an additional 24 hour urine cortisol measurement to confirm the diagnosis. If Cushing’s Syndrome is suspected, some additional blood testing and diagnostic imaging will be necessary.
How do you treat it?
First, the stressor must be identified and removed. Are you getting enough sleep? Is there an underlying infection? Is there untreated anxiety or depression present? Are you over-exercising? These things must be addressed.
Second, underlying depression or anxiety can be treated with counseling, a variety of weight neutral anti-depressant medications or a combination of both. Many of my patients find that meditation, prayer, and journaling are tremendous helps to overcoming much of the anxiety and depression they experience.
Third, adequate sleep is essential. Remove the television, computer, cell phone, iPad or other electronic distraction from the bedroom. Go to bed at the same time and get up at the same time each day. Give yourself time each day away from being plugged in, logged in or on-line.
Fourth, mild intensity (40% of your maximal exertion level) exercise 2-3 days a week was found to lower cortisol; however, moderate intensity (60% of your maximal exertion level) to high intensity (80% of your maximal exertion level) exercise was found to raise it (12). A simple 20 minute walk, 2-3 times per week is very effective.
So, the take home message . . . It’s not the stress that’s killing us, it’s our reaction to it.
References:
Pfohl B, Sherman B, Schlechte J, Winokur G. Differences in plasma ACTH and cortisol between depressed patients and normal controls. Biol Psychiatry 1985; 20:1055.
Pfohl B, Sherman B, Schlechte J, Stone R. Pituitary-adrenal axis rhythm disturbances in psychiatric depression. Arch Gen Psychiatry 1985; 42:897.
Gold PW, Loriaux DL, Roy A, et al. Responses to corticotropin-releasing hormone in the hypercortisolism of depression and Cushing’s disease. Pathophysiologic and diagnostic implications. N Engl J Med 1986; 314:1329.
Ely, D.L. Organization of cardiovascular and neurohumoral responses to stress: implications for health and disease. Annals of the New York Academy of Sciences (Reprinted from Stress) 771:594-608, 1995.
McEwen, B.S. The brain as a target of endocrine hormones. In Neuroendocrinology. Krieger and Hughs, Eds.: 33-42. Sinauer Association, Inc., Massachusetts, 1980.
Vicennati, V., L. Ceroni, L. Gagliardi, et al. Response of the hypothalamic- pituitary-adrenocortical axis to high-protein/fat and high carbohydrate meals in women with different obesity phenotypes. The Journal of Clinical Endocrinology and Metabolism 87(8) 3984-3988, 2002.
Wallerius, S., R. Rosmond, T. Ljung, et al. Rise in morning saliva cortisol is associated with abdominal obesity in men: a preliminary report. Journal of Endocrinology Investigation 26: 616-619, 2003.
Epel, E.S., B. McEwen, T. Seeman, et al. Stress and body shape: stress-induced cortisol secretion is consistently greater among women with central fat.
Psychosomatic Medicine 62:623-632, 2000.
Tomlinson, J.W. & P.M. Stewart. The functional consequences of 11_- hydroxysteroid dehydrogenase expression in adipose tissue. Hormone and Metabolism Research 34: 746-751, 2002.
Epel, E., R. Lapidus, B. McEwen, et al. Stress may add bite to appetite in women: a laboratory study of stress-induced cortisol and eating behavior.Psychoneuroendocrinology 26: 37-49, 2001.
Cavagnini, F., M. Croci, P. Putignano, et al. Glucocorticoids and neuroendocrine function. International Journal of Obesity 24: S77-S79, 2000.
Hill EE, Zack E, Battaglini C, Viru M, Vuru A, Hackney AC. Exercise and circulating cortisol levels: the intensity threshold effect. J Endocrinol Invest. 2008. Jul;31(7):587-91.
The only way to successfully loose weight is to modify or turn off the mechanisms that stimulate fat storage. For years we have been told that this was just a problem of thermodynamics, meaning the more calories you eat, the more calories you store. The solution was, thereby, eat less calories or exercise more, or both. We are taught in school that a 1 gram of carbohydrate contains 4 kcal, 1 gram of protein contains 4 kcal, and 1 gram of fat contains 9 kcal.
It’s easy to see that if I’m going to limit my calories, cutting out fat is the first step. For the last 65 years, we as a society have been doing just that, cutting out fat, exercising more and eating fewer calories. What has it done for us? It’s made us fatter! (1)
Obesity Rates Around the World
Some may argue that we really aren’t eating fewer calories and exercising more. But most people I have seen in my office have tried and tried and tried and failed and failed and failed to loose weight with this methodology. The definition of insanity is “doing the same thing over and over and expecting a different result.”
