Watch as we discuss the important markers of heart disease and vascular disease risk. We will talk about how these markers can help you understand what your body is doing in the process of making or reversing atherosclerosis (plaque in the vessels). And, should you really be taking that STATIN (cholesterol lowering) drug? Get the scoop here as Dr. Nally very simply points out how the right diet can and will lower your cholesterol without the use of medications.
Research in the last 10 years points to the small-dense LDL particle as the atherogenic component of cholesterol (Hoogeveen RC et al., Arterioscler Thoromb Vasc Biol, 2014 May; Ivanova EA et al., Oxidative Med Cell Longevity, 2017 Apr). Studies in the last five years have identified that elevated small-dense LDL cholesterol correlates much more closely with risk for inflammation, heart disease and vascular disease (Williams PT, et al. Atherosclerosis. 2014 April; 233(2): 713-720.)
Recent research in the last three years demonstrates that small dense LDL cholesterol is a better marker for prediction of cardiovascular disease than total LDL-C (Hoogeveen RC et al., Arterioscler Thromb Vasc Biol. May 2014, 34(5): 1069-1077l; Ivanova EA et al., Oxidative Med Cell Longev. 2017).
Additionally, higher LDL-C is actually predictive of longer life and has been demonstrated to correlate with longevity (Ravnskov U et al., BMJ Open, 2016 Jun 12;6(6): e010401). And, a low LDL-C actually increases risk of early mortality (Schwartz I et al., Lancet 2001, 358: 351-55).
It is commonly understood that LDL-C will rise with increased saturated fat intake on a ketogenic diet. This has been know and reported in the scientific literature for over twenty years. This is to be expected, because LDL-C is really a measurement of three different LDL sub-particles (“big fluffy, medium, and small dense”). Increased saturated fat intake, while at the same time lowering carbohydrate intake, actually causes a shift in these low density particles to a bigger “fluffier” particle conformation (Griffin BA et al., Clin Sci (Lond), 1999 Sep).
The 2015 British Medical Journal, referenced above, analyzed the relevant 19 peer reviewed medical articles that included over 68,000 participants. This review showed that there is no association of high LDL-C with mortality (meaning that an elevated LDL-C does not lead to an increased risk of death from heart or vascular disease). I realize that, in stark opposition to the landmark review above, The American Heart Association’s Presidential Advisory published their position in the June 20, 2017 issue of Circulation. They stated that saturated fat is the cause of increased LDL-C and they further extrapolated that elevated LDL-C is associated with an increase in death by cardiovascular disease. This boldfaced claim is only based on one single small four year (2009-2013) literature review completed by the World Health Organization with a total of only 2353 participants, most of these studies only lasting 3-5 weeks (not nearly long enough to see fully effective cholesterol changes) and none of which had any focus on carbohydrate intake, insulin levels or LDL sub-particle measurement (Mensink RP, Geneva: WHO Library Cataloguing-in-Publication Data, 2016).
Based upon the most current scientific evidence above and my clinical experience, the large body of evidence above demonstrates the use of total cholesterol and LDL-C to determine vascular disease risk to be ineffective tools. A low carbohydrate/ketogenic diet lowers small dense LDL cholesterol, triglycerides and blood sugar and in many cases, the use of cholesterol drug (STATIN) therapy is not needed and ineffective in comparison with a ketogenic/carbohydrate restricted lifestyle.
Over fifty years of data have demonstrated that creating energy deficit through the reduction in caloric intake is effective in reducing weight. . . However, it is only for the short term (1, 2). The biggest challenge physicians face in the treatment of obesity is that calorie restriction fails when it comes to long-term weight loss.
Isn’t Fasting Effective in Long-Term Weight Loss?
With the craze and popularity of intermittent fasting, some have claimed that intermittent fasting is more effective in weight reduction. Recent results demonstrate that this may also be incorrect. In the short term evaluation of caloric restriction and intermittent fasting, reduction in 15-20 lbs of weight is effectively seen and the highly publicized Biggest Loser’s losing ~ 120 lbs. Intermittent fasting and alternate day fasting have been shown to be more effective in lowering insulin levels and other inflammatory markers in the short term.
There is, however, controversy over maintaining weight loss beyond 12 months in the calorie restriction, intermittent and alternate day fasting groups. Forty different studies in a recent literature review, thirty-one of those studies looking at forms of intermittent fasting, demonstrate that the majority of people regain the weight within the first 12 months of attempting to maintain weight loss(3, 5). This is, also, what I have seen for over 18 years of medical practice.
