As of late, Banner Health and Banner Community Integrated Network, in which I participate as a physician, is requiring that I recommend the COVID-19 vaccination to my patients. In order to be compliant with their requirement and my duty as a physician to “do no harm,” your understanding of the following data is necessary to give you a clear picture of the pros and cons to COVID-19 vaccination.
Please read, contemplate and sign this Informed Consent document before you receive any COVID-19 vaccination or booster. (A hardcopy of this informed consent is available in our office)
—————————————
You have asked for guidance in regards to the health risks and benefits of complying with COVID-19 mRNA experimental vaccination therapy required by your institution or place of employment. Although this medical intervention and injection does not meet the traditional definition of a vaccine defined by the CDC and published on their website in 2012 (the CDC changed the definition of “vaccine” in 2021 to fit this therapy), the term vaccine will be employed for ease of use in the below.
Note that the long-held (but presently ignored) standard for informed consent requires that I fully disclose the current and accurate data regarding all potential risks, benefits, and alternatives to COVID mRNA vaccination. Note that my interpretation of the below data was done consistent with the long-held (but pandemic-ignored) Federal regulatory standard that considers any adverse event or death reported in temporal association with receipt of a novel and/or experimental therapy to be caused by the intervention until proven otherwise. I recognize this practice departs from the recently adopted, ethically and morally troubling pandemic standard whereby U.S Federal and State Health Agencies’ and hospital systems dismiss adverse event reports as unrelated to the vaccines until proven otherwise.
In the following, I will provide documentation of the informed consent discussion I hold regarding a decision on whether to pursue COVID-19 mRNA vaccination. In the following, I solely rely on the most current, available data regarding:
1) Risks associated with receipt of a COVID mRNA vaccination
2) Efficacy of the COVID-19 mRNA vaccine in preventing illness
2) Efficacy of the COVID-19 mRNA vaccine in preventing transmission
3) Efficacy of the COVID-19 mRNA vaccine in preventing hospitalizations and death
4) Efficacy of the COVID-19 mRNA vaccine compared to the protection offered by natural immunity
5) Efficacy of the COVID-19 mRNA vaccine in the prevention of “long-haul” COVID
6) Risks of a healthy child suffering hospitalization and/or death from COVID
7) Efficacy and safety of alternatives to vaccination (i.e. reliance on effective early, anti-viral, and anti-inflammatory combination therapy)
As is standard in informed consent discussions, I first begin with a review of the risks of COVID-19 mRNA vaccination.
1) RISKS ASSOCIATED WITH RECEIVING THE COVID mRNA VACCINE
Based on the below data compiled from peer-reviewed papers, Life Insurance Industry reports, and analyses of the Vaccine Adverse Event Reporting System (VAERS) database, it is my conclusion that a literal humanitarian catastrophe is rolling forward. This resulted from the rapid deployment of barely-tested mRNA vaccines in an illogical attempt to counter a fast-mutating coronavirus. I acknowledge that this assessment contradicts current “medical consensus,” which is that the vaccines are “safe and effective” and that vaccinating against a coronavirus is the dominant public health strategy across much of the world. There are a few reasons which may explain the discord between my personal recommendations and those of health agencies across numerous advanced health economies like the United States.
There is great dissymmetry between the data that I have spent thousands of hours reading over the last two years (many thanks to the painstaking efforts of Dr. Pierre Kori to compile this data here) and analyzed compared to the selective and near uniformly favorable data being disseminated across media, social media, and numerous high-impact scientific journals. One explanation for this discord can be found in recent FOIA-obtained evidence which revealed that $1 billion dollars was paid by the Department of Health and Human Services to U.S media companies to (blindly) support a media campaign to build public confidence in and uptake of COVID-19 mRNA vaccines.
A second contributing factor to the lack of scientific recognition of this catastrophe is that as of this writing, although over 1,650 case reports and small cases series of adverse events have been published in the medical literature, review papers reporting summary analyses of either the toxicity or poor real-world efficacy of the vaccines have been consistently rejected upon submission to medical journals, particularly high-impact ones. In addition to the rejecting of such studies, a number of journals have also illegitimately retracted papers that reported on the scale of adverse events despite those papers having successfully passed expert peer-review. The few published, peer-reviewed summary analyses that reported on either a lack of efficacy or on the excessive risks of the vaccines have generally appeared in lower impact journals that are systematically ignored by media outlets and academia. These have been included below.
In the setting of such widespread media, social media, and scientific journal propaganda/censorship of adverse vaccine data, the following information is unlikely to be known by the average citizen or physician in the United States. I invite any who want to challenge or validate these interpretations and conclusions to more deeply explore the underlying data sources using the hyperlinked references below.
Peer-Reviewed Literature
In this published paper analyzing data from the pivotal clinical trials used to support the novel mRNA vaccines (i.e. Moderna, Pfizer, and Janssen), Classen compared “all cause severe morbidity,” defined as “severe infections with COVID-19 and all other severe adverse events between the treatment arms and control arms respectively.” His analysis found a statically significant increase in all cause severe morbidity occurred in the vaccinated group compared to the placebo group.
In this paper by Walach et al, they calculated the Number Needed to Vaccinate (NNTV) to prevent one death from a large Israeli field study. They then accessed the Adverse Drug Reactions database of the Dutch National Register (Lareb) to extract the number of cases reporting severe side-effects and the number of cases reporting fatal side-effects.
- They found the NNTV to be between 200 and 700to prevent one case of COVID-19 by Pfizer’s mRNA vaccine product.
- The NNTV to prevent one death was between 9,000 and 100,000 (95% confidence interval), with 16,000 as a point estimate(as you will see below, for younger healthy people, this estimate would tend to the higher end of a NNTV of 90,000-100,000 to prevent a single death).
- They calculated that for every 6 deaths prevented by vaccination, there were approximately 4 deaths reported associated with vaccination, yielding a potential risk/benefit ratio of 2:3 (note that deaths are consistently under-reported to such databases, thus a more accurate risk/benefit ratio for death would likely be inverted).
- They concluded that, “although causality between individual reports of adverse events and vaccination has not been established, these data indicate a lack of clear benefit, which should cause governments to rethink their vaccination policy”.
In this published paper by Jessica Rose, a world-expert analyst of the VAERS database, she found that, based on the ratio of expected severe adverse events to observed adverse events in VAERS for a number of conditions, the “underreporting factor (URF)” for COVID vaccine-associated deaths was 31. Using this URF for all VAERS-classified severe adverse events, as of October 2021, vaccines were associated with 205,809 deaths, 818,462 hospitalizations, 1,830,891 ER visits, 230,113 life-threatening events, 212,691 disabled and 7,998 birth defects.”
This paper by Ronald Kostoff et al was retracted despite passing peer-review. However, in a personal review of the correspondence between the author and Journal Editor, neither I nor my colleagues were able to find a valid criticism of the underlying data analysis or conclusions. Therefore, I have incorporated this valuable study whereby they used a novel, best-case scenario, cost-benefit analysis which showed conservatively that there were five times the number of deaths attributable to each inoculation vs. those attributable to COVID-19 in the most vulnerable 65+ demographic. The risk of death from COVID-19 decreased drastically as age decreases, and the longer-term effects of the inoculations on lower age groups “may increase” their risk-benefit ratio (although this has not been demonstrated to date as can be seen below).
VAERS Data
As of April 22, 2022, in the United States alone 5,309 cases of myocarditis, 782,665 adverse events, 151,796 severe adverse events, and 14,613 deaths have been recorded in the Vaccine Adverse Event Reporting System following COVID-19 vaccination in the USA. It should be appreciated that the VAERS database’s main limitation is that of underreporting, by a factor of at least 30-fold. The most concerning implication of under-reporting is in regards to the exponential increases in actual reports of death after vaccination in the past year compared to prior years of all vaccines combined.

