
You don’t want to miss this event . . . Space is limited so RSVP TODAY!!

You don’t want to miss this event . . . Space is limited so RSVP TODAY!!
I will be starting a twice weekly exclusive live-stream here for my amazing online followers and patient who are participating in the KetoClan Group on the following sixteen topics next week. Will be sharing the basics and my 22 years of clinical experience with each of these topics as it relates to health and weight management. These topics will take 10-30 minutes, then giving the remainder of the hour to you to ask questions.

The topics we will cover over the next 8 weeks are listed below:
1. Insulin
2. Monitoring Glucose – CGMs
3. Fat Adaptation
4. Things that make insulin go “bump in the night (or the day)” – (sweeteners, creamers, teas, Resveratrol, nuts, etc)
5. Protein
6. Basic Thyroid Function
7. Female Hormones
8. Male Hormones
9. Testing Ketones in Urine, Breath, Blood
10. Ketoacidosis
11. Medications and ketogenic diets (Metformin, DPP4s, GLP-1, SLT-2s, sulfonoureas, Berberine)
12. Stress – Cortisol & DHEA
13. Exercise – Cardiovascular and Resistance Exercise
14. Sleep
15. Food Cravings and the Subconscious Mind
16. Keto, Carnivore or Fasting – What should I be doing?
Not a member yet? Sign up here.

I’ve been told that many of you have nominated me. Thank you!!!
Every year Ketogenic.com hosts the Keto Awards with Metabolic Health Summit to highlight some of the best and brightest in our community.
There are five unique categories in which you can nominate and it would be an honor to me for you to add your vote:
Top Keto Educator
Top Keto Book
Top Keto Podcast
Top Keto Researcher
Making Positivity Louder
I’ll be sure to let you know who is selected.
Please take a minute to cast your vote for me.
Vote Here:

What is the cause of abdominal bloating when following a ketogenic or low-carbohydrate diet?
Over the last few months, our fearless infectious disease leader, Dr. Anthony Fauci, and the Ivory Tower of medical journals, the New England Journal of Medicine, have clearly informed us that mask wearing by the healthy is little more than symbolic ‘Virtue Signaling.’
For those Karen’s and Felicia’s who have tried to shout me down like a Tourette’s tick with ‘Social Media Science,’ in Wal-Mart, in the big box stores, at the gas station and at the burger shop, lets look closely at what the New England Journal of Medicine said on May 21, 2020.
We know that wearing a mask outside health care facilities offers little, if any, protection from infection. Public health authorities define a significant exposure to COVID-19 as face-to-face contact within 6 feet with a patient with symptomatic COVID-19 that is sustained for at least a few minutes (and some say more than 10 minutes or even 30 minutes). The chance of catching COVID-19 from a passing interaction in a public space is therefore minimal. In many cases, the desire for widespread masking is a reflexive reaction to anxiety over the pandemic.
So, why have we been ordered to wear are masks everywhere by mayors and governors and city officials across the country? Symbolism. Pure and simple symbolism. From that same NEJM article:
It is also clear that masks serve symbolic roles. Masks are not only tools, they also serve as a talisman [an object that acts as a charm to avert evil and bring good fortune] that may help increase health care workers’ perceived sense of safety, well-being, and trust in their hospitals.
The Surgeon General was widely mocked and ridiculed for suggesting in March that masks might even increase the spread of the virus. Yet, here, in the “journal of all medical journals,” the NEJM provides the same warning to mask-wearers:
What is clear, however, is that universal masking alone is not a panacea. A mask will not protect providers caring for a patient with active COVID-19 if it’s not accompanied by meticulous hand hygiene, eye protection, gloves, and a gown. A mask alone will not prevent health care workers with early COVID-19 from contaminating their hands and spreading the virus to patients and colleagues. Focusing on universal masking alone may, paradoxically, lead to more transmission of COVID-19 if it diverts attention from implementing more fundamental infection-control measures.
However, suddenly on June 17th, 2020, Dr. Fauci suddenly changed his tune, and contrary to all the scientific evidence and over 50 years of medical literature on the subject, said wearing a mask is “better than nothing.” Within weeks, executive orders for mask wearing were signed across the nation.
The argument should have been over. Anyone advocating for universal mask wearing by the healthy, according to all the mask wearing literature, is merely engaging in virtue signaling, not actual public health.

Cities and states across the nation have mandated mask wearing (some even advocate using bananas). I’m not telling you to break the law. I am saying that the mask mandate has done nothing to “slow the spread” as so many people have now bought into. Research demonstrates that homemade masks do little to stop the spread of viral infections. It also demonstrates that properly fitted surgical masks worn correctly decrease this risk of viral spread in a highly controlled setting at the very best by only 2-5%.
In the most recent comprehensive review of the mask wearing literature, the authors stated, “The evidence is not sufficiently strong to support widespread use of face-masks as a protective measure against COVID-19. However, there is enough evidence to support the use of face-masks for short periods of time by particularly vulnerable individuals when in transient higher risk situations.”

What is effective is washing your hands regularly with soap and water, avoiding those who are actually sick or have fevers over 101 degrees, eating a healthy diet that prevents diabetes risk and getting adequate sleep. Those at high risk for infection can and should be vigilant about avoiding exposure to those who are sick.
For the rest of us, it’s time to unmask. I, myself, struggle daily to maintain enough virtue in my bones for myself, let alone signal others about it all day long.

The most common complaint that I get in my office when someone has started a ketogenic diet is, “Doc, I feel fatigued. Will this ever go away?”
That feeling of fatigue, some refer to as the “keto-flu,” is usually due to a couple of things. First, you may not be eating enough fat (I recommend a 1 gram to 1 gram ratio of protein to fat when getting started). Second, you’re not taking in enough salt (specifically sodium, potassium, magnesium and/or zinc). These four salts are essential electrolytes our body requires for proper function.
If salt is the problem, the you will be experiencing leg cramps. Cramps during daytime activity are usually due to low sodium or potassium levels. Cramps that wake you up at night are usually due to low magnesium or zinc. Leg cramps can also be due to hypothyroidism or significant blood sugar swings. Dr. Nally will usually check for this during your visit with him.
“But isn’t too much salt bad for you?” I am frequently asked.
Too much salt is only bad for you if you’re eating a “low-fat” diet.
What if increasing salt intake actually lowered your blood pressure?
Did you know that increasing your salt intake can actually improve your diabetic blood sugar if you are following a correct diet? Could it be that easy?
Almost every patient that I see in the office has a significant worry about salt intake, some greater than others. In fact, some people are so fearful about salt that when I initially began encouraging its use, they told me that I was crazy, and they left my practice.
Has restricting salt over the last 50 years really worked, or is it doing more damage than we think?
That was the question that was asked by Dr. Ames in the American Journal of Hypertension 17 years ago. However, his answer never got a mention. In fact, I’ve been in practice for almost 20 years, and incidentally stumbled upon this article when it was mentioned by a colleague of mine. Granted, the study is a small sample size of people, only twenty-one. However, the results are profound.
Twenty-one patients with hypertension were randomized to periods of no salt (placebo) and periods of 2 grams (2000 mg) of sodium chloride four times a day (a total of 8 grams of salt per day). Glucose tolerance tests were completed with insulin levels at the end of each intervention period.
Insulin Resistance and Hypertension Improve by Adding Salt
Three very noteworthy results happened. First, those patients with insulin resistance and diabetes had improvement in their glucose levels while on 2 grams of sodium supplementation.
Second, those with hypertension also, shockingly, showed improvement in their blood pressure while on the 2 grams of sodium supplementation.
Third, those with insulin resistance had a lowering of their insulin levels during the period of increased sodium intake. These findings fly in the face of the dogma that’s been drilled into our heads that “salt is bad!”
“But, Dr. Nally, you can’t base your findings on a small group of 21 people,” the experts say.
Yes, it is a small study group. However, these findings are identical to what I, also, see clinically every day in my practice for over 20 years.
We know that the average human needs at a minimum 3 grams of sodium per day and 3 grams of potassium per day. The standard American diet (SAD diet) including processed foods contains 2-3 grams per day of sodium and potassium. In fact, the CDC claims the worst salt containing meals for you are:
Insulin also stimulates additional retention of sodium at the kidney level. If you are insulin resistant, producing excess insulin in response to starches or sugars, you retain notably larger amounts of salt when eating the standard American diet (SAD diet) or a “low-fat” diet. However, if your following a low-carbohydrate or ketogenic lifestyle, you won’t be eating the meals above and you’re probably not getting near enough salt.
Salts, or electrolytes, are essential in normal cellular function. Low salt in the body is like running your car without oil. It will run, but not very efficiently and over the long term will cause problems. This is the cause of the keto-flu I wrote about previously. And, according to the study above, it is a potential driver of our persisting insulin resistance, diabetes and hypertension.
How Much Salt Should I Use?
In my office, I encourage use of 3-4 grams of sodium and 3-4 grams of potassium daily when using a ketogenic lifestyle. That’s approximately 1 ½ – 2 teaspoons of salt per day. I like the Redmond’s RealSalt or pink Himalayan salt because these products contains all four types of salt (sodium, potassium, magnesium and zinc).

