The most common complaint that I get in my office when someone has started a ketogenic diet is, “Doc, I feel fatigued. Will this ever go away?”
That feeling of fatigue, some refer to as the “keto-flu,” is usually due to a couple of things. First, you may not be eating enough fat (I recommend a 1 gram to 1 gram ratio of protein to fat when getting started). Second, you’re not taking in enough salt (specifically sodium, potassium, magnesium and/or zinc). These four salts are essential electrolytes our body requires for proper function.
If salt is the problem, the you will be experiencing leg cramps. Cramps during daytime activity are usually due to low sodium or potassium levels. Cramps that wake you up at night are usually due to low magnesium or zinc. Leg cramps can also be due to hypothyroidism or significant blood sugar swings. Dr. Nally will usually check for this during your visit with him.
“But isn’t too much salt bad for you?” I am frequently asked.
Too much salt is only bad for you if you’re eating a “low-fat” diet.
What if increasing salt intake actually lowered your blood pressure?
Did you know that increasing your salt intake can actually improve your diabetic blood sugar if you are following a correct diet? Could it be that easy?
Almost every patient that I see in the office has a significant worry about salt intake, some greater than others. In fact, some people are so fearful about salt that when I initially began encouraging its use, they told me that I was crazy, and they left my practice.
Has restricting salt over the last 50 years really worked, or is it doing more damage than we think?
That was the question that was asked by Dr. Ames in the American Journal of Hypertension 17 years ago. However, his answer never got a mention. In fact, I’ve been in practice for almost 20 years, and incidentally stumbled upon this article when it was mentioned by a colleague of mine. Granted, the study is a small sample size of people, only twenty-one. However, the results are profound.
Twenty-one patients with hypertension were randomized to periods of no salt (placebo) and periods of 2 grams (2000 mg) of sodium chloride four times a day (a total of 8 grams of salt per day). Glucose tolerance tests were completed with insulin levels at the end of each intervention period.
Insulin Resistance and Hypertension Improve by Adding Salt
Three very noteworthy results happened. First, those patients with insulin resistance and diabetes had improvement in their glucose levels while on 2 grams of sodium supplementation.
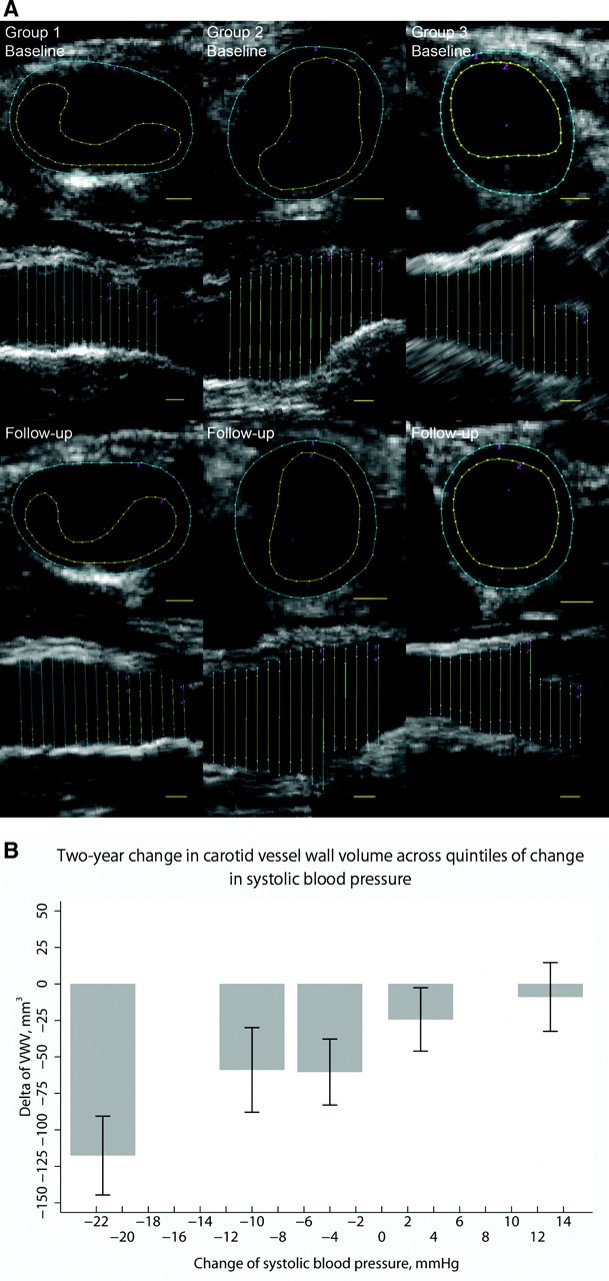
Second, those with hypertension also, shockingly, showed improvement in their blood pressure while on the 2 grams of sodium supplementation.
Third, those with insulin resistance had a lowering of their insulin levels during the period of increased sodium intake. These findings fly in the face of the dogma that’s been drilled into our heads that “salt is bad!”
“But, Dr. Nally, you can’t base your findings on a small group of 21 people,” the experts say.
Yes, it is a small study group. However, these findings are identical to what I, also, see clinically every day in my practice for over 20 years.
We know that the average human needs at a minimum 3 grams of sodium per day and 3 grams of potassium per day. The standard American diet (SAD diet) including processed foods contains 2-3 grams per day of sodium and potassium. In fact, the CDC claims the worst salt containing meals for you are:
- Bread
- Processed chicken dinners
- Pizza
- Pasta
Insulin also stimulates additional retention of sodium at the kidney level. If you are insulin resistant, producing excess insulin in response to starches or sugars, you retain notably larger amounts of salt when eating the standard American diet (SAD diet) or a “low-fat” diet. However, if your following a low-carbohydrate or ketogenic lifestyle, you won’t be eating the meals above and you’re probably not getting near enough salt.
Salts, or electrolytes, are essential in normal cellular function. Low salt in the body is like running your car without oil. It will run, but not very efficiently and over the long term will cause problems. This is the cause of the keto-flu I wrote about previously. And, according to the study above, it is a potential driver of our persisting insulin resistance, diabetes and hypertension.
How Much Salt Should I Use?
In my office, I encourage use of 3-4 grams of sodium and 3-4 grams of potassium daily when using a ketogenic lifestyle. That’s approximately 1 ½ – 2 teaspoons of salt per day. I like the Redmond’s RealSalt or pink Himalayan salt because these products contains all four types of salt (sodium, potassium, magnesium and zinc).