Even more damning is the temporal relationship of these reports to the date of the individual’s vaccination, which some authorities have attempted to dismiss as simply representing “background” deaths. The fact that the reporting of deaths decrease over time from date of vaccination (seen below), infers a worrying causal relationship whereas erroneously reported “background deaths” would instead appear in similar numbers each subsequent day after the date of vaccination.

Statisticians and analysts working with the Vaccine Safety Research Foundation (VSRF) have estimated the total number of deaths in the U.S caused by the COVID-19 vaccines based on the numbers reported to the U.S Vaccine Adverse Event Reporting System. In their white paper, they employed 9 different statistical prediction models and found that as of December of 2021, total deaths associated with the vaccines ranged from 148,000 to 216,000. Using the same methodology for the 14,613 COVID-19 vaccine associated deaths in the U.S reported as of May 16, 2022, the updated point estimate is approximately 599,000 deaths. The data and conclusions from these publications above provide support for identifying the vaccination campaign as the primary cause of the massive increases in Life Insurance claims among working-age Americans beginning in the second half of 2021, as will be detailed below.
Life Insurance Industry Data
Most concerning is a recent report of a large, unexplained rise in U.S life insurance claims amongst working age Americans of ages 18-64 beginning in early to mid-2021, timed with the vaccination campaign rollout. In a press conference, the CEO of One America, the $100 billion Life Insurance giant, publicly stated;
- “what we saw just in third quarter, we’re seeing it continue into fourth quarter, is that death rates are up 40% over what they were pre-pandemic.”
- “deaths in this age group is 4 times higherthan what would be seen in a “one-in-200-year catastrophe,” and that, “40% is just unheard of.”
- “every single other insurance company has also reported seeing the same – what’s most worrisome though, is that the biggest increase in excess deaths has come from traditionally healthier working-aged individuals under 65 – and not the elderly, who are the most susceptible to the Covid-19 virus.”
- “we are seeing, right now, the highest death rates we have seen in the history of this business – [and] not just at OneAmerica, the data is consistent across every player in that business.”
Financial analyst and former Blackrock Managing Director, Edward Dowd, reported similar historic increases in death claims over the same time period from discussions with major U.S life insurance industry executives; 57% for Lincoln National, 41% for Prudential, 32% for Hartford, 24% for MetLife and 21% for RGA.
In line with these data, a publicly available quarterly report by the Group Life Insurance Industry, covering roughly 90% of the employer-based policies, reported on Page 23 that younger age groups were suddenly dying at historically unprecedented rates beginning in Q3 of 2021.
The timing and magnitude of the historic rise in death and disability are also seen in German health insurance claims data and Medicare billing data.
Epidemiologic Data
An article published in the journal Nature reported:
- increases of over 25% in the number of ambulance calls in response to cardiac arrests (CA) and acute coronary syndromes (ACS or “heart attacks”) for young people people in the 16–39 age group during the COVID-19 vaccination rollout in Israel (January–May, 2021) compared with the same period of time in prior years (2019 and 2020).
- a robust and statistically significant association between the weekly CA and ACS call counts and the rates of 1st and 2nd vaccine doses administeredto this age group. Note they found no observed statistically significant association between COVID-19 infection rates and the CA and ACS call counts.
- findings that aligned with previous studies showing that increases in overall CA incidence were not always associated with higher COVID-19 infections rates at a population level, and that the stability of hospitalization rates related to myocardial infarction throughout the initial COVID-19 wave compared to pre-pandemic baselines in Israel.
- findings that mirrored reports of increased emergency department visits with cardiovascular complaints during the vaccination rollout in Germany as well as increased EMS calls for cardiac incidents in Scotland.
In line with the above, as a result of a FOIA application in the state of Massachusetts, an analysis of the now publicly available death certificate data found that during 2020, the predominant cause of rises in all cause mortality were due to “respiratory causes,” (i.e. excess mortality from COVID-19) while in 2021, the predominant causes were “cardiovascular.” The analyst concluded, “the official Massachusetts database of death certificates contains proof that C19 vaccines killed thousands of people in Massachusetts in 2021.”
Equally alarming are the massive rise in deaths among healthy, young professional athletes from around the world. Since the vaccination campaign was initiated, and as of June 4, 2022, there were approximately 1,090 athletes that suffered a cardiac arrest, with 715 of them dying as a result. The majority of arrests occurred in competition or training. The frequency of these events in comparison to historical data is highly concerning. In a 2009 review of professional athletes deaths, published in a prominent European Cardiology journal, they found that from 1966 to 2004, there was an average of only 29 sudden athlete deaths per year worldwide. Compare this number to just the month of January 2022 alone where 127 collapses and 87 deaths among professional athletes were reported. Overall, these athlete deaths reflect an approximately 22-fold increase in the year after the introduction of COVID vaccines, to date unexplained by other identifiable causes.
On March 10, attorney Matt Staver of Liberty Counsel presented data in court showing 127 VAERS-reported COVID vaccine-related deaths in the military in 2021. That is more than the 93 reported COVID deaths in the military since the beginning of the pandemic. Note that COVID deaths tend to be overestimated, while VAERS-reported deaths, especially in the military, are severely underreported.
The CDC data provided in this article shows the timing of the start and the steady rise in all-cause mortality of working-age adults in the U.S, both overlapping with the start of the mass vaccination campaign. Although alternate causes of this historic rise in death have been considered, (i.e. COVID deaths, deaths of despair etc), the number of deaths from these causes is insufficient to explain the overall rise.
Rises in Disability
Associated with the massive rises in death claims are disability claims. The Bureau of Labor Statistics (BLS) surveys 60k households monthly to estimate the unemployment rate, and in this survey, asks households about disabilities as well. From the BLS data, for Americans over the age of 16:
* After declining in 2020 (and stable for five years prior), in Dec 2020 there were 29.9 million Americans disabled. This is a disability rate of 11.4%.
* At year end 2021, there were 32.4 million Americans disabled. This is an increase of 2.5 million people and a disability rate of 12.4%. This is a record number and record percentage rate.
* As of May 2022 there were 32.7 million Americans disabled. This is an increase of 2.9 million people since Dec 2020, the start of mass vaccinations. This is again a record number and percentage rate.
If you look at the charts below you can see that 1.8 million of the increase came in spring 2021 with another increase in fall 2021. Given the strong overlap with the broad vaccination campaign in spring of 2021 followed by vaccine mandates in fall of 2021, it is consistent with the vaccine injury hypothesis as detailed in the data above.