It is probably that your salt restrictions is making your insulin resistance and blood pressure worse. That’s what the clinical evidences are pointing toward, and it is what I see every day in my office.
Want to know more about a ketogenic life-style? Click the KetoLife link to get some basics.
If you’re already following a ketogenic lifestyle, then let me help you navigate the bumps and turns by going to the KetoKart and checking out the products I recommend to jump-start ketosis DocMuscles-style!
Until then, I’ll have another piece of bacon, please . . . and, oh, pass the salt!

Do you have the keys to your “fat lock-box?”
Lock-boxes have always fascinated me. Lock-boxes with special keys are even more fascinating. The more I’ve learned about fat cells (adipocytes), the more I think about them as special fuel depositories or fat lock-boxes. Before the invention of refrigerators, fast-food, Bisquick and beer, our bodies preserved and reserved fat as a precious commodity.
The body, when given fat with carbohydrates or excess protein, quickly places the fat into a lock-box for safe keeping. It does this for two reasons. First, the body can store fat very efficiently. Second, hormone signals stimulate fat storage when other fuel sources (carbohydrate & protein) are present in excess. The body can access this stored fuel only when the right presentation of hormonal keys are present. Fascinatingly, we now know from recent research, there are actually three types of lock-boxes for fat in the human body (white adipose tissue, brown adipose tissue, and tan adipose tissue).
The greatest challenge for the obesity doctor is getting into the fat lock-box. Some people’s boxes are like the “Jack-in-the-Box” you had as a child – just add a little exercise spinning the handle and the box pops open (These are those people that say, “Oh, just eat less and exercise and you’ll lose weight.”) For the majority of the people I see, it’s more like the lock above with a four or five part key required to turn the gears just right. (And, that key often only seems available on a quarter moon at midnight when the temperature is 72 degrees.) Fat cells, called adipocytes, require four, and possibly more, keys to open them up and access the fuel inside. Exercise is only one of those keys. However, exercise alone often fails.
Over the last 18 months, I have been surprisingly impressed with the results patients have by the addition of both medium chain triglycerides and exogenous ketones. A number of people have asked me, “Why do you encourage the addition of exogenous ketones to a person already following a ketogenic diet?”
Others just accuse me of self promotion, saying, “You’re just trying to sell a product!”
Or they exclaim, “Giving more ketones is just a waste of time and money.”
A few of the uneducated holler from across cyberspace, “You’re just going to cause ketoacidosis!”
Believe me, I’ve heard it all. And, the skepticism is understandable. I work with people every day, looking closely at weight gain/loss, metabolism, cholesterol, blood pressure, inflammation, etc. With any “low-carb” or “ketogenic product,” I test it out on myself and my family, before I offer it to my patients or even consider encouraging its use in my practice. I have this desire to understand “the how” and “the why” before I prescribe the who and when.
First , let’s talk about the adipocyte as a fat lock-box – and where you find the keys. Then, we’ll discuss how products may or may not help.
There is only one door INTO the adipocyte for the fat, and the key to that door is insulin. Insulin stimulates an enzyme called lipoprotein lipase that essentially pulls the fat from the cholesterol molecule into the fat cell. Without insulin, fat doesn’t enter the fat cell. As a result, type I diabetics (those that make absolutely no insulin) look anorexic if they don’t take their needed insulin. Insulin is also the first key to the back door on the adipocyte. Actually, if there is too much insulin in the system, fat enters easily through the front door but cannot exit the back door (Picture 1). Insulin seals up the back door so that fat cannot exit very effectively.
That’s why insulin is the master hormone when it comes to obesity. You’ve got to lower the over-all insulin load to get the adipocyte slowing fat entry and increasing fat exit. If you don’t do that, I don’t care how much you exercise, 85% of the population will struggle with weight loss. Hmmm, seems kind a familiar to the last 50 years of our obesity epidemic, No?

The second key to the back door of the fat cells are the catecholamines. These are adrenaline (epinephrine), norepinephrine, adrenocorticotropic hormone (ACTH) and even serotonin. These hormones are produced in the adrenal glands through exercise, fear and even recollection of powerful memories. Medications can also stimulate production of these hormones. The catecholamines stimulate cAMP. cAMP opens the fat cell, releasing fatty acids for fuel.

The thyroid hormone conversion of T4 to T3 also plays a role in uptake of the catecholamines by adnylyl cyclase (AC). Low levels of T3 (like those seen in hypothyroidism or in cases of thyroiditis) also inhibit unlocking of the fat lock-box. Conversion of T4 to T3 is driven by the presence of bile salts in the gut. Increase fat intake increases the presence of the bile salts which naturally leads to better T3 conversion. Hence my constant references to eating more fat and bacon. .
The third key is an inhibitory effect on adenylyl cyclase (AC) activity by alpha and beta adrenoreceptors, adenosine, prostaglandins, neuropeptide Y, peptide YY, HM74-R & nicotinic acid. These inhibitory and inflammatory hormones produced in the brain, gut and other areas decrease cAMP activity in the fat cell and slow fat loss. The fancy long names are all hormones causing inflammation. Of note, many are also stimulated by medications including blood pressure lowering drugs. Check with your doctor if the medications you are taking may be causing weight gain, or halting your weight loss.
Please note that the first three keys have effect on the cAMP pathway for release of fat from the adipocyte. These three keys turn on or off effective function of cAMP leading release of fatty acids from the fat cell.
The fourth key follows a separate pathway. This is why I’ve clinically seen patients experience weight loss even in the presence of higher insulin, inflammatory disease or hypothyroidism. This key activates release of the naturitic peptides (ANP, BNP). These hormones are released from the heart when it squeezes more powerfully. As the cardiac muscle contracts, it releases ANP & BNP hormones. These hormones stimulate the cGMP pathway in the adipocyte. It then activates hormone sensitive lipase (HSL) and perilipin to release free fatty acids. Again, this pathway is separate from the pathway by which the first three keys released fat. Exercise increases heart contractility, but is inhibited by high insulin levels. However, ketones themselves also stimulate this increased contractile effect.
There actually is a fifth key not referenced above. The fifth key to the fat lock-box amplifies testosterone’s presence through the HPG axis. Insulin resistance and leptin resistance lower testosterone in men and raise it in women, causing poly-cystic ovarian syndrome (PCOS). Normalizing insulin levels (with a ketogenic diet) while at the same time increasing ketones as the primary fuel powerfully resets the HPG axis through a complex series of hormonal reactions. Growth hormone is balanced and testosterone returns to a normal range.
Clinically, 60% of the people I see in the office have abnormal testosterone due to insulin resistance. This leads to hypogonadism in men and PCOS (abnormal periods, facial hair growth and/or infertility) in women. Restricting carbohydrates and maintaining nutritional ketosis by diet and/or addition of exogenous ketones has a powerful corrective factor in these people.
Testosterone influences the up-regulation of the alpha & beta adrenergic receptors (the 2nd & 3rd key above). Hence, if your testosterone is low, it has a suppression on the way that the catecholamines influence fatty acid release from the fat cells. If your testosterone and growth hormone are normal, muscle development and adrenaline stimulus from exercise helps amplify the use and mobilization of fat from the fat cell. In people with insulin resistance and leptin resistance, exercise and the catecholamines don’t have the same fat burning effect.
Yes, I have greatly simplified a series of very complex hormonal pathways in the explanation of the keys above. Why do you think understanding obesity has been so difficult? Think of your adipocytes as a fat lock-box.
What’s even more important is the knowledge that the fat cell DOES NOT open or close because of calories. There is no dogmatic calorie-meter on the wall of the fat cell. There is no calorie key to the fat lock-box. Really, . . . in the 50 years of studying fat, researchers haven’t found one. (Prove me wrong when you show me an electron micro-graph of a calorie-meter in the wall of a cell). Science has demonstrated multiple times that the lack of food from starvation or excessive fasting suppresses thyroid function (an inhibitory effect on key #3). Restricting calories actually inhibits fat loss in many people.
The fat lock-box keys I refer to above are hormone responses to the presence of macro-nutrients (food). That means, first reduce your carbohydrate intake by eating real food from good sources. You can learn how to get started by registering for my FREE six part weight loss mini-course. Second, be as active as you can. Third, reduce stress and medications that have inhibitory effect on catacholamines. Fourth, balance your thyroid. And, fifth, get into ketosis and consider adding exogenous ketones to your dietary regimen. It really is that simple.
(For those of you that still believe there is a calorie key – or just need something to do while in the bathroom):