Is Calorie Restriction the Only Way to Lose Fat?
Numerous “experts” claim that the only way to reduce fat is “caloric deficit.” Variations through the use of intermittent, long-term or alternate day fasts can be found all over the internet. In regards to calorie restriction, these “experts” with nothing more than a personal experience and a blog to back their claims preach this louder than the “televangelists” preach religion. Based on the faith that many place in this dogma, it could be a religion. What causes belief in this dogma is that weight and fat loss actually does occur with caloric restriction to a point. The average person will lose 20-25 lbs, however, within 12 months of achieving this goal, most people regain all the weight. (No one ever mentions the almost universal problem with long-term weight loss, especially those “experts.”)
Prolonged calorie restricted fasts, intermittent fasts, and alternate day fasts are often grouped together into the fasting approach, causing significant confusion among those that I speak to and counsel in my office. There is great data that alternate day fasts do not have the reduction in resting energy expenditure that prolonged fasting, intermittent fasting and calorie restriction cause. However, none of these approaches appears to solve the problem of weight re-gain after long-term (12-24 months into maintenance) weight loss (3). And, a recent study of 100 men participating in alternate day fasting showed that there was a 38% dropout rate, implying that without close supervision and direction, maintenance of this lifestyle is not feasible for over 1/3rd of those attempting it.
Long-Term Weight Loss Failure Brings Tears
Failure on calorie restricted diets, low fat diets, and intermittent fasting diets with weight regain at twelve to twenty-four months is the most common reason people end up in my office in tears. They’ve fasted, starved themselves, calorie restricted, tried every form of exercise, and still regained the weight. Trainers, coaches and “experts” have belittled them for “cheating” or just not keeping to the diet. Yet, we know that calorie restriction and intermittent fasting cause a rebound in leptin, amilyn, peptid YY, cholecystikinin, insulin, ghrelin, gastric inhibitory peptide and pancreatic poly peptide by twelve months causing ineffective long-term weight loss (6). The dramatic rise in these hormones stimulates tremendous hunger, especially from ghrelin and leptin.
N Eng J Med 27 Oct 2011. Mean (±SE) Fasting and Postprandial Levels of Ghrelin, Peptide YY, Amylin, and Cholecystokinin (CCK) at Baseline, 10 Weeks, and 62 Weeks.
Although less problematic in alternate day fasting, these calorie restricted approaches also cause dramatic slowing of the metabolism at the twelve month mark. In many cases, the metabolic rate never actually returns to baseline, creating even more difficulty in losing further weight or even maintaining weight (6).
N Engl J Med 27 Oct 2011. Mean changes is weight from 0 – 62 weeks.
Is Gastric Bypass or Gastric Sleeve the Solution?
Gastric bypass and the gastric sleeve procedures have been touted as the solution to this problem, as they decrease ghrelin, however, 5-10 years later, these patients are also back in my office. They find that 5-10 years after these procedures the weight returns, cholesterol and blood pressure rise, and diabetes returns. These hormones kick into high gear, stimulating hunger in the face of a slowed metabolism, that to date, has been the driver for weight regain in the majority of people. People find it nearly impossible to overcome the hunger. You may have experienced this, I know I have.
It’s the Hormones, Baby!
So, what is the answer? It’s the hormones. (WARNING – You’ll hear that when your wife is pregnant, too, gentlemen). We are hormonal beings, both in weight gain, and in pregnancy. Trying to preach calorie control to a hormonal being is like showing up at the brothel to baptize the staff. You might get them into the water, but you’re probably not getting them returning weekly to church or pay a tithe.
So, how do you manipulate the hormones in a way to control the rebounding hunger and suppression of metabolism? This is where we put a bit of twist on the knowledge we’ve gained from alternate day fasting. Recent research shows that “mild” energy deficit in a pulsatile manner, that has the ability to mimicking the body’s normal bio-rhythm’s is dramatically effective in reducing weight and maintaining normal hormonal function without cause of rebound metabolic slowing (4).
Pulsed Mild Energy Restriction
What does this mean in layman’s terms? It means that if we provide a diet that maintains satiety hormones while providing a period of baseline total energy expenditure needs and a period of mildly reduce caloric intake in a pulsed or cyclic manner, greater weight loss occurs and there is no rebound of weight 1-2 years later.