Most of my patients are not insane, they recognize this and stop exercising and stop restricting calories . . . ’cause they realized, like I have, that it just doesn’t work! If you’re one that is still preaching caloric restriction and cutting out fat, I refer you to the figure above and the definition of insanity . . .
So, if reducing the calories in our diet and exercising more is not the mechanism for turning on and off the storage of fat, then what is?
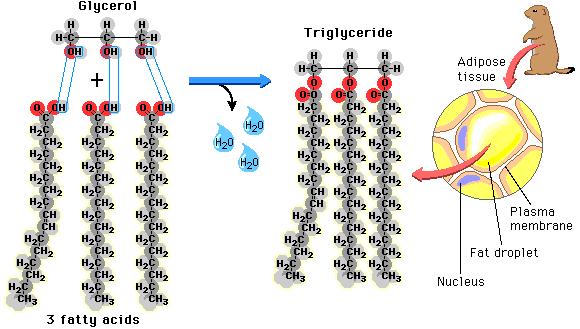
Before I can explain this, it is very important that you appreciate the difference between triglycerides and free fatty acids. These are the two forms of fat found in the human body, but they have dramatically different functions. They are tied to how fat is oxidized and stored, and how carbohydrates are regulated.
Fat stored in the adipose cells (fat cells) as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
(“What! Fat comes from sugar?! How can this be?!!“)
De Novo Lipogenesis
We all know that glucose derived from sugar is taken up by the cells from the blood stream and used for fuel, however, when too much glucose is in the blood stream or the blood sugar increases above the body’s comfort zone (60-100 ng/dl), the body stores the excess. The process is called de novo lipogenesis, occurring in the liver and in the fat cells themselves, fancy Latin words for “new fat.” It occurs with up to 30% (possibly more if you just came from Krispy Kream) of the of the carbohydrates that we eat with each meal. De novo lipogenesis speeds up as we increased the carbohydrate in our meal and slows down as we decrease the carbohydrate in our meal. We’ve known this for over 50 years, since it was published by Dr. Werthemier in the 1965 edition of the Handbook of Physiology (2).
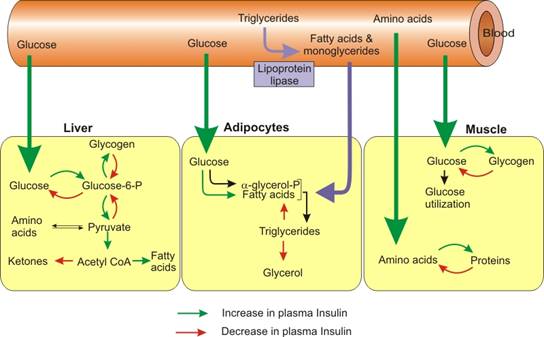
While we know that fat from our diet and fat from our food is stored as triglyceride, it has to enter and exit the fat cell in the form of fatty acids. They are called “free fatty acids” when they aren’t stuck together in a triglyceride. In their unbound state, they can be burned as fuel for the body within the cells. I like to think of the free fatty acids as the body’s “diesel fuel” and of glucose as the body’s version of “unleaded fuel.” The free fatty acids can easily slip in and out of the fat cell, but within the adipose cell, they are locked up as triglycerides and are too big to pass through the cell membranes. Lipolysis is essentially unlocking the glycerol from the free fatty acids and allowing the free fatty acids to pass out of the fat cell. Triglycerides in the blood stream must also be broken down into fatty acids before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).
So when carbohydrates increase in the diet, the flow of fat into the fat cell increases, and when carbohydrates are limited in the diet, the flow of fat out of the fat cells increases.
Summarizing the control mechanism for fat entering the fat cell:
The Triglyceride/Fatty Acid cycle is controlled by the amount of glucose present in the fat cells (conversion to glycerol phosphate) and the amount of insulin in the blood stream regulating the flow of fatty acid into the fat cell
Glucose/Fatty Acid cycle or “Randle Cycle” regulates the blood sugar at a healthy level. If the blood glucose goes down, free fatty acids increase in the blood stream, insulin decreases, and glycogen is converted to glucose in the muscle and liver.
These two mechanisms ensure that there is always unleaded (glucose) or diesel fuel (free fatty acids) available for every one of the cells in the body. This provides the flexibility to use glucose in times of plenty, like summer time, and free fatty acids in times of famine or winter when external sources of glucose are unavailable.