In particular, the increase of 2.9 million disabled since December of 2020 represents more than 1% of the 263 million Americans over age 16. These Americans were all newly disabled in 2021 from some injurious societal or environmental development or exposure beginning in 2021, and not in 2020. It should be noted that these data reflect only a portion of the extent of injuries occurring given that it is likely that far more Americans suffered less debilitating adverse consequences.
On Feb. 10, the Israeli Health Ministry published the results of a survey of adverse events among roughly 2,000 random Israelis who received booster shots. Although many could be thought of as minor, it is concerning that 51% of the women and 35% of the men who experienced a side effect reported that, as a result, they had difficulty performing daily activities. A total of 4.5% of those who received booster doses reported neurological side effects.
Further, in the documents related to a recent FOIA request, in the Pfizer informed consent document (p. 5) it was revealed that the company recognized the risk of myocarditis to be as high as 1 in 1,000. In 2022, with many fewer vaccines administered compared to 2021, the rate of myocarditis reports to VAERS is averaging 245% higher than last year. The myocarditis is overwhelmingly found in young adults like Grace.
In addition, military whistleblowers leaked data from a Department of Defense database, showing major increases in a large number of diagnoses in 2021 compared to the stable average over the years 2016-2020. They found that in 2021, among military service members, there was a 988% increase in all diseases and injuries, a 218% increase in cancer diagnoses, a 374% increase in female infertility, 221% increase in dysmenorrhea, and a 183% increase in spontaneous abortions, with these latter findings of great concern to the future reproductive health of a young woman like Grace. Later claims by the Department of Defense that the prior year illness frequencies were erroneous and caused by “data corruption during a server migration” is simply not credible given this supposed error was “corrected” only after the whistleblowers reported. Further, these morbidity increases are consistent with all the other data sources presented above.
2) EFFICACY IN PREVENTION OF COVID-19
Using up-to-date data (i.e. last 3-6 months to today) from a wide selection of public health sources including the U.S, Denmark, Israel, Australia, and the UK, the current estimate of the protective efficacy from contracting COVID is one of either “negative efficacy” or rapidly waning efficacy such that potential benefits, if any, are demonstrably short-lived. Further, given the above alarming estimates of the real-world risks of the vaccines, the information below is focused on the most conservative data estimates of efficacy to determine “the minimum of what COVID-19 vaccinations can achieve.” This is base on the fact that you have both natural immunity and a good health status.
It must be acknowledged that accurately interpreting epidiomiologic data to determine the relationship between vaccination status and the risk of contracting COVID is both challenging and complicated given:
1) the unmeasured confounding variables associated with an individual’s vaccination status (i.e. age, co-morbidities, behaviors)
2) the rapidly changing and often inconsistent definitions of what it means to be vaccinated (dependent upon varying numbers of vaccinations during different periods, varied vaccine types and schedules, and varied time windows from last vaccination).
3) the definition of a COVID case (tested, untested, false positive, false negative), the definition of a COVID death (“with COVID” vs. “from COVID,” with the latter likely overestimated due to hospital financial incentives created during the Pandemic).
4) the exclusion from efficacy calculations of the surprisingly large numbers of COVID infections and deaths suffered by the recently vaccinated (i.e. within 14 days of vaccination).
With the above caveats in mind, the best assessment of the below data indicate that vaccinated individuals are more likely to fall ill with the variants now in circulation. This may not have been the case earlier in the global vaccination campaign but is unfortunately the case now. There are several possible explanations for this finding. Chief among them is that the current mRNA vaccines were formulated using the genetic sequences of the original “Wuhan” strain of SARS-CoV2 from over 2 years ago. Given SARS-CoV2 is a highly mutagenic virus, many dozens of variants have since emerged, with several strains exhibiting sudden, multiple, and major pathogenically important mutations, particularly within the original spike protein to which the mRNA sequences are directed.
The major mutations have been “named” and each have many subvariants. The Delta variant phase in the U.S ran from approximately June of 2021 to January 2022, after which the Omicron variant has predominated, and we are currently seeing rising cases from sub-variants of this strain. Omicron deserves mention as it is phylogenetically different from both Delta and the original Wuhan strain. This is likely the most accurate explanation as to why, in the setting of what are now “non-neutralizing” antibodies, this paradoxically makes “Wuhan strain” vaccinated individuals more susceptible as follows;
Stanford researchers found that “prior vaccination with Wuhan-Hu-1-like antigens followed by infection with Alpha or Delta variants gives rise to plasma antibody responses with apparent Wuhan-Hu-1-specific imprinting manifesting as relatively decreased responses to the variant virus epitopes compared with unvaccinated patients infected with those variant viruses.”
From a Public Health England vaccine surveillance report in the U.K., government researchers asserted (p. 23) that their serology tests were underestimating the number of people with prior infection due to recent observations from UK Health Security Agency (UKHSA) surveillance data that “N antibody levels appear to be lower in individuals who acquire infection following 2 doses of vaccination.”
Dr. Paul Offit, Chair of the FDA Vaccine Advisory Board conceded in a letter to the New England Journal of Medicine that there is a real concern of the shots inducing a form of immune suppression known as original antigenic sin.
In this peer-reviewed paper, “Increases in COVID-19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States,” they found that at the country-level (and U.S county level), there appears to be no discernable relationship between the percentage of the population fully vaccinated and new COVID-19 cases as seen below. In fact, the rising slope of the relationship in both graphs below suggest that mass vaccination policies may paradoxically lead to more cases, with Israel serving as a worrying outlier.

