
You don’t want to miss this event . . . Space is limited so RSVP TODAY!!

You don’t want to miss this event . . . Space is limited so RSVP TODAY!!

I will be starting a twice weekly exclusive live-stream here for my amazing online followers and patient who are participating in the KetoClan Group on the following sixteen topics next week. Will be sharing the basics and my 22 years of clinical experience with each of these topics as it relates to health and weight management. These topics will take 10-30 minutes, then giving the remainder of the hour to you to ask questions.

The topics we will cover over the next 8 weeks are listed below:
1. Insulin
2. Monitoring Glucose – CGMs
3. Fat Adaptation
4. Things that make insulin go “bump in the night (or the day)” – (sweeteners, creamers, teas, Resveratrol, nuts, etc)
5. Protein
6. Basic Thyroid Function
7. Female Hormones
8. Male Hormones
9. Testing Ketones in Urine, Breath, Blood
10. Ketoacidosis
11. Medications and ketogenic diets (Metformin, DPP4s, GLP-1, SLT-2s, sulfonoureas, Berberine)
12. Stress – Cortisol & DHEA
13. Exercise – Cardiovascular and Resistance Exercise
14. Sleep
15. Food Cravings and the Subconscious Mind
16. Keto, Carnivore or Fasting – What should I be doing?
Not a member yet? Sign up here.

I’ve been told that many of you have nominated me. Thank you!!!
Every year Ketogenic.com hosts the Keto Awards with Metabolic Health Summit to highlight some of the best and brightest in our community.
There are five unique categories in which you can nominate and it would be an honor to me for you to add your vote:
Top Keto Educator
Top Keto Book
Top Keto Podcast
Top Keto Researcher
Making Positivity Louder
I’ll be sure to let you know who is selected.
Please take a minute to cast your vote for me.
Vote Here:

What is the cause of abdominal bloating when following a ketogenic or low-carbohydrate diet?

BHB stands for beta-hydroxybutyrate. This is one of three naturally occurring ketones formed in the body when metabolizing fat.

I’ve been asked what they are and how to use them quite a few times in the last week, so I thought I’d answer it here. . .
BHB can be used for a number of things:
1) to push you into a ketogenic state for 1-6 hours – I use them to jumpstart keto in people just starting a ketogenic diet (however, if BHB is being used while cheating on carbs at the same time, they often halt weight loss and in some cases can allow for weight gain).
2) I use it as a pre-workout drink for increased energy and stronger muscle contraction (I use them prior to sword fighting and it allows me more energy and endurance.)
3) For appetite suppression when the “munchies” try to kick in due to stress or anxiety.
4) To help enhance cognition in patients with Alzheimer’s dementia and Parkinson’s disease.
5) To improve mental clarity and focus in those with ADD/ADHD.
6) I also use them as a meal replacement while traveling.
7) I use them to help people who are morbidly obese experience a ketogenic state when they have never restricted carbohydrates before.
8) And, to prevent seizures when scuba diving with re-breather type equipment (bubble-less SCUBA).
You can find my exogenous ketones (BHB) at http://www.ketoliving.com

Isn’t it interesting, back in April and May, 2020, those of us closely watching the data stated that this virus would look much like the influenza pandemic of 1918. Look closely at the numbers of deaths in St Louis (who participated in the 1918 quarantine – red line) and Arizona, who has done much the same in our approach (in the 2nd graphic below).
 The death count curves are nearly identical. Interestingly, the numbers of those that died St Louis are almost identical to Arizona’s graph below, directly from the Arizona Department of Health Website. We know that the rates of infection differ between the two viruses and a number of things including domicile proximity, health of the city or state, transportation methods, sanitary condition, etc. play a significant role in the infection rates. My point is not to compare the two viruses, but to point out that the effect of quarantine did exactly what we expected it to do.
The death count curves are nearly identical. Interestingly, the numbers of those that died St Louis are almost identical to Arizona’s graph below, directly from the Arizona Department of Health Website. We know that the rates of infection differ between the two viruses and a number of things including domicile proximity, health of the city or state, transportation methods, sanitary condition, etc. play a significant role in the infection rates. My point is not to compare the two viruses, but to point out that the effect of quarantine did exactly what we expected it to do.
We expected the resurgence of the virus. Let’s say that again. We expected it. However, the media and many health professionals that I interact with seem horrified that it occurred.

We predicted this pattern months ago.
I am surprised at the number of health professionals that are just beside themselves about this virus. I recognize that, in its most severe form, this virus can be deadly. And, so is the flu, RSV and other RNA viruses. Do these professionals not read history? Do they not read the actual scientific literature? Do they not see the patterns that diet and control of hyperinsulinemia have on this virus?
Instead, these medical professionals have remained quiet, and in some cases cheered, as our government over-reach and personal liberty infringement took place. We’ve lost our ability to travel, participate in group gatherings and church services. Quarantine, mask wearing and social distancing has essentially done nothing for our community in the last 3 months.
Our initial reasoning for quarantine was to take the peak off of hospitalizations. That was done. Yet continued suppression of personal liberties has done nothing for the overall health of our society. The second wave of infection was going to occur no matter what we did.
Instead, the media fear mongering, social distancing and force wearing of masks has lead to increased risk of suicide, overdose and drug addiction. Estimates are as high as 150,000 deaths due to the effects of quarantine and social distancing mandates. In fact, much of the anxiety and PTSD that is expected will not be seen until 4-6 month after the quarantine occurs.
According to a recent JAMA report, “It is possible that the 24/7 news coverage of these unprecedented events could serve as an additional stressor, especially for individuals with preexisting mental health problems.” Our routines have been completely upended and even things like wearing a mask or waiting in lines at the grocery store can make you feel tense.

Some common signs of pandemic-induced stress are:
What we know from research after the SARS outbreak is that post-traumatic stress (PTSD) is possible, especially in front line healthcare workers. In one particular study, about 10 percent of the hospital employees had had high SARS-related PTSD symptoms post-outbreak. And about half of them still had symptoms three years later. Other studies have shown that when a person’s PTSD symptoms persist for more than 6 months after an event, they are very likely to continue to persist over the long term.
A significant part of the problem in both the lay public and among health care workers is confusion about actual risk of disease, what can be done to prevent/treat the disease, and how to access treatment. I see this confusion today in many physicians and nurses I interact with in my community.
If you are having symptoms of anxiety, stress or depression, don’t be afraid to reach out for help. Knowledge is power. The more you know, the less fear and anxiety you will have.
Wear your mask if you want. Initially, when we didn’t know how invective this virus was, I was all for using any protection available. But, since the end of April, the data has changed my mind. Wearing a mask isn’t doing anyone any good.
Some cities and states have mandated mask wearing. I’m not telling you to break the law. I am saying that the mask mandate has done nothing to “slow the spread” as so many people have now bought into. Research demonstrates that homemade masks to little to stop the spread of viral infections and surgical mask that have been properly fitted and worn correctly decrease this risk of viral spread by only 2-5%. In the most recent review of the mask wearing literature, the authors stated, “The evidence is not sufficiently strong to support widespread use of face-masks as a protective measure against COVID-19. However, there is enough evidence to support the use of face-masks for short periods of time by particularly vulnerable individuals when in transient higher risk situations.”
What is effective is washing your hands regularly with soap and water, avoiding those who are actually sick or have fevers over 101 degrees, eating a healthy diet that prevents diabetes risk and getting adequate sleep. Those at high risk for infection can and should be vigilant about avoiding exposure.