Listen in to our live audience recording of KetoTalk Episode #69 while cruising around Alaska!
Questions You Can Find Answers to On This Podcast:
– Can your fasting blood sugar creep up if you’ve been low carb for a long time?
– What combination of electrolytes do you need to prevent leg cramps while keto?
– Should I use a keto diet to treat an immunosuppressed system?
– How does a keto diet effect someone with low stomach acid levels?
– Does plaque leave your arteries when you go keto, or do you have it forever?
– What is the best time to test blood sugar?
– Why does some bacon have sugar, and should I be eating it? What about nitrates?
– How do you account for the variations in home glucose meter readings?
– Why are most artificial sweeteners not a good idea?
– Can keto help Reynaud’s Syndrome?
– Is there a role for energy balance on keto specifically after hormones have been normalized?
– Why do some people get keto rash?
– Is my raised blood sugar levels telling me that I am still healing?
– Stalled weight loss after gastric band
– Why do you sometimes go out of ketosis after exercise?
– What is the difference in using MCT oil vs coconut oil?
– What is the proper timing of supplementing with bone broth and other electrolytes?
– Are food sensitivity tests a good idea?
– If calories don’t matter, why do things like the rice diet work?
– Why do I wake up hungry in the middle of the night?

I am a Family Practice Physician. I spent eleven years of my life training to become a physician certified in Family Medicine. But, I found this wasn’t enough. I struggled to treat the “diseases of civilization” that arise from society, our Western diet and lifestyle.
I, also, specialize in dietary weight/obesity management and low-carbohydrate/ketogenic diets. I actually spent an additional three years obtaining specialized training and board certification in this field. When you add all the training and my years of experience in practice together, I’ve spent over 25 years perfecting this art of medicine.
Because of this training, I have been very blessed that people from all over the world travel to Surprise, Arizona, to see me for weight management, dietary advise, and counseling on the diseases of civilization. I’ve been amazed that simple changes in diet halt and reverse obesity, arthritis, diabetes, cholesterol, high blood pressure, etc. The list goes on and on …
But I find a disturbing mindset pervasive through the community and the nation:

After listening to an number of people get angry over this issue in the last few weeks, I began wondering to myself…
“Who ties your shoelaces for you?”

While at a medical conference in Tampa, Florida, I started thinking about uric acid. This lead to remembering the story of a patient who was passing a kidney stone . . . watch to find out what she said.
Kidney stones are really just gout’s wicked step-child and both are usually found in the insulin resistant patient. Learn why as we spend a short 10 minutes talking about how both types of kidney stones are formed and why. Uric acid stones & calcium oxalate stones are siblings with different mechanisms of formation but, oh, how they love hanging out in your kidney.
Interested in learning how to start a ketogenic diet? Sign up for my Free Six-Part Weight Loss Mini-Course and check out DynamicKetones.com if your interested in jump-starting your ketogenic metabolism.

Look at what you can do when you understand how to follow a ketogenic/low-carbohydrate diet. Learn more by clicking above and taking my free weight loss mini-course.
How does being in ketosis and living a ketogenic lifestyle lower your blood pressure, decrease risk of kidney stones and gout? Listen in to the way nitrous oxide is raised by being in ketosis . . . Enjoy!
What is the Yin & Yang of glucose control? It is Glucagon & Amylin. We talked about glucagon in an earlier post. Today we’ll balance the world of blood sugar with Amylin talk. Don’t go getting hypoglycemic with all the excitement . . . !!
Another incretin that you may not know plays a role in your weight loss . . . cholecystikinin (CCK). Enjoy!
Stay tuned for Part II – Gut hormones & GLP-1.



You’re not going to want to miss this one, listen in by down loading KetoTalk on your IOS device or here at iTunes. Or, you can use your computer to listen on KetoTalk.com to hear Dr. Nally & Jimmy Moore talk about the benefits of Ketones, Abdominal Pain and Ketones, & “To Cheat . . . or Not To Cheat.”


Listen to KetoTalk Podcast #32 where we talk about hereditary angio-edema, adequate ketone ranges, statin use while in ketosis and healthy keto questions. You can listen in by going to KetoTalk.com or you can listen in on iTunes.


Too much protein, too little protein? How do you know how much protein to eat? This has become a very confusion question for many of my patients in recent years. There a a large amount of “mis-information” in the ketogenic world about the effect of protein of gaining and losing fat.

For the person exercising 5-6 days a week, 1 gram of protein per pound of ideal body weight is the formula that works quite well. However, for the average Joe or Mary who doesn’t work out for an hour a day 5 days a week, I’ve provided the calculation below. This calculation is a baseline starting point. It is the basic amount of needed protein to maintain muscle on a ketogenic or carnivorous diet:


LISTEN ON YOUR COMPUTER AT KETOTALK.COM
If you are interested in the low-carb, moderate protein, high-fat, ketogenic diet, then this is the podcast for you. We zero in exclusively on all the questions people have about how being in a state of nutritional ketosis and the effects it has on your health. There are a lot of myths about keto floating around the blogosphere, and our two amazing co-hosts are shooting them down one at a time. Keto Talk is co-hosted by 10-year veteran health podcaster and international bestselling author Jimmy Moore from “Livin’ La Vida Low-Carb” and Arizona osteopath and certified obesity medicine physician Dr. Adam Nally from “Doc Muscles” who thoroughly share from their wealth of experience on the ketogenic lifestyle each and every Thursday.

Listen in today as Jimmy and Adam blaze through a bunch of listener questions in Episode 27 of KetoTalk with Jimmy and the Doc!
KEY QUOTE: “Children are born in ketosis, so ketones are perfect for babies. The level of fat in breast-milk is essential for them to maintain their health and their growth.” — Dr. Adam Nally
Here’s are the 12 questions Jimmy and Adam answered in this special Keto Talk Mailbox Blitz extended podcast today:
– Testimonial from someone who learned his lesson why it’s important to stay ketogenic all the time
– Three-decade study confirms saturated fats are bad for health
– Is increased testosterone from a ketogenic diet a bad thing for women?
– Why am I still struggling with low energy and low ketones after months of being in ketosis?
– Can being in nutritional ketosis above 1.0 mmol cause painful headaches?
– Do artificial sweeteners and stevia raise insulin?
– Is my ketogenic diet causing me to cramp up before and during my half marathon racing?
– Is MCT oil a better fat to use on a ketogenic diet than other fats like coconut oil, cream, or butter?
– Why do I have a constant stomachache while I’m on a ketogenic diet?
– Do you have to be in ketosis to burn fat?
– Does being in ketosis lead to daily spotting and extended periods?
– Are ketones in my baby’s breastmilk safe for her to consume? And why did my milk supply drop when I went keto?
– What is the impact of the supplement creatine on ketones, blood sugar, and insulin levels?
– Can I ease into ketosis as a way to avoid the dreaded “keto flu?”
KEY QUOTE: “If you’re not feeling energy after that adaptation period of 2-4 weeks at the very most, then you’re doing something wrong. Let that be your wakeup call to change something.” — Jimmy Moore