The regulation of fat storage, then, is hormonal, not thermodynamic. Unfortunately, we’ve know this for over 65 years and ignored it.
We’ve ignored it for political reasons, but that’s for another blog post . . .
References:
1. James, W. J Intern Med, 2008, 263(4): 336-352
2. Wertheimer, E. “Introduction: A Perspective.” Handbook of Physiology. Renold & Cahill. 1965.
3. Taubs, G. “The Carbohydrate Hypothesis, II” Good Calorie, Bad Calorie. Random House, Inc. 2007, p 376-403.
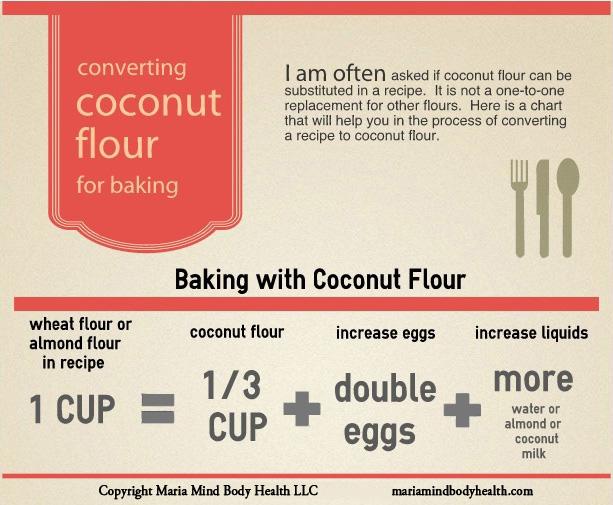
For those on a ketogenic or low-carbohydrate diet, whole wheat flour or almond flour is often substituted for with coconut flour. Found this cool chart at “Maria Mind Body Health.” Maria Emmerich has given me permission to post it here for you, my wonderful patients and followers.
We use many of Maria’s recipes in my home, but occasionally you may want to convert your own recipe and this chart will help. My wife is the cook in our family, and probably already knows how to do this, but for those just beginning your ketogenic journey, this will be a big help in recipe conversion.
I’ve had patient’s ask me in the room how to substitute for flour. Here’s the answer. Remember, you have to double the eggs per cup. Thanks Maria!!
As a family practice physician and bariatrician, my job is to examine and treat the “Diseases of Civilization.” The Diseases of Civilization are those diseases arising out of the changes induced by industrializing and modernizing a society of people. These include diseases like diabetes, dyslipidemia (abnormal cholesterol), heart disease, hypertension, gout, vascular disease, & stroke. It is interesting that the so called Diseases of Civilization didn’t really appear on the scene until the early 1900’s. Yes, we have now identified some of these diseases in the early Egyptians, but to my point, as a society modernizes or industrializes, certain types of disease begin to arise. The Canadian cardiologist William Osler, one of the founding professors of John’s Hopkins Hospital, documented the first “syndrome” associated with narrowing of the arteries causing heart disease at the turn of the 19th century, and in 1912, the American Cardiologist James Herrick is credited with the discovery that narrowed arteries cause angina, a form of chest pain with exertion.
Today we know that underlying each of these diseases is the phenomenon of insulin over production, which seems to arise between five and twenty years prior to the onset of the Diseases of Civilization. Metabolic Syndrome, Dysmetabolic Syndrome or Syndrome X is the name we’ve given to the presentation of three or more of these diseases at once in one person. There is still argument as to whether insulin over production is the chicken or the egg, but what I see clinically has convinced me that insulin is culprit.
May 2013 Metabolism “Insulin Resistance: An adaptive mechanism . . .” 62(5):622-33. doi: 10.1016/j.metabol.2012.11.004. Epub 2012 Dec 20.
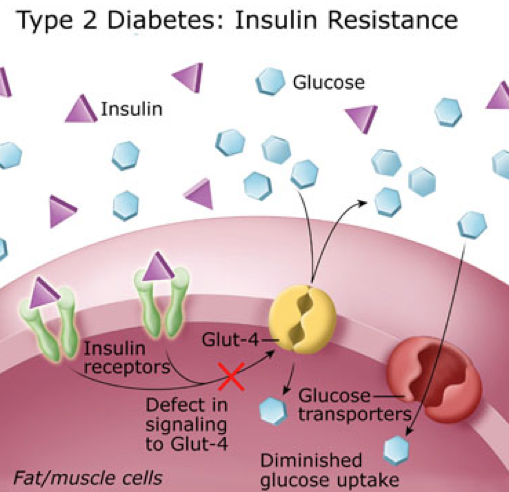
Insulin is a very powerful hormone that acts as a key, opening a door in just about every cell in the body, letting glucose (the primary form of fuel derived from carbohydrate) into the cell. For reasons that appear to be genetic, this key becomes “dull” in a portion of the population and does not unlock the door fast enough to lower the blood sugar. So, the body panics, and stimulates production of additional insulin, 2-10 times more in many people. However, the insulin that was produced initially, eventually kicks in. This extra insulin, acting at a slower rate, is the underlying culprit to the Diseases of Civilization.