A study prepared by Humetrix for the Department of Defense called “Project Salus,” monitored 20 million Medicare beneficiaries from January to August of 2021 and found that the vaccinated share of the COVID hospitalizations rose steadily with both vaccines after three to four months and sharply after six months (as the Israelis found). By late July, 71% of all cases and 61% of all hospitalizations were among vaccinated individuals.
More current data from the Walgreens chain of pharmacies finds that in the U.S, over the last several months, fully or partially vaccinated individuals are testing positive at higher relative rates than the unvaccinated.
According to Cornell University’s faculty, an outbreak in December of 2021 which forced the school to switch to online learning was driven exclusively by the vaccinated. “Virtually every case of the Omicron variant to date has been found in fully vaccinated students, a portion of whom had also received a booster shot,” said Vice President for University Relations Joel Malina in a statement.
On December 31, 2021, the UK’s Office of National Statistics released an “Infection Survey” of 1,701 individuals who tested positive for COVID between Nov. 29 and Dec. 12, of whom 115 tested positive for the Omicron variant. The agency found a clear correlation between the number of vaccinations and the likelihood of an Omicron-positive result. The odds ratio of testing positive for Omicron with two vaccinations was 2.26; for the triple-vaccinated, it was 4.45.
According to the latest U.K. health surveillance report, roughly 95% of those over 70 are double-vaccinated and about 90%-93% of the age cohorts over 70 are boosted. Just 1.6% of the senior cases between weeks 7 and 10 of this year were among the unvaccinated, which is below the 5% share of the population they compose. The triple-boosted actually made up 90% of the cases.

The respected Robert Koch Institute reported that among the 4,206 Germans infected with Omicron for whom their vaccination status was known, 95.58% were fully vaccinated. More than a quarter of them had booster shots. Given that the overall background rate for vaccination in Germany is 70%, this suggests an -87% effectiveness rate against Omicron.
As of Dec. 31, 2021, in Denmark, 89.7% of all Omicron cases were among the fully vaccinated with just 8.5% of all cases in Denmark among the unvaccinated, according to the Statens Serum Institut. Overall, 77.9% of Denmark was fully vaccinated at the time, and Omicron is more prevalent among younger people for whom there is a greater unvaccinated pool, which again support a negative efficacy. Even for non-Omicron variants, the unvaccinated composed only 23.7% of the cases.

As mentioned above, assessing the true relationship between vaccinations and the risk of infection must also consider the shocking numbers of COVID infections and deaths occurring during the first 14 days after vaccination. The argument to include these data is supported by the biological plausibility based on the studies presented above finding that the outdated vaccines are inducing an immune suppression favoring infection with newer variants. It is my opinion that these cases and deaths should not be excluded given the below examples (there are many more) of record rises in cases (and deaths) proximate to the start dates of various country-wide vaccination rollouts.