I’m not sure what it is about this time of year . . . maybe the post-holiday weight gain, or the fear of pulling out a swimming suit in a few months. But I have had a number of people, both men and women, in the office with excessive estrogen levels.
Estrogen excess and estrogen dominance are two hormone abnormalities I find commonly in both men and women in my practice. These two issues are frequently complicating factors that make feeling good and weight loss difficult. They are, also, often the main reasons people don’t see dramatic improvement in a person’s symptoms of energy, fatigue and mental clarity when they’ve already changed their diet and lifestyle.
IMPORTANT NOTE BEFORE WE GO ON: This information applies to patient who already have normal thyroid function and corrected insulin resistance. If your thyroid is off or if you are still significantly insulin resistant, it will affect estrogen and other male and female hormones, so follow a ketogenic diet and get your thyroid balanced FIRST!
I’ve addressed estrogen dominance in a previous blog post. You can find it here. Estrogen dominance is a condition where there is an abnormal estrogen/progesterone ratio. The estrogen/progesterone ratio MUST be balanced. Normal estrogen levels with low progesterone (this can commonly occur with the use of a synthetic progestin (HRT) in female patients) is a common scenario that falls into the estrogen dominance pattern.
Estrogen excess is a situation where progesterone levels may be normal but estrogen is elevated (an abnormal ratio can also be present in this condition).
The symptoms of excess estrogen can be:
Estrogen naturally stimulates cells to grow and multiply. Natural estrogens are essential. But, too much estrogen increases thyroid binding globulin, inactivating the thyroid function causing abdominal weight gain. Too much estrogen changes the body’s ability to remodel bone.
Estrogen is essential to stabilize the inner lining of arteries, however, excessive estrogen doubles one’s risk for stroke and increases the risk of coronary atherosclerosis and heart attack. Too much estrogen increases the size of the prostate, increases risk of prostate cancer and increases the risk of rheumatoid arthritis.
Estrogen excess is an elusive condition. Measuring estrogen levels is not frequently done, and most doctors were never trained to look at the three separate forms of estrogen in men and women. I had no idea this was an issue until about five years ago.
What causes excess estrogen?
The eleven most common causes of estrogen excess are:
Other diseases can cause estrogen ratio’s to be elevated. These include liver disease, zinc deficiency, excessive alcohol intake, obesity, calcium deficiency, insulin resistance, diabetes, and excessive testosterone therapy.
These hormones, like estrogens, progesterone and testosterone can be easily checked by your doctor through blood or salivary testing. The key is a balance in the ratio between progesterone and estrogens.
The two estrogens that are essential to test are:
These can be ordered through your doctor. Estrogens can take 2-3 months to balance out. It may take some time after making changes to see your levels normalize. Don’t fret.
When natural methods of lowering estrogen levels are ineffective, then your doctor will recommend treatment. A number of other effective medicinal approaches including:
In my clinical experience, a ketogenic lifestyle is foundational to balancing these hormones consistently and naturally. Carbohydrate restriction by itself corrects many of the diseases of civilization. I addressed this in my book The Keto Cure. For many, there are few more steps necessary to living a long, happy and healthy life.
In my office, in addition to the ketogenic or carnivorous diet, I add on Berberine Plus 500mg twice daily with meals. This has been shown to notably improve the insulin resistance, lower estrogen and improve progesterone naturally.
Years ago, this was hard to find, so I created my own supplement line and these can be found at Ketoliving.com. Go to Ketoliving. com and order your bottle of Berberine Plus right now, before it is too late. I designed my own pharmaceutical grade berberine so that my patients could make sure they are getting real berberine in the doses I want you to have.
The treatment of this issue isn’t difficult. There is much more to come on this subject. I will address each of the progesterone, testosterone, DHEA and sex hormone binding globulin abnormalities in my future blogs. So, keep an eye on my web page DocMuscles.com/blog/.
So, get your hormones checked by someone who understand this problem and knows how to treat it. Second, limit estrogen stimulating sources in your diet and environment. Third, control you diet and order a bottle of Berberine Plus right away.
I’ve had many of my patients and followers on social media ask about my continued use of the hashtag #JustKeepEsterifying. Well, here is the answer. Check out the short 4 minute video below to get the answer:


The most common complaint that I get in my office when someone has started a ketogenic diet is, “Doc, I feel fatigued. Will this ever go away?”
That feeling of fatigue, some refer to as the “keto-flu,” is usually due to a couple of things. First, you may not be eating enough fat (I recommend a 1 gram to 1 gram ratio of protein to fat when getting started). Second, you’re not taking in enough salt (specifically sodium, potassium, magnesium and/or zinc). These four salts are essential electrolytes our body requires for proper function.
If salt is the problem, the you will be experiencing leg cramps. Cramps during daytime activity are usually due to low sodium or potassium levels. Cramps that wake you up at night are usually due to low magnesium or zinc. Leg cramps can also be due to hypothyroidism or significant blood sugar swings. Dr. Nally will usually check for this during your visit with him.
“But isn’t too much salt bad for you?” I am frequently asked.
Too much salt is only bad for you if you’re eating a “low-fat” diet.
What if increasing salt intake actually lowered your blood pressure?
Did you know that increasing your salt intake can actually improve your diabetic blood sugar if you are following a correct diet? Could it be that easy?
Almost every patient that I see in the office has a significant worry about salt intake, some greater than others. In fact, some people are so fearful about salt that when I initially began encouraging its use, they told me that I was crazy, and they left my practice.
Has restricting salt over the last 50 years really worked, or is it doing more damage than we think?
That was the question that was asked by Dr. Ames in the American Journal of Hypertension 17 years ago. However, his answer never got a mention. In fact, I’ve been in practice for almost 20 years, and incidentally stumbled upon this article when it was mentioned by a colleague of mine. Granted, the study is a small sample size of people, only twenty-one. However, the results are profound.
Twenty-one patients with hypertension were randomized to periods of no salt (placebo) and periods of 2 grams (2000 mg) of sodium chloride four times a day (a total of 8 grams of salt per day). Glucose tolerance tests were completed with insulin levels at the end of each intervention period.
Insulin Resistance and Hypertension Improve by Adding Salt
Three very noteworthy results happened. First, those patients with insulin resistance and diabetes had improvement in their glucose levels while on 2 grams of sodium supplementation.
Second, those with hypertension also, shockingly, showed improvement in their blood pressure while on the 2 grams of sodium supplementation.
Third, those with insulin resistance had a lowering of their insulin levels during the period of increased sodium intake. These findings fly in the face of the dogma that’s been drilled into our heads that “salt is bad!”
“But, Dr. Nally, you can’t base your findings on a small group of 21 people,” the experts say.
Yes, it is a small study group. However, these findings are identical to what I, also, see clinically every day in my practice for over 20 years.
We know that the average human needs at a minimum 3 grams of sodium per day and 3 grams of potassium per day. The standard American diet (SAD diet) including processed foods contains 2-3 grams per day of sodium and potassium. In fact, the CDC claims the worst salt containing meals for you are:
Insulin also stimulates additional retention of sodium at the kidney level. If you are insulin resistant, producing excess insulin in response to starches or sugars, you retain notably larger amounts of salt when eating the standard American diet (SAD diet) or a “low-fat” diet. However, if your following a low-carbohydrate or ketogenic lifestyle, you won’t be eating the meals above and you’re probably not getting near enough salt.
Salts, or electrolytes, are essential in normal cellular function. Low salt in the body is like running your car without oil. It will run, but not very efficiently and over the long term will cause problems. This is the cause of the keto-flu I wrote about previously. And, according to the study above, it is a potential driver of our persisting insulin resistance, diabetes and hypertension.
How Much Salt Should I Use?
In my office, I encourage use of 3-4 grams of sodium and 3-4 grams of potassium daily when using a ketogenic lifestyle. That’s approximately 1 ½ – 2 teaspoons of salt per day. I like the Redmond’s RealSalt or pink Himalayan salt because these products contains all four types of salt (sodium, potassium, magnesium and zinc).

It is probably that your salt restrictions is making your insulin resistance and blood pressure worse. That’s what the clinical evidences are pointing toward, and it is what I see every day in my office.
Want to know more about a ketogenic life-style? Click the KetoLife link to get some basics.
If you’re already following a ketogenic lifestyle, then let me help you navigate the bumps and turns by going to the KetoKart and checking out the products I recommend to jump-start ketosis DocMuscles-style!
Until then, I’ll have another piece of bacon, please . . . and, oh, pass the salt!