The main reason I’ve not jumped on the intermittent fasting band wagon is the shift in leptin, amylin, ghrelin and GLP-1 signaling that regularly occurs at the 6-12 month mark. The rebound of these hormones causes weight re-gain and is what prevents successful long-term weight loss. A number of people come to my office and tell me they couldn’t follow a ketogenic diet, so they’re doing intermittent fasting and it works . . . for a while. Then, they end up in my office having hit a plateau or fallen off the wagon and regained all the weight. They are completely confused and don’t understand what happned. Most of them are convinced it’s their thyroid or cortisol and they’ve seen every naturopath and functional medicine doctor in town.
What people really need is a simple approach to long-term weight loss without having to spend the night in the physiology lab every two weeks sleeping under a ventilated hood system.
The Ketogenic Lifestyle is a Pulsed Energy Lifestyle
Third, providing adequate fat is the simple way to maintain leptin, ghrelin, amylin, GLP-1 (among the others) and long-term weight loss. Can you eat too much fat? Of course you can. But, because each of us have differing levels of stress and activity each day, this fat intake becomes the lever for hunger control.
Fourth, the use of exogenous ketones ensures easily accessible ketone (short chain fatty acids) to modulate adipose (white fat) signaling of the liver without large caloric intake through the portal vein by first pass of liver metabolism. The ketones also help stabilize the gut bacteria. The combination of hormone balance between the liver and fat cells and improvement of gut bacteria suppresses key hunger hormones and aids glucose regulation between the fatty tissues and the liver. Ketones, both endogenous and exogenous, suppress production of TNF-alpha, IL-6, resistin, and stabilize production of adiponectin and leptin from the adipose cells (7, 8, 9).
In my office, once we calculate the basic protein needs daily, we start with a 1:1 ratio of protein to fat. Then, the fat is adjusted up or down based on hunger. Remember, hunger occurs, because your body produces hormones. The addition of fat to a diet that is not stimulating large amounts of insulin resets the hormone patterns back to normal without causing weight gain.
Give Obese People Fat Ad Libitum?
“Sure, Dr. Nally, but what about those people who don’t know if they are hungry, bored, stressed or just have a bacon fixation? You can’t just give them all the fat they want?!”
Why not? Implying that people aren’t smart enough to know when they are full is a bit of a fascist philosophy, don’t you think?
Do people over eat? Sure they do. But, I’ve found that when you give people an antidote to hunger (using fat intake in the presence of stabilized insulin levels) over a few months, people begin to recognize true hunger from other forms of cravings. This is especially true when they keep a diet journal. This gives people the ability to begin listening to their own bodies, responding accordingly and governing their stress, eating, exercise and activity. Keeping a diet journal is key to long-term weight loss. And, isn’t helping people use their own agency to improve their health really what we’re trying to do?
Interestingly, doing this over the years seems to line up with the findings of this year’s MATADOR study in the International Journal of Obesity. They found that mild intermittent energy restriction of about 30-33% for two weeks, then interrupting this with two weeks of a diet that was energy balanced for needs improved both short and long-term weight loss efficiency (4). In looking at my, and my patient’s diet journals, this energy restriction of about 1/3 of needed calories cyclically seems to happens naturally with a ketogenic lifestyle, without even counting calories. (Calories are a swear-word in my office).
What does the correct long-term wight loss program look like in a diet or meal plan? Well, you’ll have to join the Ketogenic Lifestyle 101 Course to see what that really means to you individually. I look forward to seeing you there.
Want to find out more about the Ketogenic Lifestyle 101 course? CLICK HERE.
Have you read my book The Keto Cure? Get a signed copy from me by clicking HERE.