The examples below include countries that initiated the most aggressive mass vaccination campaigns in the period from late December, 2020 to January, 2021. Note these countries are from different regions of the globe, however the rollouts were all followed by large increases in cases and deaths.





3) EFFICACY IN PROTECTION FROM SEVERE DISEASE
In Ireland, in March of 2022, during the milder Omicron variant wave, there were more people in Irish hospitals than at any point in the previous 12 months. This occurred despite the fact that nearly 95% of all adults in Ireland are fully vaccinated, and nearly 100% of seniors are vaccinated and boosted.
In Scotland, on page 29 of their recent national COVID-19 report, the data revealed that the vaccinated were dying and being hospitalized at higher rates than the unvaccinated. Note that Scotland has since made the decision to no longer publish these comparative data for “concerns that they are being misinterpreted”. Although it is true, as was noted above, that numerous variables beyond vaccination status may contribute to explaining these differences, it is troubling (similar to the Department of Defense actions mentioned above) that the decision to stop publishing these data occurred only after a negative efficacy against severe disease and death was found.
In Israel, the Director of a major hospital recently declared that the fully vaccinated are not protected against severe illness.
NSW Health in New South Wales, the most populated of Australian states at 8.1 million inhabitants, reported that 97 out of 98 COVID-19 deaths occurring over the previous two weeks involved fully vaccinated persons. Moreover, those that had three doses appeared most at risk for hospitalization admission, ICU transfer, and death.
These data are consistent with the recent report published in the New York Times which stated “despite strong levels of vaccination among older people, COVID killed them at vastly higher rates during this winter’s Omicron wave than did last year, preying on long delays since their last shots and the variant’s ability to skirt immune defenses.” These higher rates of death in the elderly are also seen in the boosted.
The conclusion of a recent Danish study in the prestigious Lancet found that in long-term follow-up of over 74,000 adult participants in the Moderna and Pfizer trials there was no all-cause mortality benefit from the two mRNA shots.
In a recent, large Veterans Administration study, investigators discovered disturbing evidence: by month six after a SARS-CoV-2 infection, beyond the first 30 days of illness, vaccinated persons with breakthrough infections were at higher risk of death (hazard ratio (HR) = 1.75, 95% confidence interval: 1.59,1.93).
The implications of the vaccine’s diminished ability to protect against severe disease among more recent variants is now playing out in real-time. On June 5th, 2022, analyst Igor Chudov posted a 2 country comparison of the current cases and deaths being reported from Portugal and S. Africa, two countries undergoing similar waves of infection from the emerging B4/5 sister variants. South Africa is only 35% vaccinated and 5% boosted whereas Portugal is 95% vaccinated and 70% boosted. These variants are now driving a deadly wave of Covid in highly-vaccinated Portugal, with deaths among the Portuguese nearing their January peak and still rising as seen below.