What if increasing your salt intake actually improved your diabetic blood sugar?
What if increasing salt intake actually lowered your blood pressure? Could it be that easy?
Just about every patient that I see has significant worry about salt intake. Some greater than others. In fact, some people are so salt phobic that when I encouraged its use, they called me a “quack” and left my practice. But does salt restriction really work, or is it doing more damage than we think?
That was the question that was asked by Dr. Ames in the American Journal of Hypertension 17 years ago. However, his answer never got a mention. In fact, I’ve been in practice for almost 18 years, and incidentally stumbled upon this article when it was mentioned by a colleague of mine. Granted, it is a small sample of people, only 21 in the study. However, the results are profound.
21 patients with hypertension were randomized to periods of no salt (placebo) and periods of 2 grams (2000 mg) of sodium chloride four times a day (a total of 8 grams of salt per day). Glucose tolerance tests were completed with insulin levels at the end of each intervention period.
What was noteworthy was that those with insulin resistance and diabetes had improvement in their glucose levels while on sodium supplementation. Those with hypertension had improvement in their blood pressure while on the sodium supplementation. Lastly, those with insulin resistance had a lowering of their insulin levels during the period of increased sodium intake. These findings fly in the face of the dogma that’s been drilled into our heads that “salt is bad!”
“But, you can’t base your findings on a small group of 21 people,” the experts say.
Yes, it is a small study group. However, these findings are what I, also, have seen clinically in my practice for over 13 years.
We know that the average human needs 3 grams of sodium per day and 3 grams of potassium per day. If you’re eating the standard American diet (SAD diet) including processed foods, you’re getting 2-3 grams per day of sodium. In fact, the CDC claims the worst meals for you are:
However, if your following a low-carbohydrate or ketogenic lifestyle, you won’t be eating the meals above and you’re probably not getting near enough salt. This is the cause of the keto-flu I wrote about a few weeks ago. And, according to the study above, it is a potential driver of our persisting insulin resistance, diabetes and hypertension.
In my office, I encourage use of 3-4 grams of sodium and 3-4 grams of potassium daily when using a ketogenic lifestyle. That’s approximately 1 1/2 – 2 teaspoons of salt per day. I like Redmond’s RealSalt or if you can’t find it, Himalayan Pink Salt, because the pink sea salts contain sodium, potassium, magnesium and zinc.

Could it be that salt restrictions are making our insulin resistance and blood pressure worse? That’s what the clinical evidences are pointing toward. However, more research is still needed.
Want to know more about a ketogenic life-style? Click the link on KetoLife above to get some basics. If you’re already following a ketogenic lifestyle, then let me help you navigate the bumps and turns by going to the Supplement section above and checking out the products I recommend to jump-start ketosis DocMuscles style!
Until then, I’ll have another piece of bacon, please . . . and, oh, pass the salt!

Inability to lose weight is the most common reason people see me. It’s often a combination of small things of which they are unaware. What simple things are keeping the spare tire inflated around the your waist? I’ve listed the eight most common reasons you can’t lose the fat.
About 85% of the people that walk through my office doors have some degree of insulin resistance. This means that they produce 2-20 times the normal amount of insulin in response to ANY form of starch or carbohydrate. Insulin is the hormone responsible for letting glucose into the cell to be used as fuel. More importantly, it is the hormone responsible for dampering glucose production in the liver and, it is the primary hormone responsible for pushing triglycerides into the fat cells (essentially, the master hormone for making you FAT). The more insulin you make the more fat you store. Insulin resistance, the inability for insulin to signal glucose dampering at the liver receptors, is the first stage that starts 15-20 years before you become a diabetic.
 In order to lose fat, you have to decrease the insulin to a basal level. If you don’t the fat enters the fat cell faster than it exits and the fat cells get bigger. This is RULE number one to weight loss. You gotta turn down the high insulin surge that 85% of us are really good at producing. If you don’t do this, it is almost impossible for many of us to lose weight.
In order to lose fat, you have to decrease the insulin to a basal level. If you don’t the fat enters the fat cell faster than it exits and the fat cells get bigger. This is RULE number one to weight loss. You gotta turn down the high insulin surge that 85% of us are really good at producing. If you don’t do this, it is almost impossible for many of us to lose weight.
For at least 1/3rd of the people I see, this cannot be accomplished unless TOTAL CARBOHYDRATES are decreased to less than 20 grams per day. Yes, you read that correctly . . . Less that 20 grams per day.
Yes, protein can cause weight gain. And, no, it’s not because gluconeogenesis is on overdrive. There is always a body builder that sends me a nasty message after I say this. But the fact is that it’s true. (I’ll keep an eye on my e-mail).

Five of the ten essential amino acids stimulate an insulin response. Remember why carbohydrates cause weight gain . . . ? (I will give you a hint . . . INSULIN).
Certain amino acids that make up proteins can do the same thing. Arginine, Lycine, Phenylalanine, Leucine & Tyrosine, in that order, stimulate insulin enough to halt weight loss or increase weight gain in a significant way (1). We need protein to stay healthy, but too much of these amino acids in someone who is insulin resistant will inhibit weight loss and stimulate fat gain. I’ve also seen it raise small dense LDL particles in the cholesterol (the heart disease causing particle driven by insulin over production) I’ve seen this time and time again with many people. Simply modulating down the protein to the calculated needs lets the weight start coming off again.
So, what foods contain these in the highest amounts? Sea lion liver (I know, this won’t go over very well with the polar bears), soy protein isolate, crab, shrimp, sesame flour, turkey breast, pork loin (it’s the leanest cut of pork – No. BACON is fine), chicken, pumpkin seeds, soybeans, peanuts, spirulina (blue green alge that is found in the sea).
Yes, I get it. We’ve been told these were the healthy foods for the last 50 years. But, think about it. When did we start gaining weight as a country? 50 years ago.
Too much chicken, shrimp, crab and soy foods will inhibit weight loss in those with insulin resistance. So, consider whether it should be chicken you add to your salad. Consider, instead, bacon or beef as a wonderfully tasty substitute.
How much protein do you need? My formula for calculating your individual amount is here in my blog Calculating Protein Needs.