References:
Bronson FH, Marsteller FA. “Effect of short-term food deprivation on reproduction in female mice.” Biol Reprod. Oct 1985; 33(3): 660-7. https://www.ncbi.nlm.nih.gov/pubmed/4052528?dopt=Abstract&holding=npg
Connors JM, DeVito WJ, Hedge GA. “Effects of food deprivation on the feedback regulation of the hypothalamic-pituitary-thyroid axis of the rat.” Endocrinology. Sep 1985. 117(3): 900-6. https://www.ncbi.nlm.nih.gov/pubmed/3926471?dopt=Abstract&holding=npg
Seimon RV, Roekenes JA, Zibellini J, Zhu B, Gibson AA, Hills AP, Wood RE, King NA, Byrne NM, Sainsbury A. “Do intermittent diets provide physiological beneftis over continuous diets for weight loss? A systematic review of clinical trials.” Mol Cell Endo. 15 Dec 2015. 418(2): 153-172. https://www.sciencedirect.com/science/article/pii/S0303720715300800
Byrne NM, Sainsbury A, King NA, Hills AP, Wood RE. “Intermittent energy restriction improves weight loss efficiency in obese men: the MATADOR study.” Int J Obes. 2018. 42:129-138. https://www.nature.com/articles/ijo2017206
Trepanowski JF, Kroeger CM, Barnosky A. “Effect of Alternate-Day Fasting on Weight Loss, Weight Maintenance, and Cardioprotection Among Metabolically Healthy Obese Adults.” JAMA Intern Med. Jul 2017. 177(7): 930-938. https://jamanetwork.com/journals/jamainternalmedicine/article-abstract/2623528?redirect=true
Sumithran P, Prendergast LA, Delbridge E, Purcell K, Shulkes A, Kriketos A, Proietto J. “Long-term persistence of hormonal adaptations to weight loss.” N Engl J Med. 27 Oct 2011. 365: 1597-1604. http://www.nejm.org/doi/full/10.1056/NEJMoa1105816
Asrih M et al., “Ketogenic diet impairs FGF21 signaling and promotes differential inflammatory responses in the liver and white adipose tissue.” PlosOne. 14 May 2015. Open Access. https://doi.org/10.1371/journal.pone.0126364
Veniant MM et al. “FGF21 promotes metabolic homeostasis via white adipose and leptin in mice.” PlosOne. Jul 2012. Open access. https://doi.org/10.1371/journal.pone.0040164
Whittle AJ, “FGF21 conducts a metabolic orchestra and fat is a key player.” Endocrinology. 1 May2016. 157(5): 1722-1724.
Have you been cutting your calories and reducing fat and exercising your brains out and still not seeing the needle on the scale move that much? Persistently and repetitively performing an action that doesn’t produce the desired result is insanity. Cutting calories and reducing fat while expecting weight loss is akin to pouring water in the gas tank of your car and expecting it to run smoothly. Why do we do it? Are the 53, 000, 000 people with health club and gym memberships this year really insane?
This evening on PeriScope we touch on fat phobic insanity and the limiting step that actually turns weight gain on or off. (We knew about this in the 1960’s, we just ignored it.)
You can see tonight’s PeriScope with the rolling chat-box questions here at Katch.me/docmuscles. Or, you can watch the video stream below:
The only way to successfully loose weight is to modify or turn off the mechanisms that stimulate fat storage. For years we have been told that this was just a problem of thermodynamics, meaning the more calories you eat, the more calories you store. The solution was, thereby, eat less calories or exercise more, or both. We are taught in school that a 1 gram of carbohydrate contains 4 kcal, 1 gram of protein contains 4 kcal, and 1 gram of fat contains 9 kcal.
If you ascribe to the dogma that weight gain or loss is due to thermodynamics, then it’s easy to see that cutting out fat (the largest calorie containing macro-nutrient) would be the best way limit calories. For the last 65 years, we as a society have been doing just that, cutting out fat, exercising more (with the idea of burning off more calories) and eating fewer calories.
What has this dogma done for us? It’s actually made us fatter! (1)
Obesity Rates Around the World
Some may argue that we really aren’t eating fewer calories and exercising more. But most people I have seen in my office have tried and tried and tried and failed and failed and failed to loose weight with this methodology. In fact, the majority of my patients attempt caloric restriction, exercise and dieting multiple times each year with no success. The definition of insanity is “doing the same thing over and over and expecting a different result.”
Most of my patients are not insane, they recognize this and stop exercising and stop restricting calories . . . ’cause they realized, like I have, that it just doesn’t work!
If you’re one that is still preaching caloric restriction and cutting out fat, I refer you to the figure above and the definition of insanity . . . your straight-jacket is in the mail.
So, if reducing the calories in our diet and exercising more is not the mechanism for turning on and off the storage of fat, then what is?
Before I can explain this, it is very important that you appreciate the difference between triglycerides and free fatty acids. These are the two forms of fat found in the human body, but they have dramatically different functions. They are tied to how fat is oxidized and stored, and how carbohydrates are regulated.