How, you ask? Let me explain.
Insulin does more than just open the door for glucose.
1. Insulin causes weight gain. It turns on the storage of fat by activating an enzyme called lipoprotein lipase, pulling the triglycerides out of the cholesterol molecules and depositing them in the adipose tissue (fat cells).
2. Insulin raises cholesterol. It drives increased triglyceride production in the liver, especially in the presence of fructose.
3. Insulin triggers atherosclerosis. Triglycerides are essentially the passenger in the LDL (bad cholesterol) molecule. Higher triglycerides cause increased LDL production leading to increased atherosclerosis (narrowing of the arteries).
4. Insulin causes gout & kidney stones. Insulin increases uric acid production and in a round about way can increase calcium oxylate as well, increasing the risk of kidney stones and gout.
5. Insulin raises blood pressure. Insulin stimulates the retention of sodium, causing and increase in blood pressure.
Tiffini & Jazz riding near the top of the White Tank Mountains
6. Insulin makes inflammation worse. Insulin drives the inflammatory cascade and increases free radicals, and stimulates the inflammatory hormones causes arthritis, allergic rhinitis, psoriasis, dermatitis, and inflammatory bowel problems to be amplified.
My intent is not to demonize insulin. It is an essential hormone, however, when five to ten times the normal amount of insulin is being produced, you’re going to amplify the problems above by five to ten times normal. Type II Diabetes is really just a consequence of 15-20 years of over production of insulin.
This isn’t just something that affects humans. either. We have been seeing this in other species of the animal kingdom as well. Take for example my wife’s horse, Jazz. She’s a beautiful grey Arab/Saddle-Bred who kept having problems with laminitis, or more colloquially known as “founder.” Her diet consisted predominantly of alfalfa at the time, considered a moderate starch containing form of feed.
Laminitis is a progressively increasing tenderness to the hoof of horses or cattle that can be disabling and if not treated appropriately can cause permanent lameness in the animal. Recent literature in the veterinary world have identified that animal diets high in starch have a propensity to cause laminitis as well as colic. First identified in the equine community in the 1980’s with glucose tolerance tests, insulin resistance has been identified as a significant factor in hoof disease. The use of Corn, Oats, Barley or even Alfalfa as a primary form of feed for a horse with insulin resistance greatly increases the risk of laminitis.
Like Jazz, many horses in the arid Arizona climate are fed primarily with oats and alfalfa. Jazz was tested and found to have insulin resistance. Since Jazz has been placed on a much lower starch containing feed, she has had no further problems with laminitis. We converted all our horses to Bermuda grass.
Bailey, Jazz, Nayha & Houdini grazing in the back pasture
Our family and our horses are all now on Low-Carb diets to some degree and have been for the last seven years. No further hoof problems with the horses, and 55 lbs of weight loss with normalization of cholesterol in their owner, me.
Trail Riding in the White Tank Mountains
For those with interest, studies reveal feeds in order of the highest to lowest starch (carbohydrate) content to be: Sweet Feed, Corn, Oats, Barley, Wheat Bran, Beat Pulp, Alfalfa, Rice Bran, Soybean hulls, Bermuda Grass. Take a look the Low Carbohydrate help section in the menu above to see the carbohydrate content of many of the foods for human consumption.
It’s time we recognize that our diet and lifestyles have lead us to the Diseases of Civilization, and those diets and lifestyles have even effected our animals.
When you visit your doctor, he or she will probably measure your height and your weight. Then a Body Mass Index (BMI) will be calculated and placed on your chart. The BMI has actually become one of the standard “vital signs” required at a doctor visit over the last five years. This was not something that physicians started measuring on their own, it is a required measurement most health insurance plans insist upon before they will pay for the visit. BMI is an interesting and arguably worthless measurement. It was developed by a Belgian physicist by the name of Adolphe Quetelet some time between 1830-1850. Quetelet was a “Social Physicist,” trying to combine probability and statistics with the study of sociology (1). BMI was originally called the “Quetelet Index” and was designed specifically to measure averages among large populations in sociology or epidemiological studies (2).