To successfully lose fat on a ketogenic diet, 30-70% of your caloric intake should come from fat. Yes. You read that correctly. (The definition of a high fat diet is any diet containing more than 30% of fat from calories).
If we limit carbohydrates (which is currently 80% of the body’s fuel on the standard America plate), and moderate excessive protein which also halts weight loss, you have to replace the fuel. That fuel replacement should come from fat. Increasing fat will improve the sensation of fullness, provide all the fat soluble vitamins, and actually makes food taste good again.
As long as you are lowering the insulin to basal levels, you can actually eat all the fat for which you are hungry. Add bacon, butter, coconut oil, avocado, hard cheese, and oh, did I say bacon?
But Dr. Nally, what about all that saturated fat?
The saturated fat is only a problem with vascular disease, cholesterol and heart disease when the insulin level is also high at the same time. It’s the high insulin in the presence of large amounts of fat that drives the risk for atherosclerosis (vascular and heart disease). Instead of cutting out the fat, we’re cutting out the insulin.
How much fat should you be eating? Shoot for 60-70% of your calories from fat for the first 3 months. If your fat grams are slightly higher than or equal to your protein grams, you’re there. Listen to your body and eat fat until you’re full. That’s how most of my patients gauge their need and suppress hunger.
After the third month, most of us are fat adapted. You may notice your weight loss slows or halts. This means that our ability to absorb fat into the blood stream is dramatically more efficient. It also means that your taking in more fat into the fat cell then you are pulling out of the fat cell. I’ve found this to be the case with people who are loading butter, MCT or heavy whipping cream into their coffee. In this case, back off the “extra fat” your are loading or drinking. It’s not the calories in this case. There are 3-4 hormonal reasons this occurs once you are fat adapted. (We’ll talk about this in another blog post.)
 I know, I know. Tea is a national pass time in Europe. And, it is deeply embedded in the culture of many other countries. I’m probably not winning any friends across the pond by saying this, and it may bring back memories of the Boston Tea Party. However, the problem is that leaf based teas stimulate a rise in insulin (not taxes). I have had many patients hit a weight loss plateau because of the use of tea, specifically black tea, oolong tea, and green tea (2,3,4).
I know, I know. Tea is a national pass time in Europe. And, it is deeply embedded in the culture of many other countries. I’m probably not winning any friends across the pond by saying this, and it may bring back memories of the Boston Tea Party. However, the problem is that leaf based teas stimulate a rise in insulin (not taxes). I have had many patients hit a weight loss plateau because of the use of tea, specifically black tea, oolong tea, and green tea (2,3,4).
Yes, I am well aware of the tremendous benefits of the epigallocatechin gallate (ECGC) found in green tea. ECGC, which can be isolated as an extract, improves insulin resistance and improves GLP-1 signaling. ECGC has, also, been show to improve triglycerides (5). For this reason, it is one of the components in the KetoEssentials Multi-Vitamin I developed a few years ago and recommend to all my patients.
It appears, however, that the theaflavin within the leaf of the tea may be playing the offending role in the insulin spike seen with their use (6).
Lack of sleep has been implicated in difficulty with weight loss and weight gain (7). Lack of sleep places the body into a state of chronic stress. This elevates cortisol, lowers testosterone, increases insulin (there’s that insulin problem, again) and increases the other inflammatory hormones. This perfect storm of stress, driven by lack of restful sleep, plays a big role in fat loss.
My average patient needs at a minimum of 6-7 hours of restful sleep to maintain and lose weight.
This is where untreated sleep disorders like sleep apnea play a big role. If you have sleep apnea, get it treated. What else can you do to help improve sleep?
It may take your body and body’s biorhythm 3-4 weeks to adjust to changes you make around sleep habits. Be patient with yourself.
Just as lack of sleep is stressful, other forms of chronic stress also raise cortisol, insulin and the inflammatory hormones. Chronic stress also lowers testosterone. It, also, has the potential to lower neurosignaling hormones in the brain like serotonin and dopamine, putting you at greater risk for depression and anxiety.
Other forms of chronic stress can occur from poor relationships, chronic pain, stressful employment, unfulfilled expectations, chronic illness and all forms of abuse. If any of these are playing a role in your life, you need to address them, and address them now.
As a physician, my job is stressful. Dealing with life and death issues with multiple people through the day, six or seven days a week, takes it’s toll. I’ve found that weight lifting, horseback riding, and taking care of my animals are my outlets. Find something physical, that takes you outside in the elements and forces you to break a sweat for 15-20 minutes is the key.
 Our bodies have a “fight or flight system.” 100 years ago, the stress was fighting or running from the bear that squared off with you when you happened upon him in the woods. Cortisol, adrenaline, epinephrine, insulin, glucose, and inflammatory hormones pour into the blood stream. The heart beats faster, blood flows rapidly to the muscles, sensory awareness is heightened in the brain and increased oxygen flows to the lungs. This lets you fight the bear or run from the bear.
Our bodies have a “fight or flight system.” 100 years ago, the stress was fighting or running from the bear that squared off with you when you happened upon him in the woods. Cortisol, adrenaline, epinephrine, insulin, glucose, and inflammatory hormones pour into the blood stream. The heart beats faster, blood flows rapidly to the muscles, sensory awareness is heightened in the brain and increased oxygen flows to the lungs. This lets you fight the bear or run from the bear.
But, you can’t fight or run from your cynical boss. You can’t fight or run from oppressive finances, the person that cuts you off on your one hour commute in traffic, or your coworker who keeps pestering you. However, your body still releases adrenaline, cortisol, epinephrine, insulin and a number of inflammatory hormones prepping you to fight or run. If you don’t burn these hormones off, they halt weight loss, and actually can cause weight gain, increase anxiety and over time disrupt sleep.
So find your favorite way of physically relieving stress, and do it 2-3 times per week. (No, gentlemen, sex doesn’t count).
In the last few years, we’ve been able to identify a number of genetic deficiencies that play a role in weight gain. One of those is an methyl-tetrahydrofolate enzyme deficiency (MTHFR deficiency for short). This is a genetic deficiency in the enzyme that converts adds a methyl ion to the folic acid in the cells of your body.
This is important, because if you can’t methylate folic acid inside the cell, you’ll have difficulty using vitamin B12 and B6 very efficiently to form methionine (a key amino acid in blood vessel and nerve function). There are two genes that encode for the enzyme that does the methylation of folic acid. Deficiency in one or both of these can lead to problems.
In severe cases, it causes homocysteine to build up to unsafe levels in the blood and slow the formation of methionine. It is associated with B12 deficiency, weight gain, fatigue, migraines, depression, anxiety, neuro-developmental disorders like autism, pregnancy loss, blood clots and neuropathy in pre-diabetic and diabetic patients (8, 9, 10).
Giving extra vitamin B12, B6 and folic acid (vitamin B9) doesn’t appear to help. Clinical evidence is pointing to the pre-methylated form of the folic acid. Finding this pre-methylated form has been difficult and notably expensive for patients. I found this deficiency to be so prevalent in my office, I added methylated folic acid to the KetoEssentials Multivitamin.
We have become a very sedentary people. We have engineered physical activity out of our lives. Remote controls, elevators, escalators, people movers, and automation have made our lives physically easier.
The average office worker burns 300 kcal per day sitting at a desk on a computer. The average farm worker burns 2600 kcal per day. That’s the equivalent of running a marathon every day.
Physical activity doesn’t necessarily cause weight loss. However, physical activity changes the hormones of the body including increasing a hormones like catacholamines, testosterone and a hormone called atrial naturitic peptide (ANP). ANP opens the fat cell, and lets more fat out (11).
When physical activity is paired with the correct diet, the weight come off. This is where exogenous ketones may play a role. The increased presence of ketones in the blood increases the release of ANP helping to activate triglyceride release from the fat cell.
Don’t get me wrong, many of my patients can lose weight with just dietary carbohydrate restriction alone, however, if you’ve hit a stall, you may need to look at your physical activity levels and many people like me, who are notably insulin resistant, benefit greatly with the addition of exogenous ketones.
Is your fat loss on a plateau? Knowing that these challenges plague people on and off throughout the year, and, seeing people get hung up on these issues, I’ve created the Ketogenic Lifestyle 101 Course. This program gets you jump-started into ketosis and gives you the tools to overcome the individual hurtles you will experience on your health journey.
If your the really motivated type, and want a true 30 day challenge, then join my Kickstart program.

