One of the common complaints that I see in my office is chronic numbness and tingling of the hands, fingers, feet & toes. There are multiple causes of these symptoms, but by far the most common cause in my practice is polyneuropathy caused by insulin resistance (hyperinsulinemia).
Before we dive into this particular type of nephropathy, it is important that we define a few terms. The terms “polyneuropathy,” “peripheral neuropathy,” and “neuropathy” are frequently used interchangeably, and although they can be easily confused, they are distinctly different.
Definitions
- Polyneuropathy is a specific term that refers to a generalized sensation of tingling or numbness that uniformly affects many nerves at the peripheral sites (ends of the extremities like hands, fingers, lower legs, feet and toes).
- Peripheral neuropathy is a less precise term. It is frequently used synonymously with polyneuropathy, but can also refer to any disorder of the peripheral nervous system. However, this term includes pain or numbness that radiates from nerve roots like “sciatica” of the leg and “brachial plexopathy” causing symptoms in one hand and/or arm (mononeuropathies).
- Neuropathy, which again is frequently used interchangeably with peripheral neuropathy and/or polyneuropathy, can refer even more generally to disorders of the central (brain & spinal cord) and peripheral nervous system (nerves of the arms and legs) and their connections to sensory organs, such as the eye and ear, and to other organs of the body, muscles, blood vessels, and glands.
Why spend time defining all this? Because, neuropathy can be very confusing, even for the experienced physician. And, because I am seeing, more and more frequently, cases of insulin resistance induced polyneuropathy. The polyneuropathies must be distinguished from other diseases of the peripheral nervous system, including the mononeuropathies and mononeuropathy multiplex (multifocal neuropathy), and from disorders of the central nervous system.
- Mononeuropathy refers to focused involvement of a single nerve, usually due to a localized trauma, compression, or nerve entrapment. Carpal tunnel syndrome is a common example of a mononeuropathy. Sciatica due to a lumbar disc bulge is another form of mononeuropathy.
- Mononeuropathy multiplex refers to simultaneous involvement of non-adjoining sections of nerve trunks. Used loosely, this term can refer to multiple compressive mononeuropathies. However, in its more specific meaning, it identifies trauma, infection, auto-immunity or damage to multiple nerves outside the central nervous system. This is often due to lack of blood supply due to disease based inflammation of blood vessels supplying blood to these peripheral nerves.
- Diseases of the central nervous system such as a brain tumor, stroke, or spinal cord lesion occasionally present with symptoms that are difficult to distinguish from polyneuropathy.
Insulin Resistance and Neuropathy
Insulin resistance, or better defined hyperinsulinemia, begins 10-15 years before a person is considered “pre-diabetic” and 20 years before the onset of type II diabetes. This “over production of insulin” in response to carbohydrates, starches and sugars causes a subtle and progressive form of inflammation. This excessive production of insulin will damage the smallest arteries (capillaries) carrying oxygen and fuel to the back of the eyes, the kidneys and the peripheral nerves of the hands, fingers, lower legs, feet and toes.
Often not identified until a person is actually diabetic, the mechanism underlying the development of this type of neuropathy is extremely complex. It is driven by years of subtle and progressive damage to the blood vessels, and inability of the nerves to use essential B vitamins damaging the genetics of the cell. This leads to inflammatory, metabolic, and ischemic effects causing the nerves to function poorly over time.
What Causes Polyneuropathy?

The mechanism of polyneuropathy damage in the patient with hyperinsulinemia three-fold.
-
- The presence of high insulin stimulates increased fat storage. As fat cells begin to get filled, they begin to over-produce a number of inflammatory hormones including TNF-alpha, IL-6, IL-1, Adiponectin, Leptin and Resistin. These inflammatory hormones turn on auto-immunities and abnormal immune system function.
- At the same time, the high insulin levels suppress appropriate testosterone and estrogen production causing microscopic damage to the lining of the smallest arteries and capillaries of the body (found predominantly at the extremities, kidneys and back of the eyes).