Thus, in terms of benefits, based on the most up-to-date data, the current crop of mRNA vaccines against Omicron confer either rapidly waning efficacy or negative efficacy, and not only do they no longer protect against severe disease, they appear to be raising the risk of severe disease and death.
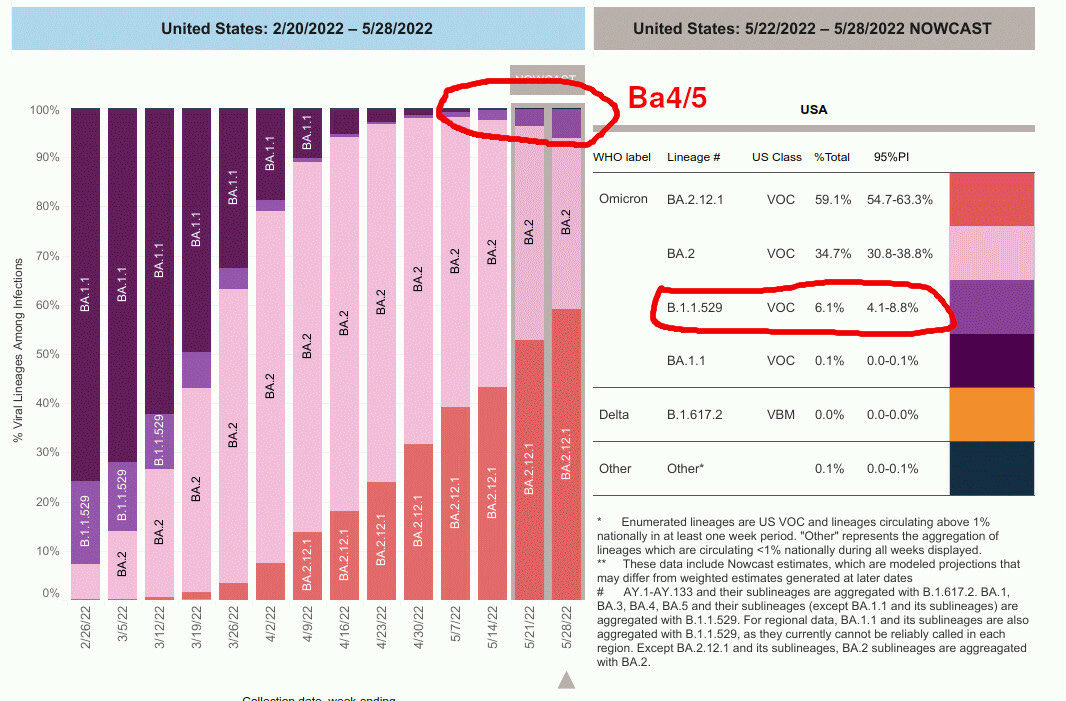
I, therefore, would advise extreme caution given that, currently, in the U.S, the prevalence of the B4/5 variant appears to be doubling every week in the past month, now comprising approximately 8% of cases.
4) BENEFITS IN REDUCING TRANSMISSION TO OTHERS
Current data do not support this claim. The CDC Director herself has reported that vaccinated individuals are now well known to carry equal or greater viral loads than the unvaccinated, and thus transmit at equal or higher rates, for physiologic reasons detailed above, most concerning being the negative efficacy of the vaccines against Omicron. This has also been reported by seminal nosocomial outbreak papers by Chau et al. (Health care workers (HCW) in Vietnam), the Finland hospital outbreak (spread among HCWs and patients), and the Israel hospital outbreak (spread among HCWs and patients).
A new large study from Quatar in the New England Journal of Medicine by Weil Cornell Medicine found that the Pfizer vaccine protection waned after four months. By seven months, when adjusted for those who already had prior infection, the Pfizer shot was -4% effective against transmission. Also, effectiveness against asymptomatic infection was -33% after seven months, which suggests that the vaccinated become more likely to spread COVID-19 over time.
5) BENEFITS IN REDUCING THE RISK OF LONG-HAUL COVID SYNDROME
Again, from the large Veterans Administration study, investigators discovered disturbing evidence: by month six after a SARS-CoV-2 infection, vaccinated persons with breakthrough infections were at higher risk of long COVID (HR = 1.50, 95% CI: 1.46, 1.54). When including the earlier time periods, the COVID-19 vaccines only reduced the risk of long COVID by approximately 15% compared to the unvaccinated, a level of estimated protection far less than the increased risk of death found in the same study as mentioned above.
6) BENEFITS OF NATURAL IMMUNITY
Natural immunity provides robust protection, not only from contracting the COVID-19 a second time, but also against hospitalization and death.
The most recent review of data supporting the protection of natural immunity, compiled from over 150 research studies, found that natural immunity provided equal or superior protection against not only contracting the disease, but also against hospitalization and death.
Further, vaccinated individuals are far more likely to get re-infected with COVID compared to those with natural immunity. A new preprint study from Bangladesh found that among 404 people re-infected with COVID, having been vaccinated made someone 2.45 times more likely to get re-infected with a mild infection, 16.1 times more likely to get a moderate infection, and 3.9 times more likely to be re-infected severely, relative to someone with prior infection who was not vaccinated. Although overall re-infections were rare, vaccination was a greater risk factor of re-infection than co-morbidities.
A new study from Harvard, Continued Effectiveness of COVID-19 Vaccination among Urban Healthcare Workers during Delta Variant Predominance, tracked vaccinated and unvaccinated Massachusetts healthcare workers and showed 0 infections in 74,557 person-days for previously infected patients compared to 49 infections out of 830,084 person-days for fully vaccinated patients.