Listen in here at KetoTalk.com or you can download the episode for free on iTunes.
Hypertension (elevated blood pressure) is one of the triad symptoms of metabolic syndrome. Most of the hypertension that I see clinically is driven by insulin resistance as  the underlying cause. I see this problem in a very large majority of the people in my office and I am seeing people younger and younger show up with continually increasing blood pressure.
the underlying cause. I see this problem in a very large majority of the people in my office and I am seeing people younger and younger show up with continually increasing blood pressure.
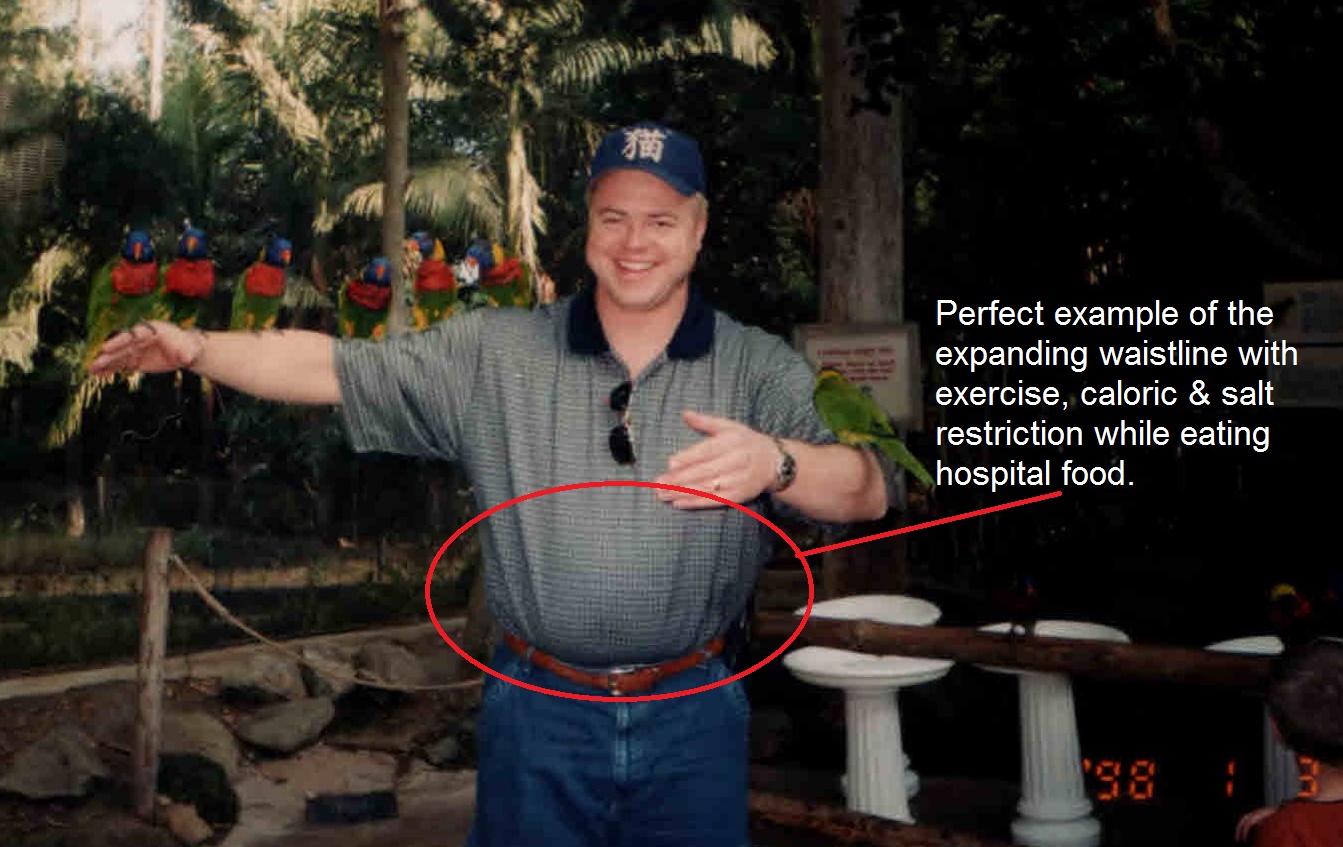
In medical school, we were taught to treat “borderline” or “slightly elevated blood pressure,” through “lifestyle changes” which was another way of saying exercise, caloric restriction & hold the salt. But most physicians today will tell you that exercise, salt & caloric restriction doesn’t work. When asked why the 34 year old male in my office suddenly has elevated blood pressure, the only explanation we had was it is a “genetic problem,” or “blood pressure naturally goes up as we get older,” or “you’ve been eating too much salt,” and they are started on blood pressure medication and sent on their way. But, as time went on, I found that I had to keep adding more and more blood pressure medication to control the continually rising blood pressure of the patients in my practice.
Most of these people will have a progressive elevation in blood pressure over time, and these blood pressure (anti-hypertensive) medications are/were continually raised until the person is on four or five different blood pressure pills at maximal doses. Again, when questioned why, their genetics are blamed and that is the end of it. Or is it?!
What shocked me was that when I took patients off of salt & caloric restriction, and placed them on low carbohydrate high fat diets (and yes, I gave them back their salt), their blood pressure normalized. I noticed that as their fasting insulin levels began to fall, their blood pressure began to return to normal.
What?! Blood pressure rise is caused by insulin?!
Ummm . . . Yes!
I am a prime example. During the first few years of my medical practice and reserve military service, we had routine vitals checkups. I was working out 3-5 days a week with weights and running 3-5 miles 2-3 times a week and restricting my calories to 1500 per day. So, I thought I was in pretty good shape. However, it was not uncommon for for the nurse to raise her eyebrows at my blood pressure readings in the 140-160 systolic and 85-98 range diastolic. “Oh, it’s the lack of sleep last night,” or “it’s the caffeine I had this morning,” would be my excuse. But I was making a lot of excuses, and in light of those excuses, my caloric restriction, exercise and salt restriction, I was also still gaining weight.
By the 5th year of my medical practice, I weighed 60 lbs heavier than I do today and I struggled to keep my blood pressure under 150/95. I was violating my own counsel . . . don’t trust a fat doctor for nutritional advise. (Or, was that advise from Dr.House?)

After cutting out the carbohydrates (I’ve kept my carbohydrate intake < 20 grams per day), moderating my protein intake and eating all the fat I am hungry for each day, my recent physical examination at the beginning of June 2016 revealed my blood pressure at 112/64. I don’t remember ever having blood pressure that low. And to be honest, I didn’t sleep well the night before my exam due to a number of middle of the night patient calls.
When I first started treating the insulin resistance problem in the human, rather than the blood pressure problem, I began to see immediate reductions in blood pressure within one to two weeks. So much of a reduction that if I didn’t warn the patient that they should  begin to back down their blood pressure medications, they would experience symptoms of dizziness, light-headedness, headache and a few patient’s nearly passing out. On a low-carbohydrate, high-fat (ketogenic) diet you need salt (sodium, potassium, & magnesium).
begin to back down their blood pressure medications, they would experience symptoms of dizziness, light-headedness, headache and a few patient’s nearly passing out. On a low-carbohydrate, high-fat (ketogenic) diet you need salt (sodium, potassium, & magnesium).
The process of burning fat as fuel causes you to lose increased amounts of sodium & potassium, and you have to replace these electrolytes. A number of my patients begin a low-carbohydrate, high-fat diet and are afraid of increasing their salt intake. Not replacing these electrolytes while on a ketogenic diet can also lead to low blood pressure, dehydrate and dizziness.
I often wondered why applying a ketogenic diet had such a profound effect on blood pressure so quickly. Dr. Robert Lustig helped answer that question for me.
In order to understand how the Standard American Diet (we call it the SAD diet in my office) raises your blood pressure, it is important to understand how the body processes the basic sugar molecule. Sugar is one glucose molecule bound to a fructose molecule. This is broken down in the body and 20% of the glucose is metabolized in the liver, the other 80% is sent on to be used as fuel throughout the body. Fructose, however, is where the problems arise. 100% of the fructose is metabolized in the liver, and the by product of fructose metabolism is increasing the liver’s production of MORE glucose and the byproduct of uric acid. Uric acid is produced and this inhibits the production of nitric oxide. The diminished nitric oxide in the presence of an increased level of glucose (stimulating increased insulin production due to eating starches) constricts the blood vessels and raises blood pressure. Yes, that donut you just ate raised your blood pressure for the next 12 hours.
The mechanism that fructose containing carbohydrates, sugars and starches raise blood pressure, cholesterol and cause weight gain can be seen in the really complex diagram found in Dr. Lustig’s 2010 article:

So, how do you lower your blood pressure through diet?
First, cut out all the simple sugars. These include anything with table sugar, high fructose corn syrup and corn syrup. (This is why people with any change in diet see some improvement in weight and blood pressure as they remove the simple sugars like candy, sugared drinks and pastries from their diet.)
Second, limit your overall intake of other sources of carbohydrates including any type of bread, rice, pasta, tortilla, potato, corn and carrots. Realize that carbohydrate in fruit is fructose, and when taken with other forms of glucose can have the same effect as table sugar – it can and will raise your blood pressure, as well as halt or cause weight gain.
Third, if you are taking blood pressure medications for hypertension, see your doctor about close monitoring of your blood pressure as it can and will drop within 2-4 weeks of making these dietary changes.
Maintaining ketosis is really important for weight loss and blood pressure or hypertension control. I am very much an advocate of using real food for this process, but I have also found that the use of exogenous ketone salts aid significantly in maintaining ketosis. I have found that exogenous ketones are the next step in bridging the difficulty of day to day maintenance of ketosis.
It isn’t making the mistakes that’s critical; it’s correcting them and getting on with the task that’s important. If you’ve been calorie restricting and exercising to lower you blood pressure, don’t fret. A simple change in your diet focused on restricting starches and carbohydrates has been demonstrated in my office to be more powerful than many of the blood pressure medications we’ve used for years.
Learn how to get started on a low carbohydrate, high fat (ketogenic) diet here. You can also read about the basic principles in my recent articles The Principle Based Ketogenic Lifestyle – Part I and Ketogenic Principles – Part II.
Over the last few months, I’ve found myself amid the center of vehement nutritional arguments about fat, carbohydrates, calories and diet. I have found it fascinating that very intelligent men and women, over the last 50 years, have accepted, without reservation, a dogma taught them by their eighth grade nutrition teachers. This dogma is interlaced and interwoven throughout the textbooks, manuals, and college cafeterias throughout the world.
Very few souls have questioned this dogma, and even in light of it’s utter failure to improve one’s health, it becomes the fall back point upon which millions have accepted nutritional disease and defeat. It makes no sense that a dogma of this nature, without anything more than a scientific corellation in the 1960’s, could sway the minds of intelligent researchers, physicians and scholars for over 50 years.
It is a well known fact, however, that hydrogen is the most common element in the universe and is used as a basic building block for most molecular structures. What many don’t realize is there exists another element yet to be added to the periodic table that is almost as prevalent called moronium (pending symbol approval – Mu). It fills the blank space on the table of elements between Hydrogen and Helium. I, and those who have been able to identify this element, suspect that moronium is a gas at room temperature and has some affinity to binding the white matter of the brain responsible for catechol-O-methyltransferase (COMT) gene regulation of the prefrontal cortex. It is suspected by some that when it is inhaled by a person of low intellect, it has only a mild effect. However, when combined with either oxygen (O), hydrogen (H) or Helium (He) and inhaled by those of higher intelligence, it has a much wider, more potent and even stupefying diffusion effect, that is quite surprising to witness.
Moronium reacts adversely when diffused into blood with a higher alcohol concentration and seems to spontaneously combust when it is exposed to old paper and libraries. Moronium is very difficult and very expensive to isolate. Moronium seems to be more prevalent during the summer and winter solstices, which may be why moronium intoxication seems to appear around holidays. Recent attempts in a nearby lab to synthetically create even small crystals of moronium cause an explosion, physically and psychologically stupefying all of the researchers involved and inducing them to leave the study of science and pursue individual careers as drummers.
The presence of moronium seems to be higher in those that do not read, or have an aversion to reading. There is some correlation that moronium drops in proportion to listening to iTunes podcasts, however, follow-up reading does appear to have a potential lowering affect on the moronium levels within the brain.
Why do I bring this up?
I suspect that this little known element may be responsible for intelligent men and women introducing questionable theoretical science as incontrovertible truth. Those with suppressed COMT regulation seem to have a propensity to accept theoretical science because it sounds good, even when there’s really no way to actually prove the theory at the time, or when colleagues have accepted the theory in a peer-pressure instead of peer-review situation.
The stupefying effect of moronium bound COMT produces dogma like:
The amazing thing about science is that it is self-correcting (at least it used to be). A scientist makes a set of observations about nature, and then identifies a plausible theory within the laws of nature to fit those observations. Then, researchers take that theory and test it in as many ways as possible, attempting to disprove the theory and isolate the cause of the observation. If the theory withstands scrutiny it becomes widely accepted.
At any given point in the future, if contradicting evidence emerges, the original theory is discarded and a new theory is then identified. In essence, this is the simple scientific method, however, in modern day application, it has become a great deal more messy than you’d think.
This approach (application of “the scientific method”) was skirted during the 1960’s and 1970’s regarding the “fat causes heart disease” theoretical proposition. Interestingly, there was also a notable increase in the number drummers and musicians during the 1980’s Hair Bands era. This begs the questions, which I wholly agree needs further study: Does moronium exist? and . . . . Did levels of moronium actually increase between 1960 and 1990 causing a surge in the presence and popularity of Hair Bands?

It only took us 20 years to get past the Era of the HairBands, hopefully we can turn the nutritional ship around and recognize the real culprit causing the Diseases of Civilization.


(Author’s Note: For those who may possibly be under the influence of moronium toxicity, the post above is written in sarcastic jest, and to be clear, there IS NOT an element currently under investigation called moronium!)
Listen in to KetoTalk.com for Podcast #26.
The health podcast legend, Jimmy Moore, and I talk about how much fat is too much. Or, is it? What’s the deal with Zero-carb ketogenic diets? We answer your questions and try to give you the most up-to-date knowlege regarding the ketogenic lifestyle and how it affects your metabolism. We zero in exclusively on all the questions people have about how being in a state of nutritional ketosis and the effects it has on your health.
There are a lot of myths about “keto” floating around out there and we shoot them down one at a time.
You can down-load it for free on iTunes or listen to KetoTalk.com on your computer.
Enjoy!!


I’m sitting here at my home-office desk, on this beautifully hot 118° Arizona afternoon, eating this luscious piece of ketogenic Key-Lime & Blue-Berry Cheese Cake that my wife made for Father’s Day . . . pondering all the reasons ketosis has been a blessing in my life, specifically as a father. As I sit, reason after reason popped into my mind.

“Hmmm, I should share these . . . Why aren’t you sharing them?” I mused. So, with the the sweet tart of blue-berry on my palate and with a wipe of whipped cream from the corner of my lip, my fingers begin to click away on the keyboard.
What makes a person a father?
Testosterone –
Well, first, . . . Testosterone. I know. Leave it to a man to start with testosterone, but in the big picture, a man really isn’t a man if he doesn’t have a little extra testosterone, right? I mean, it was during the 5th week of embryonic development that my Y chromosome began signaling the differentiation of male fetal growth in-utero. And like every male, that same hormone testosterone continues to differentiate me from the human female counterpart throughout life.
Low testosterone has become a significant issue. 20-30% of the men in my practice suffer from some degree of suppression in testosterone when they first present in my office. In fact, you can’t watch late night TV any longer without being asked the question about low testosterone (Low ‘T’).
We know that the primary nutrient shown to affect testosterone to the greatest extent is fat. Studies reveal that diets low in fat are associated with lower testosterone compared to diets high in fat (1, 2). That begs the question, has 50 years of low fat diets made us less manly?

When did this become acceptable? And, does our diet of low fat have anything to do with it? I actually think it plays a role.

Testosterone is essential in providing energy, muscle mass & growth and actually keeping the waistline down. Adequate testosterone is one of the key components allowing the man to fill the father’s rolls of protector and provider, and if your diet doesn’t help stimulate its production, your less inclined to perform well in areas requiring its presence. That means that the bacon and eggs you crave in the morning lends toward your manliness, and the bagel and orange juice may be a little feminizing.
Fathers Need Muscles –
Second, father’s need muscles for all sorts of important things. It’s often Dad who carries the child on his shoulders, or lifts you above his head. It takes muscles for that.

We talked about the importance of testosterone in muscle development. That that’s not all. Many fathers can provide for their families specifically because of their ability to use that muscle. That’s not saying women can’t use muscle, too. I’m saying that a number of jobs that make our country function that require fitness, strength and muscle, like police, firefighters, construction, life-guards & delivery drivers. These jobs require muscle.