Fat stored in the adipose cells (fat cells) as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
(“What! Fat comes from sugar?! How can this be?!!“)
De Novo Lipogenesis
We all know that glucose derived from sugar is taken up by the cells from the blood stream and used for fuel, however, when too much glucose is in the blood stream or the blood sugar increases above the body’s comfort zone (60-100 ng/dl), the body stores the excess. The process is called de novo lipogenesis, occurring in the liver and in the fat cells themselves, fancy Latin words for “new fat.” It occurs with up to 30% (possibly more if you just came from Krispy Kream) of the of the carbohydrates that we eat with each meal. De novo lipogenesis speeds up as we increased the carbohydrate in our meal and slows down as we decrease the carbohydrate in our meal. We’ve known this for over 50 years, since it was published by Dr. Werthemier in the 1965 edition of the Handbook of Physiology (2).
While we know that fat from our diet and fat from our food is stored as triglyceride, it has to enter and exit the fat cell in the form of fatty acids. They are called “free fatty acids” when they aren’t stuck together in a triglyceride. In their unbound state, they can be burned as fuel for the body within the cells. I like to think of the free fatty acids as the body’s “diesel fuel” and of glucose as the body’s version of “unleaded fuel.” The free fatty acids can easily slip in and out of the fat cell, but within the adipose cell, they are locked up as triglycerides and are too big to pass through the cell membranes. Lipolysis is essentially unlocking the glycerol from the free fatty acids and allowing the free fatty acids to pass out of the fat cell. Triglycerides in the blood stream must also be broken down into fatty acids before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).
So when carbohydrates increase in the diet, the flow of fat into the fat cell increases, and when carbohydrates are limited in the diet, the flow of fat out of the fat cells increases.