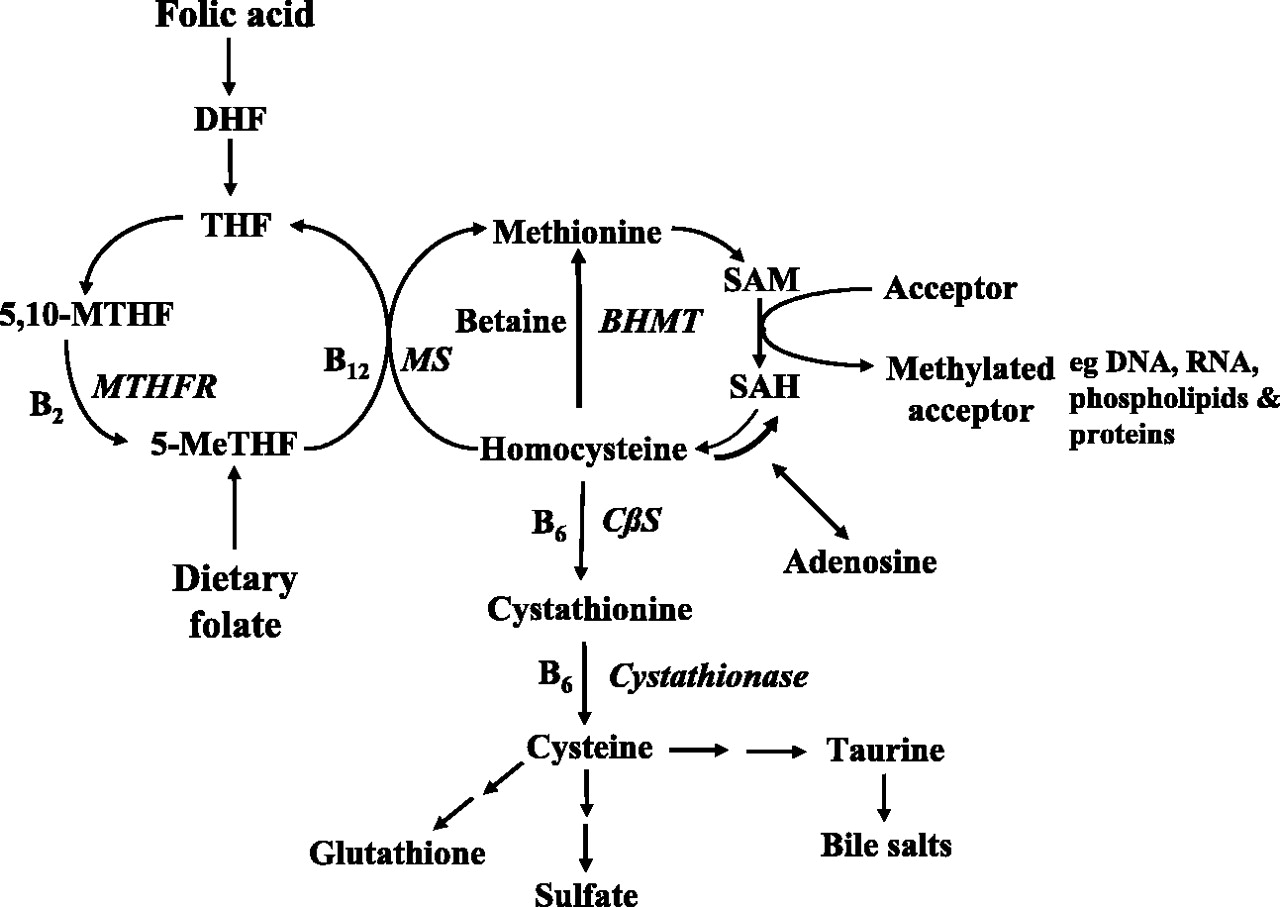
- 65% of patients with insulin resistance (hyperinsulinemia) have a malformation of one or both genes that encode the MTHFR enzyme (methylenetetrahydrofolate reductase) that uses folic acid (Vitamin B9) inside the cells of the body. Because this is genetic and is a process occurring inside the cell, it has been difficult to identify until recent advances in measuring genetic SNPs. Single nucleotide polymorphisms, frequently called SNPs (pronounced “snips”), are the most common type of genetic variation among people.