It is probably that your salt restrictions is making your insulin resistance and blood pressure worse. That’s what the clinical evidences are pointing toward, and it is what I see every day in my office.
Want to know more about a ketogenic life-style? Click the KetoLife link to get some basics.
If you’re already following a ketogenic lifestyle, then let me help you navigate the bumps and turns by going to the KetoKart and checking out the products I recommend to jump-start ketosis DocMuscles-style!
Until then, I’ll have another piece of bacon, please . . . and, oh, pass the salt!














 raise insulin levels without raising blood sugar and are not appropriate for use with a true low-carbohydrate/ketogenic diet. You can see and print the article I published clarifying which sweeteners you can use and which ones to avoid here:
raise insulin levels without raising blood sugar and are not appropriate for use with a true low-carbohydrate/ketogenic diet. You can see and print the article I published clarifying which sweeteners you can use and which ones to avoid here:









 the underlying cause. I see this problem in a very large majority of the people in my office and I am seeing people younger and younger show up with continually increasing blood pressure.
the underlying cause. I see this problem in a very large majority of the people in my office and I am seeing people younger and younger show up with continually increasing blood pressure.

 begin to back down their blood pressure medications, they would experience symptoms of dizziness, light-headedness, headache and a few patient’s nearly passing out. On a low-carbohydrate, high-fat (ketogenic) diet you need salt (sodium, potassium, & magnesium).
begin to back down their blood pressure medications, they would experience symptoms of dizziness, light-headedness, headache and a few patient’s nearly passing out. On a low-carbohydrate, high-fat (ketogenic) diet you need salt (sodium, potassium, & magnesium).