Summarizing the control mechanism for fat entering the fat cell:
The Triglyceride/Fatty Acid cycle is controlled by the amount of glucose present in the fat cells (conversion to glycerol phosphate) and the amount of insulin in the blood stream regulating the flow of fatty acid into the fat cell
Glucose/Fatty Acid cycle or “Randle Cycle” regulates the blood sugar at a healthy level. If the blood glucose goes down, free fatty acids increase in the blood stream, insulin decreases, and glycogen is converted to glucose in the muscle and liver.
These two mechanisms ensure that there is always unleaded (glucose) or diesel fuel (free fatty acids) available for every one of the cells in the body. This provides the flexibility to use glucose in times of plenty, like summer time, and free fatty acids in times of famine or winter when external sources of glucose are unavailable.
The regulation of fat storage, then, is hormonal, not thermodynamic. Unfortunately, we’ve know this for over 65 years and ignored it.
We’ve ignored it for political reasons, but that’s for another blog post . . .
References:
1. James, W. J Intern Med, 2008, 263(4): 336-352
2. Wertheimer, E. “Introduction: A Perspective.” Handbook of Physiology. Renold & Cahill. 1965.
3. Taubs, G. “The Carbohydrate Hypothesis, II” Good Calorie, Bad Calorie. Random House, Inc. 2007, p 376-403.
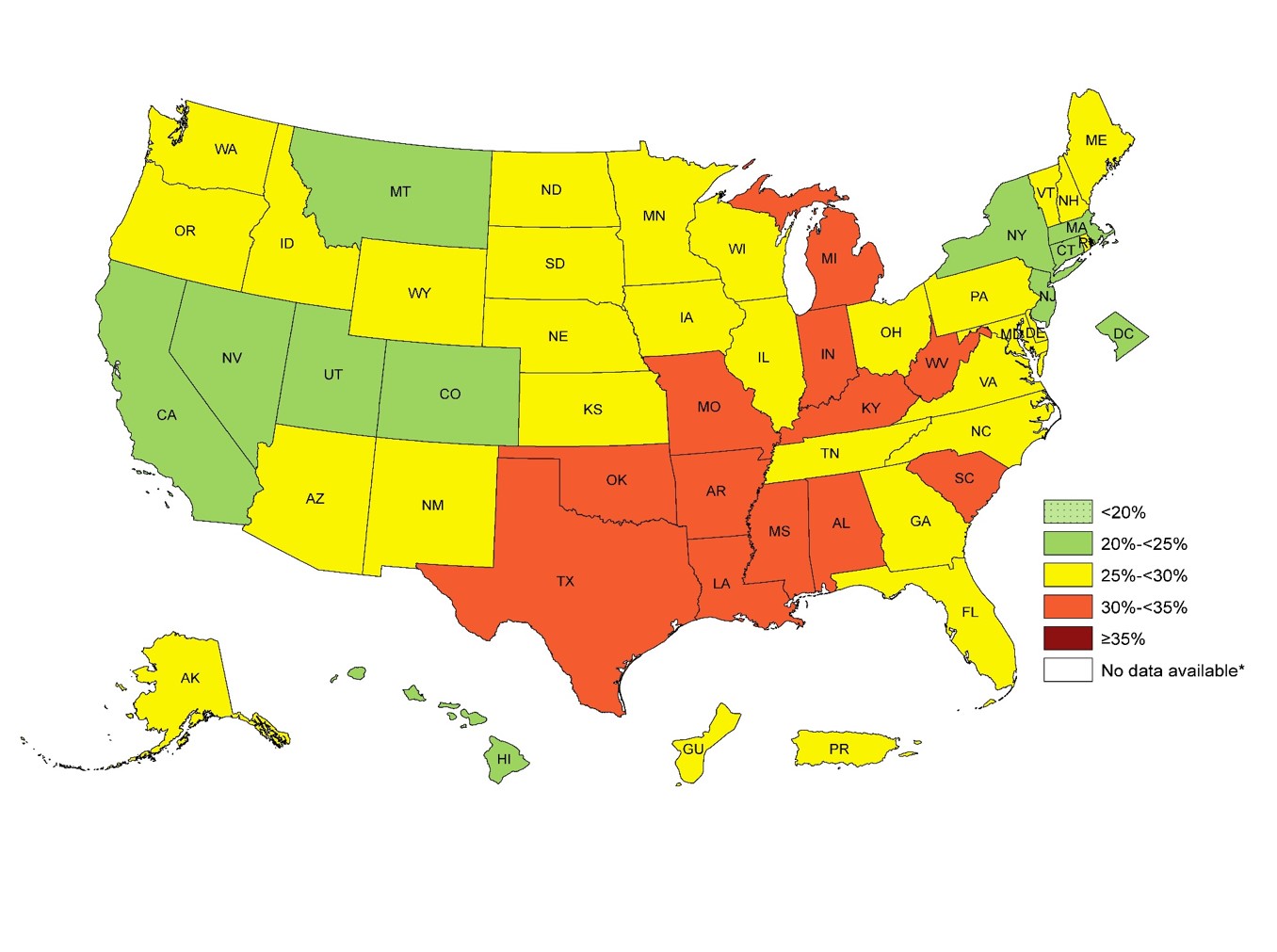
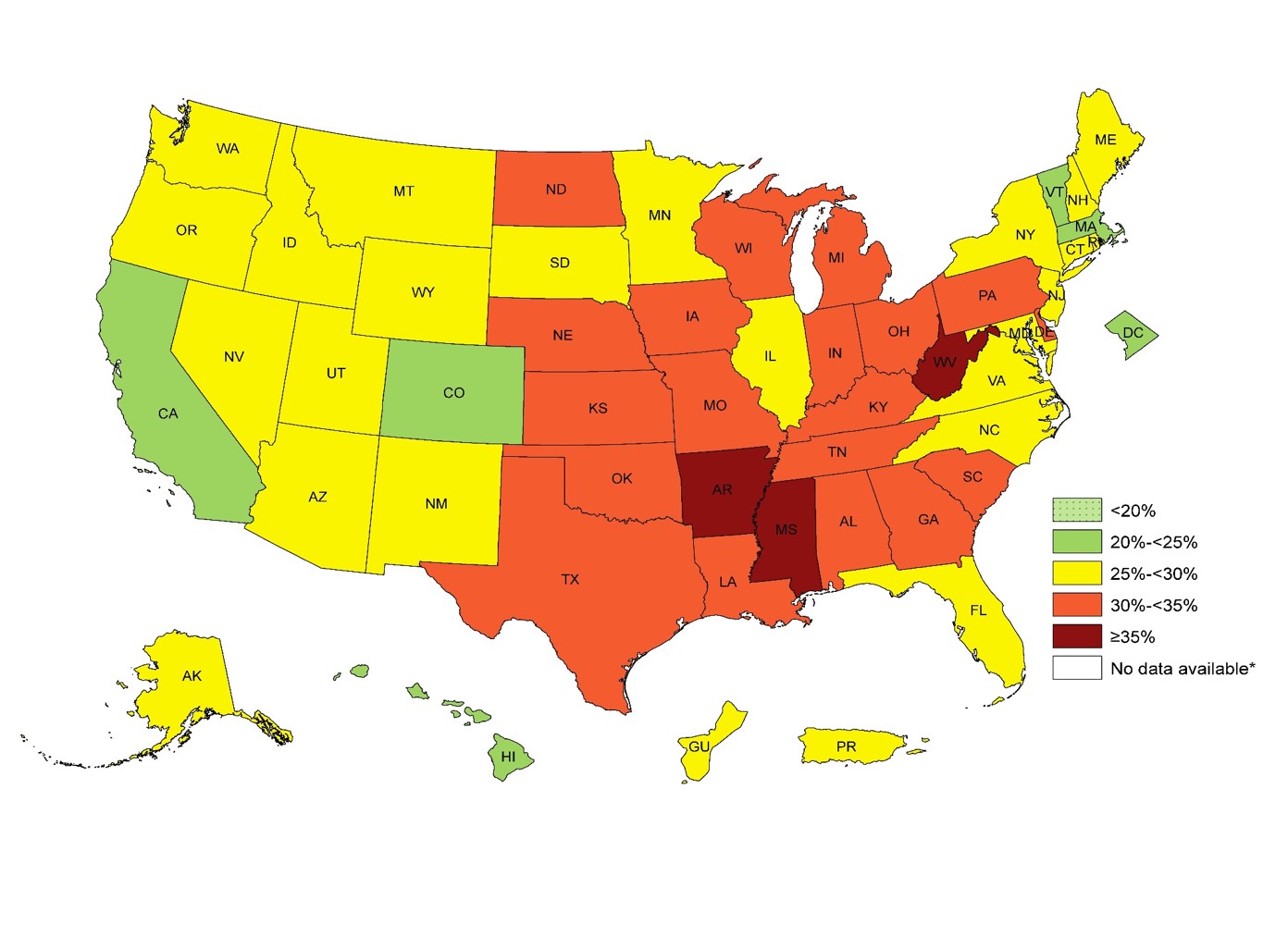
Today in the office I had the calorie conversation again . . . three times. We have an entire society with a very influential health and fitness industry built around the almighty calorie. Has it helped? Looking at our 5 year obesity outcomes. It hasn’t helped a bit. In fact, it is worse. In 1985 only 19% of U.S. adults were obese.
U.S. Obesity Adult 2011U.S. Adult Obesity 2014
In 2014, 34.5% of U.S. adults were obese. The numbers this year are approaching 35.6% You can see the dramatic increase in obesity by 1-3% every year for the last 5 years in the CDC images above.