BMI = mass (kg) / [height (m)]²
However, it wasn’t Quetelet that got BMI placed on the medical chart. BMI was made popular by the infamous Ancel Keys (the same Ancel Keys responsible for the flawed Seven Countries Study) in his July 1972 article published in the Journal of Chronic Disease. Ancel Keys, himself, explicitly stated that BMI was designed specifically for population studies, and inappropriate for evaluation of individual health (2). But, because of the ease of measurement, and the fact that Life Insurance companies had been using BMI to set your insurance premiums since the 1970’s, Health Insurance companies adopted it as a measure of overall health. In 1985, because BMI found great favor in epidemiological research, the National Institutes of Health (NIH) adopted it as the method to identify and define obesity in patients. And, in 1998 the NIH identified the BMI cutoffs – 25 for overweight, 30 for obesity – as easy numbers that could be remembered and used to counsel patients on weight reduction and health.
The problem with BMI is that it doesn’t actually identify a person with excessive fat accumulation. BMI is a height to weight ratio. It doesn’t account for fat at all. Using the NIH guidelines, the Terminator, with an estimated BMI of 31, would be considered obese. (You try telling the Terminator that he is obese, and see what happens.) Because, muscle weighs twice as much when compared to an identical volume of fat, Mr. Schwarzenegger (or anyone with increased muscle mass), will have a higher scale weight. This raises the BMI calculation, giving a false indication of increased health risk.
I was recently asked about a study published in The American Journal of Medicine that was recently commented on in Scientific American regarding BMI vs Muscle Mass as a predictor of longevity. The assumption is that just because your doctor measures BMI, it must be a great tool predicting health outcomes. The assumption is absolutely wrong. We know from multiple studies, including the article sited above, that increase muscle mass increases overall health, decreases the likelihood of insulin resistance and diabetes, reduces the risk of heart disease, and extends longevity. How can a measure of height to weight predict longevity? It can’t. The only reason BMI is on the medical chart, thanks to the NIH, is so that the physician gets paid.
In actuality, the most effective way of measuring a persons health is to simply measure body fat. This can easily be done by measuring waist circumference with an inexpensive tape measure. It can also be done with a simple bioelectrical impedance measurement. The gold standard for measuring body fat is to strip you down naked and dip you in a tub of water, measuring the water displacement. (I have very few patient’s that will return to my office after doing that, so we don’t use it very often, but it is effective).
The answer to the question is “NO,” the Terminator is NOT obese. And, if he shows up in my office, I’m not going to comment about his BMI.
1. Eknoyan, Garabed (2007). “Adolphe Quetelet (1796–1874)—the average man and indices of obesity”. Nephrology Dialysis Transplantation23 (1): 47–51.
2. Keys, Ancel; Fidanza, Flaminio; Karvonen, Martti J.; Kimura, Noboru; Taylor, Henry L. (1972). “Indices of relative weight and obesity”. Journal of Chronic Diseases25 (6–7): 329–43
Many patients come to my office desiring to loose weight, but complain of no self-control. They feel they cannot loose weight because they don’t have the willpower. Willpower, or self-control, is an elusive and mysterious thing. “If only I had more self-control,” I hear people say, “I could . . . ” exercise regularly, eat right, avoid drugs and alcohol, save for retirement, stop procrastinating, achieve a noble goal, or loose weight. A 2011 American Psychological Association study reveals that almost 30% of those interviewed felt that lack of willpower was the greatest barrier to making a change in any of these areas.
So what is “willpower” or “self-control?” It is the ability to resist short-term temptations in order to fulfill a long-term goal.
I meet and work with people every day who feel they have no willpower. In actuality, will power and self-control are learned behaviors that develop over time. Anyone can have willpower, you just have to understand how willpower in certain areas can be strengthened and what makes it weak. In fact, a 2005 study showed that self-discipline or willpower was more important than IQ in academic successes. This study also found that increased self-discipline lead to less binge eating, higher self-esteem, higher grade point averages, better relationship skills and less alcoholism. Fascinating isn’t it!?
The answer can be found in a quote from Henry P Liddon, “What we do upon some great occasion will probably depend on what we already are; and what we are will be the result of previous years of self-discipline.” This means that willpower or self-control can be learned or improved. How, you ask?
First, you must establish and write down a reason or motivation for change. In addition, that change must fulfill a clear goal. Just wanting to loose weight isn’t good enough. You have to be motivated because of a consequence that arises from the obesity or overweight. And, you “loosing weight” isn’t a clear goal. You must set a weight reduction goal. It has to be clearly written down with your motivational reason. Willpower or self-control cannot begin to form until these two steps occur.