A study published in the New England Journal of Medicine assessed a cohort of 1,304 patients meeting a very strict definition of “re-infection.” In this cohort, there were no deaths and no ICU admissions during reinfections while 7 deaths and 28 ICU admissions occurred during the primary infections. Overall, there was a statistically significant 90% reduction in the composite outcome of severe, critical, or fatal disease during reinfections
7) BENEFITS OF CURRENT HEALTH STATUS
Those persons of normal body weight and under age 21 youth with an absence of co-morbidities have essentially a near-nil risk of a severe outcome.
This data is based this on data compiled during a prior, more deadly variant where the CDC published a report on the incidence of death from COVID-19 prior to September of 2021 in people less than 21 years of age. At the time of that report, 190,000 deaths from SARS-CoV-2 had been recorded in the general population. Although people less than 21 years of age represent 26% of the population, only 0.08% (121) of all COVID-19 deaths were reported in this age group. In other words, more children died from influenza during the previous epidemic season than from SARS-CoV-2.
Several other observations were of interest:
- 75% of those under 21 who died had at least one underlying medical condition; 45% had two or more conditions.
- Minority groups were disproportionately represented among the deaths in young people. Among those who died, 45% were Hispanic, 29% were black, and 4% were American Indian or Alaskan Native persons. Although Hispanic, Black and Native populations represent 41% of the U.S. population less than 21 years of age, these groups accounted for 75% of the deaths.
In July of 2021, Dr. Marty Makary of Johns Hopkins University and Editor in Chief of MedPage today, reported that over the course of the pandemic, 49,000 Americans under the age of 18 had died of all causes, according to the CDC. Only 331 of those deaths were from COVID — less than half as many as that died of pneumonia. The risk of children was dramatically smaller still than that CDC baseline; according to one, much-cited paper, the infection fatality rate for those aged 5 to 9 is less than 0.001 percent. A large new study from the U.K. examining the fatality rate among all those under 18 found it only fractionally higher there — 0.005 percent. Overall, 126,000 Brits have died of COVID since the onset of the pandemic; just 26 of those were under the age of 18.
These data presented above must be further interpreted in the context of the current Omicron variant, a variant with markedly lower risk of leading to hospitalization and and/or death among the unvaccinated.
8) ALTERNATIVES TO VACCINATION: EARLY TREATMENT OF COVID-19
The alternative to vaccination would be to ensure provision of early treatment with a select combination from what are now dozens of medicines, nutraceuticals, and therapies with proven efficacy in COVID-19. I am willing to prescribe the medicines that cannot be obtained over-the-counter, however, I must emphasize the need to have this treatment upon first symptoms of any viral syndrome like illness. The importance of early treatment can be seen in the graph below, showing diminishing efficacy of treatment with each day of delay. Note the near 100% efficacy if treatment is started within 24 hours of symptoms.