We now know that ketones, the primary fuel in a ketogenic diet, restrain muscle breakdown by decreasing leucine oxidation and preserving muscle mass (3). So, yes, visiting the donut shop actually does make you less manly by allowing the more rapid degradation of your muscles.
“Wasn’t it my muscles that first got your attention when we met and got this whole father thing started in the first place, honey?” I asked my wife in the kitchen.
“What?! No . . .” she responded.
“Oh, . . . never mind.”
Energy –
Whether you have great muscles or not, you need energy for the muscles you have to fill your role as a father. Work requires energy. As fat is increasingly used as fuel instead of sugar, the liver breaks it down and produces ketone bodies, or ketones. The liver itself, doesn’t use the ketones, so they are taken up by the muscles and brain for fuel. Increased energy, mental clarity and suppression of inflammation are the key findings that are noticed while using fat as your primary fuel. What father couldn’t us a little more of that?

In fact, several studies report that fathers have the biggest impact on the overall fitness and on the overall weight of their children. It was found that the father’s, not the mother’s, total and percentage body fat was the best predictor of whether or not the couple’s daughters gained weight as they got older (4). All the more reason to keep your waistline under control, Dad.
Another fascinating study showed fathers’ (again, not the mothers’) body mass index is directly related to a child’s activity level (5).
Energy and muscle is essential for “rough housing” and there is science to prove that “rough housing” makes your kids awesome! Psychologist Anthony Pellegrini, in the book The Art of Roughhousing, has found that the amount of roughhousing children engage in predicts their achievement in first grade better than their kindergarten test scores do. What is it about rough and tumble play that makes kids smarter? Well, a couple things.

Roughhousing makes your kids more resilient and resilience is a key in developing children’s intelligence. Resilient kids tend to see failure more as a challenge to overcome rather than an event that defines them. Intellectual resilience that comes from energetic fathers helps ensure your children bounce back from bad grades and gives them the grit to keep trying until they’ve mastered a topic.
Intelligence for You and Your Family –
Neuroscientists studying animal and human brains have found that bouts of rough-and-tumble play increase the brain’s level of a chemical called brain-derived neurotrophic factor (BDNF). BDNF helps increase neuron growth in the parts of the brain responsible for memory, logic, social intelligence and higher learning–skills necessary for academic success. We,also, now know that the brain that uses fat, or ketones, as it’s primary fuel recovers from injury and makes BDNF more effectively (6,7).
That rib-eye with steak butter your kids gave you for dinner is actually making you and them smarter and more resilient.
Overall Happiness –
The Harvard Grant Study completed in 1934, the longest longitudinal study ever done on the lives of men, found that a man’s father influenced his life in multiple ways exclusive to his relationship with his mother. Loving fathers imparted to their sons:
It should be noted that “it was not the men with poor mothering but the ones with poor fathering who were significantly more likely to have poor marriages over their lifetimes.” Men who lacked a positive relationship with their fathers were also “much more likely to call themselves pessimists and to report having trouble letting others get close” (8).
You, as a father, matter. And, being in ketosis makes you an even better father! Seriously.

When all is said and done, a man’s relationship with his father very significantly predicted his overall life satisfaction at age 75 — “a variable not even suggestively associated with the maternal relationship” (8).
So, back to my key-lime blue-berry cheese cake, my wife just made me a better husband and father. Thanks, Dear!!
References:
Figueroa-Colon R, Arani RB, Goran MI, Weinsier RL. Paternal body fat is a longitudinal predictor of changes in body fat in premenarcheal girls. Am J Clin Nutr. 2000 Mar;71(3):829-34.
Finn, Kevin et al. Factors associated with physical activity in preschool children. J of Ped., Vol 140, Issue 1, 81-85
Vizuete AF1, de Souza DF, Guerra MC, Batassini C, Dutra MF, Bernardi C, Costa AP, Gonçalves CA. Brain changes in BDNF and S100B induced by ketogenic diets in Wistar rats. Life Sci. 2013 May 20;92(17-19):923-8.


Listen to Dr. Nally & Jimmy Moore as they answer the following questions in KetoTalk Podcast #21.
Get the answers to these questions and much more when you listen to KetoTalk.com or download the podcast for free on iTunes.

Dr. Nally recently spoke about Low-Carbohydrate/Ketogenic Diets on the 2016 Low Carb Cruise to the Eastern Caribbean. While there, he and Jimmy Moore recorded another episode of KetoTalk with Jimmy and the Doc.
Listen in to KetoTalk Episode 20: A LIVE Q&A Session From The 2016 Low-Carb Cruise
Here’s what Jimmy and Dr. Nally talked about in Episode 20:
– We are in front of a LIVE audience of Ketonians
– How long will you experience hair loss when you go ketogenic?
– What role does resistant starch have on the keto diet?
– Is eating high-fat with high-carb harming my boyfriend?
– How does intermittent fasting help with keto?
– Whether to count total vs. net carbohydrates
– Whether you need to cycle carbs when building muscle
– What the best way to test your ketones is
– How to test blood ketones on a budget
– What the difference is between an NMR and basic lipid panel
– The dramatic changes in your cholesterol when going keto
– How long should you be on keto before running blood tests?
– Whether you should cut fat lower on keto to speed up weight loss
– Is having a lower body temperature a bad thing when eating keto?
You can listen at the iTunes page here, or download it for free to your favorite iTunes player.