Do you have the keys to your “fat lock-box?”
Lock-boxes have always fascinated me. Lock-boxes with special keys are even more fascinating. The more I’ve learned about fat cells (adipocytes), the more I think about them as special fuel depositories or fat lock-boxes. Before the invention of refrigerators, fast-food, Bisquick and beer, our bodies preserved and reserved fat as a precious commodity.
The body, when given fat with carbohydrates or excess protein, quickly places the fat into a lock-box for safe keeping. It does this for two reasons. First, the body can store fat very efficiently. Second, hormone signals stimulate fat storage when other fuel sources (carbohydrate & protein) are present in excess. The body can access this stored fuel only when the right presentation of hormonal keys are present. Fascinatingly, we now know from recent research, there are actually three types of lock-boxes for fat in the human body (white adipose tissue, brown adipose tissue, and tan adipose tissue).
The greatest challenge for the obesity doctor is getting into the fat lock-box. Some people’s boxes are like the “Jack-in-the-Box” you had as a child – just add a little exercise spinning the handle and the box pops open (These are those people that say, “Oh, just eat less and exercise and you’ll lose weight.”) For the majority of the people I see, it’s more like the lock above with a four or five part key required to turn the gears just right. (And, that key often only seems available on a quarter moon at midnight when the temperature is 72 degrees.) Fat cells, called adipocytes, require four, and possibly more, keys to open them up and access the fuel inside. Exercise is only one of those keys. However, exercise alone often fails.
Over the last 18 months, I have been surprisingly impressed with the results patients have by the addition of both medium chain triglycerides and exogenous ketones. A number of people have asked me, “Why do you encourage the addition of exogenous ketones to a person already following a ketogenic diet?”
Others just accuse me of self promotion, saying, “You’re just trying to sell a product!”
Or they exclaim, “Giving more ketones is just a waste of time and money.”
A few of the uneducated holler from across cyberspace, “You’re just going to cause ketoacidosis!”
Believe me, I’ve heard it all. And, the skepticism is understandable. I work with people every day, looking closely at weight gain/loss, metabolism, cholesterol, blood pressure, inflammation, etc. With any “low-carb” or “ketogenic product,” I test it out on myself and my family, before I offer it to my patients or even consider encouraging its use in my practice. I have this desire to understand “the how” and “the why” before I prescribe the who and when.
First , let’s talk about the adipocyte as a fat lock-box – and where you find the keys. Then, we’ll discuss how products may or may not help.
There is only one door INTO the adipocyte for the fat, and the key to that door is insulin. Insulin stimulates an enzyme called lipoprotein lipase that essentially pulls the fat from the cholesterol molecule into the fat cell. Without insulin, fat doesn’t enter the fat cell. As a result, type I diabetics (those that make absolutely no insulin) look anorexic if they don’t take their needed insulin. Insulin is also the first key to the back door on the adipocyte. Actually, if there is too much insulin in the system, fat enters easily through the front door but cannot exit the back door (Picture 1). Insulin seals up the back door so that fat cannot exit very effectively.
That’s why insulin is the master hormone when it comes to obesity. You’ve got to lower the over-all insulin load to get the adipocyte slowing fat entry and increasing fat exit. If you don’t do that, I don’t care how much you exercise, 85% of the population will struggle with weight loss. Hmmm, seems kind a familiar to the last 50 years of our obesity epidemic, No?

The second key to the back door of the fat cells are the catecholamines. These are adrenaline (epinephrine), norepinephrine, adrenocorticotropic hormone (ACTH) and even serotonin. These hormones are produced in the adrenal glands through exercise, fear and even recollection of powerful memories. Medications can also stimulate production of these hormones. The catecholamines stimulate cAMP. cAMP opens the fat cell, releasing fatty acids for fuel.

The thyroid hormone conversion of T4 to T3 also plays a role in uptake of the catecholamines by adnylyl cyclase (AC). Low levels of T3 (like those seen in hypothyroidism or in cases of thyroiditis) also inhibit unlocking of the fat lock-box. Conversion of T4 to T3 is driven by the presence of bile salts in the gut. Increase fat intake increases the presence of the bile salts which naturally leads to better T3 conversion. Hence my constant references to eating more fat and bacon. .
The third key is an inhibitory effect on adenylyl cyclase (AC) activity by alpha and beta adrenoreceptors, adenosine, prostaglandins, neuropeptide Y, peptide YY, HM74-R & nicotinic acid. These inhibitory and inflammatory hormones produced in the brain, gut and other areas decrease cAMP activity in the fat cell and slow fat loss. The fancy long names are all hormones causing inflammation. Of note, many are also stimulated by medications including blood pressure lowering drugs. Check with your doctor if the medications you are taking may be causing weight gain, or halting your weight loss.
Please note that the first three keys have effect on the cAMP pathway for release of fat from the adipocyte. These three keys turn on or off effective function of cAMP leading release of fatty acids from the fat cell.
The fourth key follows a separate pathway. This is why I’ve clinically seen patients experience weight loss even in the presence of higher insulin, inflammatory disease or hypothyroidism. This key activates release of the naturitic peptides (ANP, BNP). These hormones are released from the heart when it squeezes more powerfully. As the cardiac muscle contracts, it releases ANP & BNP hormones. These hormones stimulate the cGMP pathway in the adipocyte. It then activates hormone sensitive lipase (HSL) and perilipin to release free fatty acids. Again, this pathway is separate from the pathway by which the first three keys released fat. Exercise increases heart contractility, but is inhibited by high insulin levels. However, ketones themselves also stimulate this increased contractile effect.
There actually is a fifth key not referenced above. The fifth key to the fat lock-box amplifies testosterone’s presence through the HPG axis. Insulin resistance and leptin resistance lower testosterone in men and raise it in women, causing poly-cystic ovarian syndrome (PCOS). Normalizing insulin levels (with a ketogenic diet) while at the same time increasing ketones as the primary fuel powerfully resets the HPG axis through a complex series of hormonal reactions. Growth hormone is balanced and testosterone returns to a normal range.
Clinically, 60% of the people I see in the office have abnormal testosterone due to insulin resistance. This leads to hypogonadism in men and PCOS (abnormal periods, facial hair growth and/or infertility) in women. Restricting carbohydrates and maintaining nutritional ketosis by diet and/or addition of exogenous ketones has a powerful corrective factor in these people.
Testosterone influences the up-regulation of the alpha & beta adrenergic receptors (the 2nd & 3rd key above). Hence, if your testosterone is low, it has a suppression on the way that the catecholamines influence fatty acid release from the fat cells. If your testosterone and growth hormone are normal, muscle development and adrenaline stimulus from exercise helps amplify the use and mobilization of fat from the fat cell. In people with insulin resistance and leptin resistance, exercise and the catecholamines don’t have the same fat burning effect.
Yes, I have greatly simplified a series of very complex hormonal pathways in the explanation of the keys above. Why do you think understanding obesity has been so difficult? Think of your adipocytes as a fat lock-box.
What’s even more important is the knowledge that the fat cell DOES NOT open or close because of calories. There is no dogmatic calorie-meter on the wall of the fat cell. There is no calorie key to the fat lock-box. Really, . . . in the 50 years of studying fat, researchers haven’t found one. (Prove me wrong when you show me an electron micro-graph of a calorie-meter in the wall of a cell). Science has demonstrated multiple times that the lack of food from starvation or excessive fasting suppresses thyroid function (an inhibitory effect on key #3). Restricting calories actually inhibits fat loss in many people.
The fat lock-box keys I refer to above are hormone responses to the presence of macro-nutrients (food). That means, first reduce your carbohydrate intake by eating real food from good sources. You can learn how to get started by registering for my FREE six part weight loss mini-course. Second, be as active as you can. Third, reduce stress and medications that have inhibitory effect on catacholamines. Fourth, balance your thyroid. And, fifth, get into ketosis and consider adding exogenous ketones to your dietary regimen. It really is that simple.
(For those of you that still believe there is a calorie key – or just need something to do while in the bathroom):
Two out of ten people that he sees in his office have signs of fatty liver disease. What does that mean to society and how does it affect you?
Spend 11 minutes with Dr. Nally as he discusses the cause of Fatty Liver Disease and discusses the most effective method he has found to treat it. What is the underlying cause? Watch and find out.
Watch as we discuss Type II Diabetes from the perspective of insulin resistance and how using a ketogenic diet/lifestyle as well as exogenous ketones, KetoEssentials Multivitamin and supplements like berberine play a role in improving your health.
Grab your bacon, butter and pecans, . . . pull up a chair, and enjoy!!
Pull up some pork rinds and a glass of KetoMax and check out my video blog on Insulin Resistance 101. Let me know your questions as we go and I will add them to future videos or blogs.

This week on Episode #50 of KetoTalk.com we talked about those proteins highest in arginine and lysine with the greatest potential for spiking your insulin and kicking you out of ketosis. Here is a Graphic to give you a little help:


How does ketosis help the diseases of civilization? Find out as Dr. Nally answers these and many other pertinent dietary questions this evening.
You can learn more about his multi-vitamin supplement he designed for insulin resistance/diabetic/weight management patients that he mentions in the video here at KetoLiving.com.
You can learn about exogenous ketones that he mentions helps to augment ketosis here at DymaicKetones.com.