Second, you must begin to monitor your behavior toward that goal. When it comes to weight loss, I ask every one of my patient’s to keep a diet journal. In this journal they are asked to write down every thing they eat and drink. The night before, they are to write down their plan for tomorrow’s meals, then the next evening, they account for their success or failure by journaling on that same page what they actually ate and drank, then after comparing what they did, they plan for tomorrow and journal why they were successful or why they weren’t. It’s the last part that is so powerful, a short 3-5 minutes of self-introspection. Self-introspection is the key to behavioral change. It is the key that allows a person to see their habits and then make very small changes that break bad habits, solidify good habits and strengthens willpower.
Third, willpower is developed over time. It is developed by being accountable to ones-self on very little things every single day. But it MUST be written down. If I planned to eat bacon and eggs for breakfast and I didn’t, why? When I look at my day, I may realize that I went to bed too late to get up early and cook bacon and eggs. So, instead, I ate a yogurt that was in the fridge. I am accountable to myself. If I plan to eat bacon and eggs tomorrow, I must either go to bed earlier, prepare them the night before, or throw out the yogurt . . . so not to be a temptation again. This is written down and I make a very small change tomorrow.
Over time, this self-introspection becomes easier and easier, to the point that you do it sub-consciously. It is this sub-conscious self-introspection and change will be seen by others as self-control or willpower. Just like a working or strengthening a muscle, recording short goals and and accounting for them makes your self-discipline stronger. The self-discipline muscle becomes more powerful. In time, a split second decision not to binge on that piece of cake will be seen as strong willpower by those around you. You’ll recognize that it’s just flexing your self-discipline muscle.
So, my next question to you is . . . where’s your diet journal?
How are your stress levels lately? Are you struggling with your finances? Struggling with your job? Do you have troubles in your personal relationships? Are you carrying a heavy load in school? Do you have a horse that just won’t behave?
Many of my patients will routinely experience weight loss plateaus due to stress. Most of them want to know how and why this occurs. The simple answer is this: our bodies are designed with a “fight or flight” response.
If you’re in the woods and you stumble upon a bear, the sudden recognition of significant danger will stimulate an immediate release of protective hormones into your blood stream including adrenaline and cortisol. (Your brain also know that those extra few donuts you ate will make you quite the tasty treat for the bear.)
Fight or Flight Causes Glucose in the Blood Stream
Adrenaline increased your heart rate, dilates the blood vessels to your muscles and increases your respiratory rate. Cortisol is the hormone that stimulates increased glycogen release from the liver. Glycogen is a form of sugar made available so that you can immediately fight the bear or run from the bear. The glycogen response raises your insulin level so that that fuel can be pulled right into the cells needing it. The adrenalin and cortisol, among other hormones, are released so that blood can be shunted from your stomach and intestines to your muscles and brain to more effectively enable you to finish fighting the bear, or out run that drooling growling bear hot on your heels.
Modern Bears
Most of us will never “stumble across a bear.” However, your boss may confront you about how you handled a recent assignment or may drop an extra pile of work on your desk. You may run short on your finances this month, have a serious disagreement with your significant other, or someone may cut you off in traffic causing a near accident. Any or all of these stimulate the identical “fight or flight” response. Whether it is an actual bear or the stress from traffic, the same adrenalin and cortisol response occurs.
Chronic Cortisol Release & Weight Gain
How does that keep you from loosing weight? The elevated cortisol causes a cascade effect raising your insulin levels. Insulin will remain effectively elevated in the blood stream for the next 2-12 hours. Insulin is the primary hormone driving and stimulating weight gain. If you’ve had 2 or 3 stressful events throughout the day, and you have not had the opportunity to physically burn off these stress response hormones, your body will store and/or continue to gain weight throughout the entire day. If you have been trying to loose weight, the spike in the insulin from this cortisol cascade halts the weight burning process and may actually bump you out of ketosis (the process by which we burn fat as the primary fuel source) for the next 4-12 hours.
Mitigating Daily Stress
How do you prevent this from happening? A simple 15-20 minute walk 3-5 times per week is enough to decrease the stress hormone surge that occurs from a “fight or flight” response. Any regular exercise program will decrease these stress hormones. Adequate sleep also decreases these hormones.
Berberine, the active ingredient in tumeric, is also helpful in controlling blood sugar spikes and helping those with insulin resistance to handle stress and inflammation. I’ve been using berberine daily for years personally and with many of my patients. I love it so much, I designed my own formulation. You can find it along with my other supplement line at ketoliving.com.