Alzheimer’s Disease is a progressively devastating, fatal disease that affects 5.2 million Americans and over 44 million people throughout the world. This disease is often more difficult on the families and caregivers, then on the patient’s themselves. With my office located near three of the country’s largest retirement communities, it is a disease that I see and treat every single day.
A paper published in the Journal of Alzheimer’s Disease this week, confirmed suspicions and patterns that I have been seeing for over 15 years. A significant number of my patients with Alzheimer’s dementia (AD) also have insulin resistance, impaired fasting glucose or diabetes mellitus – type II. I have long wondered if there was a tie to these diseases because of the patterns seen in my office. However, much of the research examining the association between type II diabetes and AD have come to differing conclusions about the cause. Some have concluded that insulin resistance is to blame and others have concluded that insulin deficiency may play a role. Other studies have found that a hormone called amylin secreted with insulin is to blame. And, other articles have found that both amylin and amyloid-beta protein form the plaques within the brain common to AD. Lastly, more recent data complied appears to point to the opposite conclusion – that amylin provides neruro-protective effects and may actually reduce the symptoms of AD. So, what are we to make of all of this? How is the doctor in the trenches to interpret and then advise those with or at risk for Alzheimer’s Disease?
The paper referenced above, by Dr. Schilling, takes all of this data into account and with careful attention to research methods and compiling immense amounts of data from all of these studies, it identifies the integration points with insulin and insulin-degrading enzyme (IDE) that have begun to disentangle the research. What it reveals is fascinating information.
First, under normal circumstances, we now know that insulin stimulates the expression of IDE, which subsequently breaks insulin down after it is used. IDE, however, also plays a roll in breaking down amyloid-beta protein and other amyloidogenic peptides. Alzheimer’s disease is caused by a build up of these amyloid based proteins forming plaques within the human brain.
Second, the body’s system for breaking down and removing these plaques can fail or become inefficient in four different ways. What has been confusion for many years to researchers is now much more clear with our clarified understanding of insulin resistance moving through five different stages (see my article on Diabetes Mellitus type II – really the fourth stage of insulin resistance).
What are these four possible points of breakdown?
Further study is essential to tease out what the nuts and bolts of the mechanism may be, but with our understanding of stages of insulin resistance, the puzzle pieces are falling into place. This conglomeration of data provides further confirmation that insulin resistance is likely the key player in the progression of Alzheimer’s Disease years before type II diabetes or type I insulin dependence are ever diagnosed in the individual.
What is the take home message today? Impaired fasting glucose, diabetes mellitus and Alzheimer’s disease are later expressions of the underlying problem: insulin resistance. This is where a low carbohydrate and/or ketogenic diet begins to play a huge role in both prevention and treatment of Alzheimer’s Disease.
More to come . . . In the mean time, pass the butter and the Keto//OS.
A patient recently asked me how bad being in nutritional ketosis was for her. I responded that the worse problem I’ve seen recently is the patient that broke his toe when he slipped on bacon grease. Are there risks with a ketogenic diet? Yes, but these usually only occur when you cheat or fall off the wagon. What problems can arise? Lets talk about them individually.
First, as I stated above, make sure you don’t slip on bacon the grease. It really can be an issue if you’re not used to using increased amounts of fat in your kitchen. So, be prepared for how to cook and use fat. Grandma understood this well, we could learn a great deal from her if you ask her about using bacon grease.
Second, let’s define the difference between ketosis and keto-acidosis and try to clarify the misinformation that is being spread around the blogosphere.
A ketone is a molecule the body produces from the breakdown of fat (specifically triglycerides) and some proteins (amino acids). There are specifically three types of ketones: beta-hydroxybutyric acid, acetoacetic acid and acetone. If ketosis was “bad,” then why would our bodies produce these molecules? They are not bad, and in fact, multiple studies show that the body is often more efficient in weight loss, inflammatory reduction, bowel function, epigenetic influence and maintenance of lean body mass more effectivly when it functions on ketones rather than glucose as its primary fuel source. You can see these studies here, here, here and here.
The body can only supply a limited amount of sugar or glucose for fuel. If you talk to runners, marathoners or triathletes, they will tell you that after about 45-90 minutes of continuous endurance exercise the glucose supply runs out and they will experience what is termed a “bonk” (have a low-blood sugar or hypoglycemic episode). Unfortunately, our bodies can only store about 18-24 hours of glucose.
However, the body can store days upon days of fat in the form of triglyceride in the fat cells. Triglyceride is broken down into ketones. If glucose is the “unleaded” fuel, you can think of ketones as the “diesel fuel” that is easier to store and runs longer.
The average body functioning on ketones as the primary fuel will have a ketone level measured in the blood somewhere between 0.4 and 4 mmol/L. Because of a balance that is created by the use of ketones and a feedback mechanism that kicks in when the ketone level rises, the body will maintain a pH of around 7.4.
Ketoacidosis is dramatically different. If you are a type I diabetic, you don’t produce any insulin. The feedback mechanism regulating ketone use is broken and the ketone levels and triglyceride breakdown speeds up because the body can’t access glucose and can’t produce insulin. The ketone levels spike and the level can rise to > 25 mmol/L. In the presence of a high blood sugar and high ketone level, the acid level in the blood shifts to a pH of less than 7.3. This is referred to as metabolic acidosis and can be life threatening as the low pH shuts down the bodies’ enzymatic processes and a person becomes critically ill and without treatment, can die. Further information on ketoacidosis can be found here.
If you’re not a type I diabetic, you have nothing to worry about. Regardless of what the “ketogenic nay-sayers” blog about, your liver makes approximately 240g of glucose per day, 24 hours a day, 7 days per week, this stimulates a basal release of insulin which keeps the pH in check. It’s also what keeps weight loss at a consistent pace of around 2-10 lbs per month.
If you are a type I diabetic, don’t fret. Carbohydrate restriction can still be used very effectively. It just takes some balancing and understanding of your individual metabolism. It does require close blood sugar and insulin monitoring. If you are a Type I diabetic, please talk to your physician, obesity specialist and/or bariatrician about how to follow a carbohydrate restricted diet while using insulin. It can be done and it can be done very effectively, but monitoring is essential.
What are the other potential problems that can arise when you follow a ketogenic diet?
Gastrointestinal (GI) Disturbances – Yes. Any time you change your diet you may experience diarrhea, constipation or gassiness. Most of the time, this is because you are either 1) not eating enough leafy greens (fiber) or 2) you’re using a supplement that contains an artificial sweetener. Most of the studies on ketogenic diets did not incorporate fiber and the studies used to make this point were on children who used a ketogenic fat supplement shake or liquid preparations containing these artificial sweeteners to make them palatable. If you have spoken to any obesity specialist, they will tell you, the best way to follow a ketogenic diet is to eat real food. If you want to read about the anecdotal GI effects of sweeteners, read the comment section in Amazon about the Haribo Sugar Free Gummy Bears.
Oh, by the way, 65% of patients in my practice following ketogenic diet see improvement in gastroesophageal reflux (GERD) symptoms. This was seen in a 2006 study looking at ketogenic diets and reflux.
Hair Loss/Thinning – Yes. This does happen initially and if you are not eating enough fat. It is important to note that hair loss/thinning can occur with any form of weight loss. You can see data on this here. Hair loss is very common if you are restricting calories, which was occurring in a number of the ketogenic dietary studies previously published. You do not, and should not, need to “restrict calories” if you are following a ketogenic diet correctly, and in fact, most people take in more than 1800 calories on a ketogenic diet.
Inflammation Risk – In every patient that I have placed on a ketogenic diet in the last 10 years, all inflammatory markers including CRP, Sedimentation Rate, Apo B, HOMA-IR and Uric Acid have all decreased. Inflammation gets better on an appropriately formulated ketogenic diet. The older studies of ketogenic diets in children contain most of their fat from Omega-6 fatty acids from vegetable oil which will increase inflammation and oxidative stress, spike the cortisol levels and have the secondary effect of actually raising the triglycerides. You can find more information on this here & here.
Kidney Stones/Gout – These (kidney stones & gout) are both commonly caused by spikes in uric acid. As noted above, I’ve seen multiple cases in my practice where a ketogenic diet lowers uric acid. Only a small clinical trial has been published in the literature (and it wasn’t truely ketogenic), but the results point to the potential for ketogenic diets to lower uric acid. Ketogenic diets also have the capacity to lower the formation of calcium oxalate stones through a secondary mechanism where calcium oxalate formation is driven by uric acid formation. Older small case reports in the pediatric seizure literature identify calcium oxalate stones, however, dehydration (too little fluid/water intake) is the primary cause of kidney stones.
So, are ketogenic dietary patients at risk? Only if you cheat on your carbohydrate restriction and you let yourself get dehydrated. So, I warn patients. Don’t cheat and make sure your drinking adequate amounts of water.
Muscle Cramps/Weakness – The process of weight loss occurs by burning fat into CO2 and water. We breathe the CO2 out, but the water produced has to follow salts out through the kidneys. Hence, we lose water and salts. This can cause weakness and muscle cramps. The solution? Stop restricting salt on a low carbohydrate diet. We are the only mammal that restricts salt and we do it because low-fat diets cause us to retain water. Low carbohydrate diets do the opposite. Use sea salt or sip beef or chicken bouillon broth with your dinner. You may consider adding magnesium to your diet. The use of yellow mustard also helps (the small amount of quinine in yellow mustard stops the cramping). If you have congestive heart failure, talk to your doctor about monitoring your salt intake in balance with your diuretic or water pill.
Hypoglycemia – If you read the ketogenic diet research, most of it was done on epileptic children. The diets called for a period of starvation, and then the introduction of a ketogenic liquid based shake following the John’s Hopkin’s protocol. It is a well-known fact in medicine that starvation in children can frequently cause hypoglycemia, especially in children with other genetic or congenital defects leading to forms of epilepsy. In clinical practice, with ketogenic diet use in adults, hypoglycemia is rare. The only time I see hypoglycemia is when patient’s with significant insulin resistance or diabetes cheat on a large amount of carbohydrate and get a secondary insulin surge leading to hypoglycemia 3-5 hours after cheating.