What is Insulin Resistance? Dr. Nally talks about the nuts and bolts of this syndrome and how it works. He answers multiple questions regarding diet and insulin resistance. Let me know what you thing and what questions future videos should answer.
Why should you consider using a ketogenic lifestyle? There are many reasons. This is part 8 of a 25 part series and this one focuses on how ketosis improves testosterone in men and estrogen in women.
Watch and enjoy!!
I had the chance to appear for an interview on Vicki Fitch’s podcast last night: A Fresh Perspective. We talked about bacon, ketogenic diets, hypoglycemia, sweeteners, food cravings, #FitchSlaps, exogenous ketones and we answered a bunch of great questions from the Facebook Live audience. You can see video of the show below:
Had a great time. Let me know what you think. Thanks, Vicki!!

Listen to KetoTalk Podcast #32 where we talk about hereditary angio-edema, adequate ketone ranges, statin use while in ketosis and healthy keto questions. You can listen in by going to KetoTalk.com or you can listen in on iTunes.


Listen in today as Jimmy and Adam blaze through a bunch of listener questions in Episode 27 of KetoTalk with Jimmy and the Doc!

KEY QUOTE: “Children are born in ketosis, so ketones are perfect for babies. The level of fat in breast-milk is essential for them to maintain their health and their growth.” — Dr. Adam Nally
Here’s are the 12 questions Jimmy and Adam answered in this special Keto Talk Mailbox Blitz extended podcast today:
– Testimonial from someone who learned his lesson why it’s important to stay ketogenic all the time
– Three-decade study confirms saturated fats are bad for health
– Is increased testosterone from a ketogenic diet a bad thing for women?
– Why am I still struggling with low energy and low ketones after months of being in ketosis?
– Can being in nutritional ketosis above 1.0 mmol cause painful headaches?
– Do artificial sweeteners and stevia raise insulin?
– Is my ketogenic diet causing me to cramp up before and during my half marathon racing?
– Is MCT oil a better fat to use on a ketogenic diet than other fats like coconut oil, cream, or butter?
– Why do I have a constant stomachache while I’m on a ketogenic diet?
– Do you have to be in ketosis to burn fat?
– Does being in ketosis lead to daily spotting and extended periods?
– Are ketones in my baby’s breastmilk safe for her to consume? And why did my milk supply drop when I went keto?
– What is the impact of the supplement creatine on ketones, blood sugar, and insulin levels?
– Can I ease into ketosis as a way to avoid the dreaded “keto flu?”
KEY QUOTE: “If you’re not feeling energy after that adaptation period of 2-4 weeks at the very most, then you’re doing something wrong. Let that be your wakeup call to change something.” — Jimmy Moore

Listen in here at KetoTalk.com or you can download the episode for free on iTunes.
Listen in to KetoTalk.com for Podcast #26.
The health podcast legend, Jimmy Moore, and I talk about how much fat is too much. Or, is it? What’s the deal with Zero-carb ketogenic diets? We answer your questions and try to give you the most up-to-date knowlege regarding the ketogenic lifestyle and how it affects your metabolism. We zero in exclusively on all the questions people have about how being in a state of nutritional ketosis and the effects it has on your health.
There are a lot of myths about “keto” floating around out there and we shoot them down one at a time.
You can down-load it for free on iTunes or listen to KetoTalk.com on your computer.
Enjoy!!


Does your diet really reverse vascular disease? I mean, will the diet you’re following ACTUALLY reverse the plaque burden that has occurred over the years of eating the SAD diet (Standard American Diet)?
It appears that the ketogenic diet does. At least that’s what research is showing, and that’s what I am seeing clinically. Let me give you an example. Reversal of vascular disease is what I saw last week in this patient case study in my office.
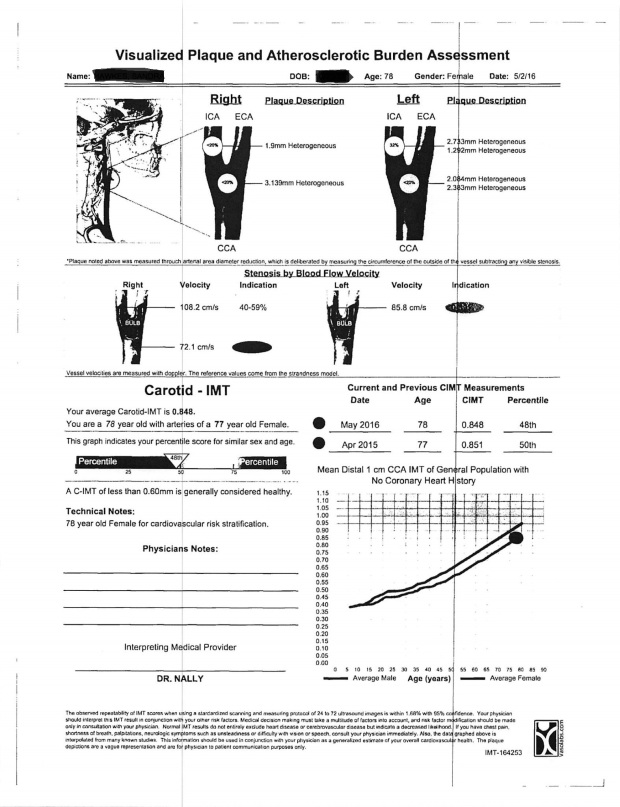
Meet “Mrs. Plaque” (name has been changed to protect her identity). She is a very pleasant 78 year old female who has been seeing me as a patient for the last 10 years. We identified worsening cholesterol and hyperinsulinemia in this patient a few years ago, and last year, she finally decided to go on a ketogenic diet after we noted slight worsening blood sugar (HbA1c increased to 6.1%), worsening cholesterol and a recent TIA (transient ischemic attack or “mini stroke”). We identified a 44% blockage in her left internal carotid artery and a 21% blockage in the right internal carotid artery putting her at risk for further cerebral ischemic events like a stroke and/or other vascular events like a possible heart attack down the road. She refused STATIN therapy as she had previous myalgia and side effects with their use in the past.
Past Medical History: Hyperlipidemia, Impaired Fasting Glucose (Pre-Diabetes),.Asthma, GERD, Irritable Bowel, Generalized Anxiety, Idiopathic Peripheral Neuropathy, Surgical Menopause (Hysterectomy) with Secondary Atrophic Vaginitis, Recent TIA, Cataracts, Appendectomy
Medications: Plavix 75mg one daily, Premarin Cream 0.635mg every other day, Xanax 0.5mg at bedtime for anxiety, Lyrica 50mg one nightly for neuropathy, Vitamin D 2000 IU daily , TUMS 750mg twice a day.
Her carotid ultrasound and carotid medial intimal thickness (CIMT) study completed April 1, 2015 is present below. You can see that her intimal thickness is only slightly higher than the average female her age, however, she has notable internal carotid artery blockage in both the right and the left sides.