If your job, school or life is stressful, incorporating an exercise program as simple as a daily walk for 15-20 minutes per day will keep the proverbial “bear in the woods” from catching up to you because of your weight. Controlling your blood sugar is the other key. The correct diet and supplements play a huge role combined with exercise.
Check out my diet page if you’d like a copy of my ketogenic dietary program. Check out my YouTube page for hundreds of free videos and DocMuscles.Locals.com for additional information for my followers. And, look at my membership programs available here.
My amazing wife, among her many talents, makes a wonderful low carb cheese cake. She has taken the recipe found in Maria Emmerich’s “Secret Weight Loss Recipes” and modified it to our family’s taste. It has quickly become one of my family’s favorites.
Preheat oven to 350F. Mix cream cheese, sweetener, protein and vanilla with an electric mixer until blended. Add eggs one at a time, mixing on low after each until blended. Blend in sour cream and pour over crust. Place a pan of water on the lower rack place cheesecake on rack above. Bake for approximately 45 minutes until set. Watch carefully!
Refrigerate overnight.
Freezes well too!
My wife will often bake them in individual sized pans (as in the picture above) so that I can pull one out of the freezer, let it thaw and cover it in whip cream and a sprinkle of berries. Tastes fantastic!
I love chocolate chip cookies! However, over the last seven years, as I have followed a low carbohydrate diet I have not been able to indulge my chocolate chip cookie craving — until recently.
My gorgeous and very ingeniousness wife has perfected her chocolate chip cookie recipe and – Oh, WOW . . .are they good.
Warm, tasty chocolate chip cookies that are actually good for you, served up by a beautiful blond in a very cute apron. . . I think this is what heaven is like.
Low Carb Chocolate Chip Cookies
Here is a snapshot of the remaining batch my wife made at our house the other day before they got eaten. Boy, are they good. Here is the recipe:
Low Carbohydrate Chocolate Chip Cookies
1 tsp vanilla
2 eggs
2 sticks (1 cup) of butter, softened
1/2 cup Sweet Perfection
1/4 cup erythritol
1/4 cup Just Like Sugar (chicory root sweetener)
1 tsp salt
1 tsp baking soda
1 tsp baking powder
1 1/2 cup almond flour
1 cup coconut flour
1/2 cup Carbalose flour
2 ChocoPerfection Milk Chocolate bars chopped
Mix the vanilla, eggs, butter and sweeteners until creamy or fluffy. Add in all dry ingredients and mix. Add chocolate and mix. Place dough on parchment paper covered cookie sheets in 2 tsp sized scoops.
As a bariatrician, I think about fat all the time. I guess you could say I have a lot of “fat thoughts.”
I frequently hear patient’s tell me, “Dr. Nally, I’m eating RIGHT, but I’m just NOT losing weight!”
If you’re not losing weight, your not eating correctly. 99% of your weight loss success is related to your diet. We have been poorly misinformed over last 40 years as to what a “correct” diet contains. We’ve been told to follow a low fat diet for the last 40-50 years. However, it is very apparent as patient’s follow a low fat diet that only a small percentage of them have success in weight loss, and the majority actually gains more weight and remains significantly hungry. When you look at the body’s physiology, fat restriction only stimulates increased hunger. The intake of any form of carbohydrate, whether that be simple or complex, stimulates an insulin response. Based on our genetics, that insulin response can be variable. some of us respond normally and others respond with between 2-10 times the normal insulin surge. Insulin is actually the hormone that drives weight loss or weight gain.
You and I will not be able to effectively lose weight until we control the response of insulin, and this can only be done through carbohydrate restriction.
You know, Dr. Seuss was right, the whole egg is actually good for you.
A recent study from the University of Connecticut demonstrated that eating the whole egg actually decreases LDL (the bad cholesterol) sub-particles and insulin resistance in Metabolic Syndrome better than the egg white or the egg substitute.
I like green eggs and ham!
I do!! I like them, Sam-I-am!
And I would eat them in a boat!
And I would eat them with a goat…
And I will eat them in the rain.
And in the dark. And on a train.
And in a car. And in a tree.
They are so good so good you see!
As a medical bariatrician and family practitioner specializing in low-carbohydrate diets, I often see the panic stricken look on people’s faces when they look at their cholesterol profiles just after starting a carbohydrate restriction life-style.