Low Platelet Count (Thrombocytopenia) – Again, this was seen in epileptic children who were placed into starvation first, then introduced a liquid fat replacement shake to stop intractable seizures. These liquids or shakes were often nutrient deficient in other essentials. Folic acid, B12 and copper deficiency can occur when not eating “real food.” Low platelet counts are rarely seen on ketogenic diets based around “real food.” Many children in the ketogenic studies had been on or were concomitantly on valproic acid for their seizures. Valproic acid is commonly known to cause thrombocytopenia and this is another reason that thrombocytopenia was seen in this population. (Barry-Kravis E et al, Bruising and the ketogenic diet: evidence for diet-induced changes in platelet function. Ann Neurol. 2001 Jan;49(1):98-103.; Kraut E, Easy Bruising, http://www.uptodate.com, May 2015.)
Impaired Concentration/Mood – A number of patients starting carbohydrate restriction will go through 2-4 weeks of carbohydrate withdrawal. This carbohydrate withdrawl can be experienced just as powerfully as morphine withdrawal in some patients. Sugar is a drug and has a powerful effect on the same hedonic receptors that morphine does in the brain. Some patients will experience headache, tremor and decreased concentration while “withdrawing” off of starches and carbohydrates. Studies show that after the 4-8 week period of keto-adaptation, cognitive function dramatically improves.
Metabolic Acidosis – As described above, metabolic acidosis can occur in a type I diabetic who is not getting adequate insulin, and metabolic acidosis has also been shown to occur in young children placed on severe carbohydrate AND protein restriction, as was the case in some of the ketogenic dietary trials with epileptic patients. (Saxena VS, Nadkarni VV. Nonpharmacological treatment of epilepsy. Annals of Indian Academy of Neurology. 2011;14(3):148-152. doi:10.4103/0972-2327.85870.; The Ketogenic Diet: One Decade Later, Pediatrics March 2007; 119:3 535–543).
Osteoporosis/Osteopenia – If your ketogenic diet is “shake” or “meal replacement” based, you run the risk of mineral deficiency that could lead to Osteoporosis, however, if you are using real food, the opposite is true and most patients have improvement in their Vitamin D levels and bone density. (, , , Babette S Zemel, Progressive bone mineral content loss in children with intractable epilepsy treated with the ketogenic dietAm J Clin NutrDecember 2008 88: 1678–1684; doi:10.3945/ajcn.2008.26099)
Easy Bruising – This is usually due to inadequate protein supplementation as was the case in much of the ketogenic literature where protein levels were also restricted. (Kraut E, Easy Bruising, http://www.uptodate.com, May 2015.)
Infections/Sepsis/Pneumonia – Increased susceptibility to illness has never been an issue in the 10 years I have been using ketogenic diets with my patients. These issues were seen in the John’s Hopkins protocol with children who had not only epilepsy, but other congenital disorders predisposing them to infection, who were placed on a diet low in protein and carbohydrate. (Saxena VS, Nadkarni VV. Nonpharmacological treatment of epilepsy. Annals of Indian Academy of Neurology. 2011;14(3):148-152. doi:10.4103/0972-2327.85870.)
Pancreatitis – Patients who are insulin resistant or have impaired fasting glucose commonly have high triglycerides. Elevation in triglycerides itself is a cause of pancreatitis. Ketogenic diets lower the triglycerides. However, if a patient has not been following their diet as directed, spikes in the triglycerides can occur placing the person at risk for pancreatitis.
Long QT Intervals/Heart Arrhythmias – The list of things causing Long QT intervals and abnormal heart rhythms is long and variable (Acquired Long QT Syndrome. Berul C et al. www.uptodate.com, May 2015). It is well know that starvation, rapid weight loss and liquid protein diets can cause a delay in the conduction signal in the heart. Anyone wishing to start any diet should have an electrocardiogram (EKG) through their doctor to ensure that the diet (of any type) doesn’t exacerbate a prolonged QT interval.
Cardiomyopathy – Prolonged QT intervals have been associated with cardiomyopathy and the former can stimulate the later. Any diet that has the potential to prolong a QT interval has the potential to cause cardiomyopathy. Hence the need for regular EKG monitoring on any diet (Acquired Long QT Syndrome. Berul C et al. www.uptodate.com, May 2015).
Lipid/Cholesterol Changes – In the 10 years I have been prescribing ketogenic diets to patients, I have seen dramatic improvement in the triglycerides, small dense LDL particle and HDL levels. The only time triglycerides rise over 100 is if the patient is using artificial sweeteners, is cheating on the carbohydrate restriction, or is taking in too much protein. Total cholesterol commonly rises, however, this is indicative of the fact that there is a shift in the LDL particle size and this affects the calculation of both total cholesterol and LDL-C. In light of this, most of my patients have dramatic improvement in triglycerides and small dense LDL particle number.
Myocardial Infarction – In older papers, elevated total cholesterol was noted and the authors made the “assumption” that myocardial infarction “could” be a risk. We now recognize that elevated Total Cholesterol is NOT a causitive risk for heart disease.
These previous assumptions have been interpreted by the blogosphere ketogenic “nay-sayers” as actual risk. However, a correlation and causation was never made. Again, in the 10 years I have been using and prescribing ketogenic diets, I have seen dramatic improvement in cholesterol profiles, inflammatory markers, atherosclerosis and carotid intimal studies (Shai I et al, Circulation 2010; 121:1200-1208).
Menstrual Irregularities / Amenorrhea – It is well known that any diet causing protein or other nutritional deficiency will affect the menstrual cycle first and growth in stature second. The only time menstrual irregularities occur with a ketogenic or Low-Carb diet is when a patient is not taking in enough protein and/or fat, and is not eating real food. What amazes me is that a properly applied ketogenic diet actually causes normalization of the menstrual cycle, and in my practice, I’ve had a number of women successfully be able to conceive after making a ketogenic dietary change.
Death – All cases of death related to ketogenic diets have been documented in children while using liquid based carbohydrate and protein restricted formulas for ketosis to treat epilepsy. These cases revealed the formation of a prolonged QT interval leading to cardiomyopathy due to deficiency in selenium. This was later solved by the addition of selenium to the ketogenic supplement. (Stewart WA et al., Acute pancreatitis causing death in a child on the ketogenic diet, J Child Neurol. 2001 Sep;16(9):682.; Bergqvist AG et al, Selenium deficiency associated with cardiomyopathy: A complication of the ketogenic diet. Epilepsia. 2003 Apr;44(4):618-20.; Kang HC et al., Early and lat onset complications of the ketogenic diet for intractable epilepsy, Epilepsia. 2004 Sep;45(9):1116-23.; Kang HC et al, Efficacy and Safety of the Ketogenic diet for intractable childhood epilepsy: Korean Multicentric Experience, Epilepsia. 2005 Feb;46(2):272-9.) Selenium deficiency does not happen when the diet is based on the use of real food instead of supplementation, and has never been seen in adults.
Is a ketogenic diet bad for you? You be the judge.
If you are following a ketogenic diet correctly and with real food, the only thing you really need to worry about is slipping on bacon grease.

In an era where over 70% of us (35.7% obesity & 34% overweight in 2015 according to the CDC) have started to resemble the food pyramid, seeing the effect of a carbohydrate heavy diet should give a clue.

Our bodies were meant to burn ketones. We have a parallel system within us designed to use ketones as an energy source. Ketones are faster and more efficient than the way our bodies use glucose. Ketones give you 38% more energy than you can get from glucose. We as a society are following a deceptive food pyramid.
When we limit or remove carbohydrate from our diet, we are left with ketones as a primary fuel. It is time that we recognize what Dr. Yudkin was trying to tell us in 1970’s, that our carbohydrate and sugar intake is the driver for heart disease, diabetes and the diseases of civilization. (Yudkin, John. Sweet and dangerous: the new facts about the sugar you eat as a cause of heart disease, diabetes, and other killers. PH Wyden, 1972.)

 If you are interested in the low-carb, moderate protein, high-fat, ketogenic diet, then this is the podcast for you. We zero in exclusively on all the questions people have about how being in a state of nutritional ketosis and the effects it has on your health. There are a lot of myths about keto floating around out there and our two amazing cohosts are shooting them down one at a time. Keto Talk is cohosted by 10-year veteran health podcaster and international bestselling author Jimmy Moore from “Livin’ La Vida Low-Carb” and Arizona physican and certified bariatric physician Dr. Adam Nally from “Doc Muscles” who thoroughly share from their wealth of experience on the ketogenic lifestyle each and every Thursday. We love hearing from our fabulous Ketonian listeners with new questions–send an email to Jimmy at livinlowcarbman@charter.net. And if you’re not already subscribed to the podcast on iTunes and listened to the past episodes, then you can do that and leave a review HERE. Listen in today as Jimmy and Adam answer more engaging questions about nutritional ketosis from you the listeners today in Episode 17!
If you are interested in the low-carb, moderate protein, high-fat, ketogenic diet, then this is the podcast for you. We zero in exclusively on all the questions people have about how being in a state of nutritional ketosis and the effects it has on your health. There are a lot of myths about keto floating around out there and our two amazing cohosts are shooting them down one at a time. Keto Talk is cohosted by 10-year veteran health podcaster and international bestselling author Jimmy Moore from “Livin’ La Vida Low-Carb” and Arizona physican and certified bariatric physician Dr. Adam Nally from “Doc Muscles” who thoroughly share from their wealth of experience on the ketogenic lifestyle each and every Thursday. We love hearing from our fabulous Ketonian listeners with new questions–send an email to Jimmy at livinlowcarbman@charter.net. And if you’re not already subscribed to the podcast on iTunes and listened to the past episodes, then you can do that and leave a review HERE. Listen in today as Jimmy and Adam answer more engaging questions about nutritional ketosis from you the listeners today in Episode 17!