The “mini stroke” and the report above, convinced her that she needed to tighten up her diet. The patient’s husband was also a diabetic and the patient had been “partially” restricting sugar in her diet up to this point in time, however, she had not fully jumped on the ketogenic band wagon. At this point she decided to change her diet.
She was placed on a ketogenic diet, restricting her carbohydrates to no more than 20 grams per day and increasing total fat to >50-60% of her total calories. Nothing else changed including her medications. She followed this program for the next year and this is the blood work that she had while following this program:
| 4/2/2015 | 8/4/2015 | 11/6/2015 | 5/12/2016 | |
| HbA1c (%) | 6.1 | 5.8 | 5.2 | |
| Tot Chol (mg/dL) | 224 | 156 | 230 | 233 |
| HDL (mg/dL) | 76 | 76 | 87 | 96 |
| LDL-C (mg/dL) | 134 | 65 | 128 | 123 |
| Small Dense LDL-P (nmol/L) | 481 | 150 | 222 | 217 |
| Triglycerides (mg/dL) | 72 | 76 | 74 | 68 |
| Fasting Insulin (uIU/mL) | 12 | |||
| Glucose (mg/dL) | 91 | 95 | 92 | 85 |
Because she was already partially restricting her sugar intake, her triglycerides and small dense LDL particle number was not bad, however, her average blood sugars were still significantly elevated. Weight decreased from 127 lbs to 119 lbs in August. She admits to slightly increased protein intake over the holidays and her weight increased back up to 125 lbs as of her last visit.
These labs also demonstrate that Total Cholesterol and LDL-C don’t appear to correlate with regression of plaque.
The image below is the patient’s repeat CIMT and carotid ultrasound 13 months later through the same lab. What is dramatic is that she has had over 10% regression in the plaque in both internal carotid arteries and a return of her carotid intimal thickness to the average female in her age bracket.
This case study is consistent with the findings of Dr.Shai and his group when they did a two year comparative dietary intervention study of Low Fat – Group 1, Mediterranean Diet – Group 2, and a Ketogenic Diet – Group 3 on vessel wall volume and CIMT.
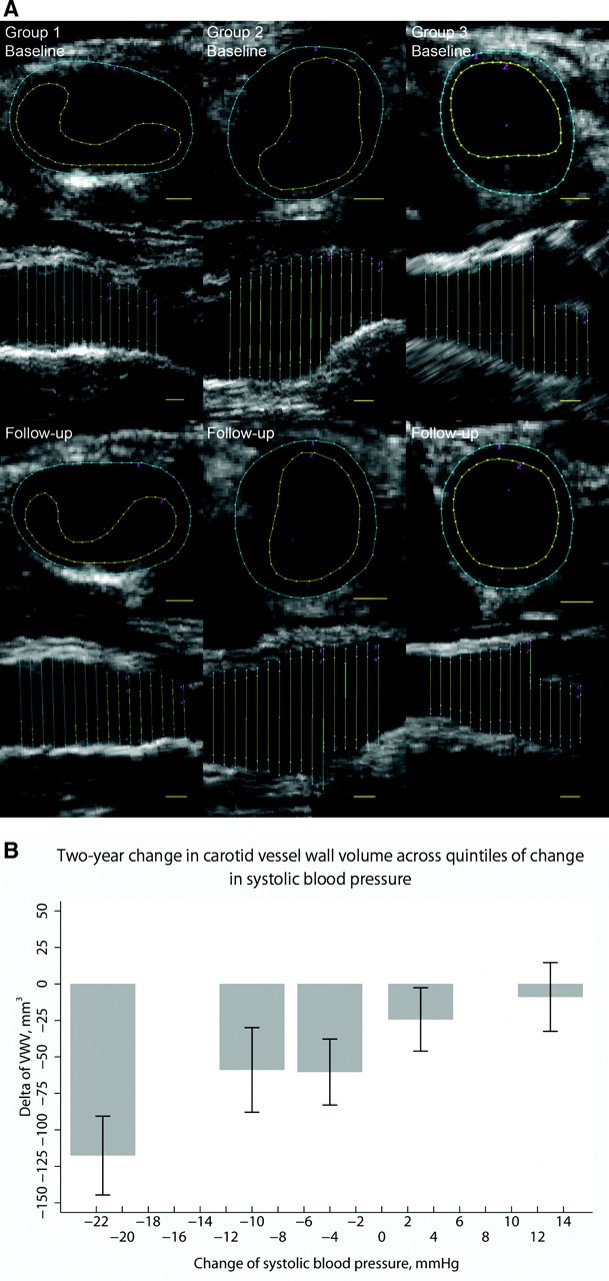
Carotid IMT changed by −1.1% from 0.816 mm at baseline to 0.808 mm after 2 years (P=0.18), with no significant difference between diet groups (P=0.91). There was a trend toward significant correlation between the 2-year changes in carotid IMT and VWV (r=0.173, P=0.056).
So, does your diet reverse vascular disease? Evidence is pointing to the fact that the ketogenic diet does. I return to the statement Hippocrates made over 2000 years ago, “Let food be thy medicine, and let medicine be thy food.”
Oh, and pass the bacon.
Ever wondered if it is possible to change up your metabolic genetics for the better? Come join me this week. I’ll be speaking about Ketogenic BioHacking, Thursday, March 31st, in Scottsdale, Arizona. Meet me from 7-8:30pm and learn how to improve fat burning, bio-hack your epi-genetic metabolism for improved blood sugar, cholesterol, blood pressure and so much more . . .
You’ll also get to meet Kim Minert who will be signing her new book, Burn Fat for Fuel. And, you’ll get a chance to meet the amazing Abigail Epps-Kluttz, body builder, fitness model & Pruvit Ambassador.
You can sign up at the Eventbrite link here. I look forward to seeing you!!
“It’s a snake.”
“It’s a wall.”
“It’s a rope.”
“It’s a fan.”
“It’s a tree.”
“It’s insulin resistance.”
I’ve always been fascinated by those describing a “new finding” in medicine. I am reminded of the story of 5 men who, never having seen an elephant before, were blindfolded and asked to describe what he discovered. However, each man was introduced to a different part of the elephant. Each of them had a dramatically different description of the elephant and each made a conclusion that was very different from the others.
What is fascinating, is that we usually make our “blindfolded comparisons” to those things we have seen or about which we have some descriptive understanding. Observing and describing human physiology is much like examining an elephant while blindfolded for the first time.
This week’s “blind-folded finding” is what has been interpreted by some as “insulin resistance” made worse by a ketogenic diet. Really? This perked my curiosity, because I’ve personally been following a low-carbohydrate/ketogenic diet for years and have thousands of patients doing the same. To this day, I’ve never seen insulin resistance “get worse.” In fact, it gets better. Clinically, it seems to take about 18-24 months to improve, but, it usually gets better.
THE QUESTION –
I’ve had three people from around the world contact me this week and ask why, after being on a ketogenic diet and “in ketosis,” they suddenly get a notably large blood glucose spike when they cheat. By notably large, I mean that their blood sugars rise to over 200 mg/dl within 2 hours of a carbohydrate containing meal. Now, they admit to rapid glucose recovery within an hour or two, and their hemoglobin A1c levels are subjectively normal (less than 5.6%). The worry is “am I becoming diabetic?” They also complain that after having been in ketosis for longer than 3-4 months, they cannot get their fasting blood sugars below 100 mg/dl.
Those asking me the question about this anomalous “physiological insulin resistance” referred to a couple of off-the-cuff blogger’s posts from 2-3 years ago referencing a few small studies (some of which were very poorly designed) [here, here, here & here] in the journals from 10-20 years ago. These articles describe a physiologic response interpreted as worsening “insulin resistance.” However, if you understand what is actually occurring in the Ketonian (yes, I made that term up – there will soon be a whole village of us), I see it as a normal physiologic response. It is misinterpreted by those who’ve never actually seen long term ketogenic physiology, as anomalous, in the average human.