First, it is very important to understand that if you check your cholesterol within the first 4-6 weeks of dietary changes, there will be a transient rise in the cholesterol profile as your adipose tissues (fat cells) release your new fuel source into the blood stream and the mitochondria in the one trillion cells in your body convert from the use of glucose to the use of ketones (derived from triglycerides) as the primary fuel source. This is not a problem as the body is designed to handle this increase in triglyceride and cholesterol. I explain to patient’s that we are essentially making the figurative change from “un-leaded fuel to diesel fuel.”
Second, the standard cholesterol profile does not give you a true picture of what is occurring at a cellular level. The standard cholesterol panel checks Total cholesterol (all the forms of cholesterol), HDL (the good stuff), LDL-C (the bad stuff) and triglycerides. It is important to recognize that the “-C” stands for a calculation usually completed by the lab.
Cholesterol Particle Sizes
Total cholesterol, HDL and triglycerides are usually measured and LDL-C is measured using the Friedewald equation [LDL = total cholesterol – HDL – (triglycerides/5)].
Third, it is also important to realize that HDL and LDL are actually transport molecules (the buses for the triglycerides (the passengers). HDL is taking triglycerides to the fat cells and LDL is taking triglycerides from the fat cells to the muscles and other organs for use as fuel.
When you being a low carbohydrate diet, your blood glucose availability as the primary fuel source drops and triglycerides become the primary source. It takes your body 4-6 weeks to increase the number of mitochondria necessary to effectively use triglycerides as the primary fuel. (This is why many athletes and patients who are active will feel slightly sluggish during their exercise for the first few weeks).
Once your body accommodation to the new fuel, there will be a notable drop in LDL-C and a rise in the HDL.
But this still doesn’t answer the question and relieve the panic seen above. A deep sigh and the look of relief occurs when I explain that LDL-C doesn’t give us the real story.
To make it simple and understandable, LDL is made up of three main sub-types big fluffy ones, medium sized ones, and small dense ones. It’s the small dense ones that contain lipoprotien A [Lp(a)] found in increased vascular risk. Recent studies reveal that heart disease and atherosclerosis is caused by the small dense LDL molecules.
A low carbohydrate diet causes the small dense cholesterol to drop and there is a rise in the two other sub-types This shift in sub-types can actually elevate the Total Cholesterol number and occasionally the LDL-C.
If you are following a low carbohydrate diet, get your cholesterol levels checked. It is more ideal to get an NMR Lipoprofile or VAP Cholesterol test that will give you an LDL particle number and this can be explained more fully by your doctor.
Now, off to the fridge . . . where did I put that package of bacon . . . ?








 People with significant stressors in their life have been show to have a raised cortisol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing an over production of cortisol and normalization of their cortisol levels occurs after resolution of the stressor. This cortisol response is not high enough to lead to a true
People with significant stressors in their life have been show to have a raised cortisol secretion. Chronic stress induces hyperactivity of the hypothalamic-pituitary-adrenal axis causing an over production of cortisol and normalization of their cortisol levels occurs after resolution of the stressor. This cortisol response is not high enough to lead to a true 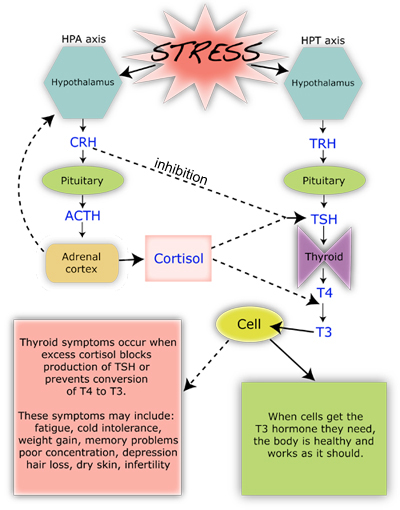 Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues and turns on the maturation process of adipocytes (fat cells). In the process, it suppresses the immune system to decrease inflammation during times of stress (7,8,9). In the short run, this is an important process, however, when cortisol production is chronically turned up, it leads to abnormal deposition of fat, increased risk of infection, impotence, abnormal blood sugars, head
Under a stress response, cortisol turns on gluconeogensis in the liver (the conversion of amino acids into glucose) for fuel. Cortisol, also, shifts the storage of fats into the deeper abdominal tissues and turns on the maturation process of adipocytes (fat cells). In the process, it suppresses the immune system to decrease inflammation during times of stress (7,8,9). In the short run, this is an important process, however, when cortisol production is chronically turned up, it leads to abnormal deposition of fat, increased risk of infection, impotence, abnormal blood sugars, head
 as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
 before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).
before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).