As of May 2022, massive evidence bases support numerous generic, repurposed drugs with excellent safety profiles that act with either anti-viral, anti-inflammatory, or immunomodulatory properties have been compiled. The medicines shown effective can be seen below. I have circled only those medicines that have received Emergency Use Authorization status by the FDA or recommended by the NIH. Note that these “officially approved” medicines consist solely of novel pharmaceutical industry products that can generate massive profits, an obvious feature of our health care system in the United States. Off-patent, generic or over the counter therapies are not recommended, despite often higher amounts of trials evidence for their use. Note that the grey font indicates medicines with less than 5 trials to support.

Ivermectin has the highest potency amongst the medicines sufficiently studied. Ivermectin’s evidence base now consists of 84 controlled trials, 34 of them randomized, and include a total of 129,000 patients. Summary analyses of the data from these trials find large, statistically significant reductions in time to clinical recovery, time to viral clearance, hospitalizations, and death as seen on the right of the below graphic.

Similarly, hydroxychloroquine has 347 controlled trials which involve almost a half-million patients. The studies show consistent, reproducible reductions in the incidence of all outcomes, particularly when given early, similar to ivermectin.

Nigella Sativa, a widely available “nutraceutical” used in many countries around the world, has also shown repeated, high efficacy as below.

Numerous other medications and compounds have demonstrated efficacy, such as the use of povidone-iodine nasal drops and mouthwashes, as well as medications like fluvoxamine.
The protocol I use can be obtained by calling my office and scheduling an appointment with me or my Nurse Practitioner.
Summary and Recommendations.
In summary, those patients with a good health status, normal body habitus, and natural immunity to COVID, have a near-nil risk of the most severe outcomes from COVID.
Risks of Long haul or prolonged illness would be further reduced with adoption of almost any early treatment strategy. Further, the totality of current evidence finds either a rapidly waning efficacy in protection against COVID-19 or a rising negative efficacy in protection from both COVID and its more severe outcomes.
Finally, given the highly concerning, excessive rates of adverse events, disabilities, and deaths found in the vaccine trials data and in association with the mass vaccination campaign, it is my professional opinion that the risks of COVID-19 mRNA vaccination for most people, except those over 80 years old with comorbidities, far outweigh the negligible or “adverse” efficacy currently being measured.
Please sign and date below that you have read and understand the risks and benefits of COVID-19 vaccination as it stands to date.
_____________________________________________ ___________________________
Name Date






 Comparison of:
Comparison of:











{kind=link}