THE ANSWER –
I’ve been seeing this slight elevation in fasting blood sugar with normal or low normal HbA1c in myself and many of my patients for quite some time. However, I never saw it as “insulin resistance” worsening. Clinically, when I tease out the food logs, it usually ends up being protein intake is too high, the person is using a sweetener or creamer causing rebound morning glucose elevation or, in those with low normal HbA1c’s (4.3-5.6%), it is in actuality a protective mechanism of “physiologic glucose sparing” in the keto-adapted individual (1, 2).
It can very easily be explained when one understands how ketones are actually used in the keto-adapted individual. First, a wonderful figure below (Thank you for pointing me to this one, Dr. Peter Attia) found in Dr. Veech et. al.’s paper (3) gives us an overview of how ketones skirt the TCA cycle within the mitochondria of the cell, causing inhibition of pyruvate dehydrogenase leading to glucose sparing by the cells of the brain that still require it’s availability (Oh, by the way, this is how we survived harsh winters and famines).
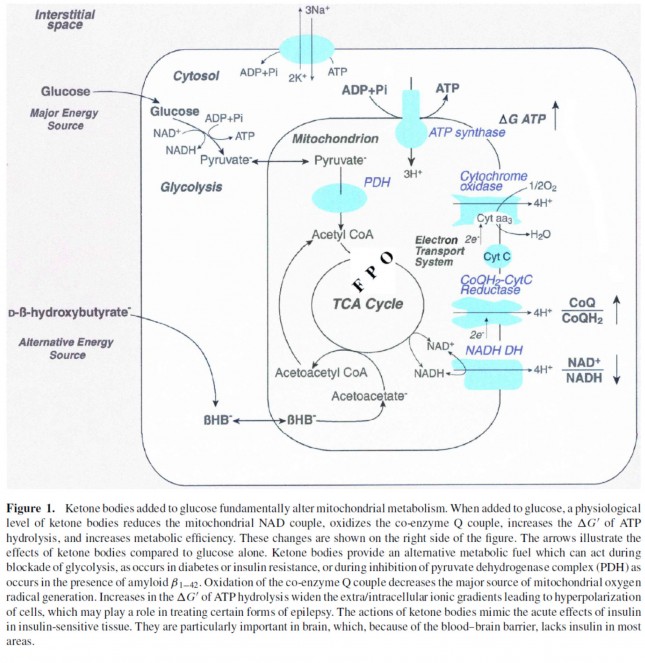
From the Figure 1 above, you can see that beta-hydroxybuterate [BHB (a ketone)] is converted to acetoacetyl CoA leading to the production of pyruvate, block-aiding additional glycolysis or inhibiting further glucose production at the liver level. Because the muscle tissues become more adept at using BHB, GLUT receptors are down-regulated at the muscle level as a person becomes more keto-adapted. Although we still have much to learn about the keto-adapted state, we know that this occurs more prominently in the muscle tissues than in the gut and brain. This fascinating glucose sparing phenomenon, has been interpreted by some as “worsening insulin resistance.”
Not to worry, glucose sparing is rapidly reversible and transitory within 1-3 days of increasing carbohydrate intake above 100-150 grams per day (1). It is also why those who become keto-adapted get a carbohydrate hangover including headache, stomach cramps, diarrhea, and malaise lasting 8-24 hours after cheating.
Is this bad? Absolutely not! It is NORMAL! (It’s just that most people, physicians included don’t know what the normal physiology of the Ketonian should look like.) Is it going to kill you, cause a stroke or give you a heart attack? Absolutely not. The elevated BHB actually increases production of adiponectin, leucine & glutathione that have antioxidant properties protecting one from transient inflammatory rises in blood sugar, enhancing insulin’s effect on the muscle, and preserving muscle mass while allowing for fat metabolism (4, 5, 6).
THE TAKE-HOME MESSAGE –
First, don’t cheat if you don’t want to see transient rises in blood sugar and experience the wonders of a carbohydrate hangover and some mild reactive hypoglycemia (low blood sugar) after the fact.
Second, if you’ve been in ketosis for longer than 3-4 months, and you absolutely must get another two or three hour oral glucose tolerance test (OGTT), you might want to increase your carbohydrate intake to 50-100 grams per day 1-3 days before the test to avoid an anomalous spike in blood glucose. (One OGTT was enough for me . . . but hey, some of us are gluttons for punishment.)
Third, enjoy your eggs, pass the bacon and stir me up some Keto//OS.

References:

Watch this weekend’s Periscope conversation about why weight loss is slow and why anything that is worthwhile takes time.
You can watch the Periscope Video below:
It has long been understood that tumor cells of any kind require high levels of glucose to grow and spread (1,2). It is also recognized that higher levels of insulin, commonly found in patients with insulin resistance or type II diabetes, are 2.4 times more likely to stimulate the development of breast cancer (3). A diet low in glucose has thereby been theorized to be an adjunct to cancer treatment.
Ketogenic diets have been demonstrated to be therapeutically useful in the treatments of epilepsy and cardiovascular disease (4). A ketogenic diet is one in which carbohydrate levels are kept below 50 grams per day and fat intake is increased to the point that the body shifts its metabolism to use triglycerides, and the ketones derived from triglycerides, as the primary fuel source for the majority of the cells within the body. With this understanding in mind, the application of a ketogenic diet, one high in fat and protein with limited carbohydrate or glucose has been suggested as a adjunct to cancer treatments (5).
A recent study (6) in the Oncology Letters evaluated the benefits of a ketogenic diet in 78 cancer patients in clinical practice. A novel marker measuring the tumor cells use of glucose called transketolase-like-1 (TKTL1) was closely monitored, as was each of the 78 patients adherence to a ketogenic diet. Increased TKTL1 was noted in more aggressively active and growing tumors (7,8).
Among the 43 males and 35 females, 7 patients agree to and followed a fully ketogenic diet and 6 of them followed a partially ketogenic diet. Ketogenic meals were provided by a German company called Tavarlin that would prepare and mail ketogenic meals including oil, fat, snacks, bread, protein and energy drinks. Dietary journals were reviewed every three months over a period of about 10 months.
40 % of these patients experienced a halting of the tumor progression and 60% experienced improvement noted by normalization of TKTL1 or reduction in TKTL1, respectively. Those on a ketogenic diet demonstrated an average reduction of TKTL1 by approximately 50%.
This is the first study of its kind and has significant potential. Could dietary carbohydrate restriction be an effective cancer treatment or adjunct to cancer treatment?
Because the food diaries were based on reporting only, the sample study was very small, and patients treated in the outpatient setting have the possibility of variability in the standard oncologic treatments, the results must be interpreted with caution. However, the data is very promising. This study is one in which I have great interest as I have seen similar results in my clinic on a case by case basis.
Based on the limitations noted above, rigorous randomized control studies are needed, but this is an exciting an promising first step. Additionally, the presence of a marker for tumor growth that correlates with diet is remarkable. And, it provides the ketogenic specialist a possible measurement tool that could be used clinically.
References:

The image above has nine dots within a square. Your task, using only four lines is to connect ALL nine dots WITHOUT ever raising your pen, pencil or finger (Please don’t use a sharpie on your computer screen . . . it doesn’t come off).
You may have seen this puzzle previously . . . it’s made its rounds in corporate training circles. But the underlying principle remains true. The solution requires you to expand your thinking or to “think outside the box.”
Whenever you find yourself on the side of the majority, it is time to pause and reflect. (Mark Twain)
Why should we limit ourselves to thinking outside the box. Can’t we just get rid of the box?
True discovery consists in seeing what everyone has seen . . . then, thinking what no one has thought.
The answer can be found when those four lines are used beyond the box our mind creates:

What good has the box done us? People were burned at the stake because they refused to believe the Earth was not the center of the universe. People were beheaded because they had a sneaking suspicion that the world was not flat.
Why is it so very hard to accept that our weight gain and diabetes are driven by a hormonal signal, and not by gluttony or caloric intake of fat? The definition of insanity is doing the same thing repetitively and expecting a different outcome. How long have you been restricting calories and fat with only minimal or no improvement in your weight, blood sugar, cholesterol or general feeling of health?
The main problem with the current thought model, or dogma, on the obesity’s cause is that it does not account for metabolic syndrome. Metabolic syndrome is insulin resistance. It is an over production of insulin in the presence of ANY form of carbohydrate (sugar or starch).
In the practice of medicine over the last 15 years, I noticed that a very interesting pattern emerged. There was always a spike in fasting and postprandial insulin levels 5-10 years prior to the first abnormal fasting and postprandial blood sugars. These patients were exercising regularly and eating a diet low in fat. But they saw continued weight gain and progressed down the path of metabolic syndrome. 10-15 years later, they fall into the classification of type II diabetes. What I now lovingly refer to as stage IV insulin resistance.
The only thing that seems to halt this progressive process with any degree of success is carbohydrate restriction. Fasting insulin levels return to normal, weight falls off, and the diseases of civilizations seem to disappear as insidiously as they arose.
So you tell me, is the world flat? Is the Earth the center of the universe?

What is a low carbohydrate or ketogenic diet? 15 years of practical in the trenches experience have helped me develop a very simple program to help you lose and maintain your weight. Access to this program, video help and access to blog articles at your fingertips are offered through my online membership site.
You can also hear me each week a I discuss low carbohydrate, paleolithic and ketogenic diets with the Legendary Jimmy Moore on KetoTalk.com

{kind=link}