Interestingly, MTHFR deficiencies are also strongly correlated with depression, anxiety and other forms of mental illness. MTHFR is a SNP that can easily be tested through a simple blood sample at your local lab or doctors office. And, nerve testing can be done through a simple sudomotor function test in the doctors office. In fact, Medicare encourages this testing yearly through part of the Annual Wellness Exam.
The polyneuropathy that I see most commonly in my office can and will improve. In fact, polyneuropathy will completely resolve if you catch it early enough. We treat it in two ways.
What Can I Do To Treat Polyneuropathy?
First, restrict carbohydrate intake. A ketogenic or carnivore diet is the perfect approach to this. If you don’t have a copy of my book, The KetoCure, please pick one up on my website or on Amazon. if you are just looking to fine tune the nuts and bolts of your diet, you can get a copy of my diet recommendations here. Carbohydrate restriction corrects the high insulin levels. Within a few weeks, people start seeing improvement in inflammation, testosterone, estrogen and leptin resistance.
Second, get your MTHFR SNPs tested. This can be ordered through a simple blood test through your doctor or nearby lab. If you have one or both MTHFR mutations, treatment is simple. A mutation of the MTHFR SNP directly causes polyneuropathy, anxiety, depression and in severe cases, schizophrenia. It can also cause significant problems with homocysteine metabolism and is a significant risk factor in heart disease.
Third, use the correct form of folic acid. If you have the MTHFR mutation, regular folic acid is ineffective. Instead of using regular folic acid (Vitamin B9), 1000-5000mcg per day of L-methyl folate (premethylated Vitamin B9) solves the problem. Within 90 days, over 50% of my patients feel dramatic improvement in their neuropathy and many have compete resolution of the numbness and tingling. I see this so frequently, that a few years ago I had my multivitamins designed to include L-methyl folate instead of regular folic acid. You can find them here at Ketoliving. com. If you want more information on why I designed my own vitamin supplement a few years ago, you can read about them here.
So, restrict your carbs, use the appropriate form of folic acid for you, and pass the bacon!
If you are interested in getting more help on this issue, schedule an appointment with me in my office. Or, consider one of my membership options if seeing me in my office isn’t convenient for you. Sign up today!
References:
- Yigit, Serbulent et al. “Association of MTHFR gene C677T mutation with diabetic peripheral neuropathy and diabetic retinopathy.” Molecular vision 19 1626-30. 25 Jul. 2013.
- Wan, Lin et al. “Methylenetetrahydrofolate reductase and psychiatric diseases.” Translational psychiatry 8,1 242. 5 Nov. 2018, doi:10.1038/s41398-018-0276-6.
- Shelton, Richard C et al. “Assessing Effects of l-Methylfolate in Depression Management: Results of a Real-World Patient Experience Trial.” The primary care companion for CNS disorders 15,4 (2013): PCC.13m01520. doi:10.4088/PCC.13m01520.
- Hughes R. Investigation of peripheral neuropathy. BMJ 2010; 341:c6100.
- Morrison B, Chaudhry V. Medication, toxic, and vitamin-related neuropathies. Continuum (Minneap Minn) 2012; 18:139.
- Pareyson D, Piscosquito G, Moroni I, et al. Peripheral neuropathy in mitochondrial disorders. Lancet Neurol 2013; 12:1011.
- Rutkove SB, et al., Overview of Polyneuropathy. UpToDate.com. Online Jan 2020, https://www.uptodate.com/contents/overview-of-polyneuropathy?search=neuropathy&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1