For over 50 years we have been told that caloric restriction and fat restriction is the solution. But by the numbers above, the 58 million people in the U.S. utilize a gym or health club to burn off those calories aren’t seeing the success that they should be expecting.
Why? Because the calorie is NOT king. What do I mean by that? We don’t gain weight because of the thermogenic dogma we’ve been taught for the last 50 years. Our weight gain is driven by a hormone response to food. Hear more about why the calorie is NOT king on tonight’s PeriScope. You can Katch it here with all the live stream comments and hearts at Katch.me/docmuscles.
Or you can watch the video without the comments here:
85% of the people that walk through my office doors have some degree of insulin resistance.
What is “insulin resistance?” It is an over production of insulin in response to ANY form of carbohydrate intake (yes, even the “good carbs” cause an insulin over-response in a person with insulin resistance.)
How do I know this? Because I routinely check insulin levels (I check them every three months) and the down stream markers of insulin on a large number of the patients that I see. I have been fascinated by the fact that a diet high in both sugar and fat [like the Standard American Diet, (SAD) diet] turn on the genetics leading to insulin resistance. Starch and sugar load the genetic gun.
Insulin acts like a key at the glucose doorway of every cell in your body. In many people, the insulin signal is blocked by hormones produced in the fat cell and the the insulin, acting like a “dull or worn out key” – can’t open the glucose doorway as efficiently.
So, the body panics, and releases extra insulin in response to the same load of carbohydrate or glucose. People with insulin resistance will produce between 2-20 times the normal amount of insulin in response to a simple carbohydrate load. Recent studies(1, 2) reveal high cholesterol and diets high in both fat and carbohydrate cause insulin resistance to progress or worsen.
So, instead of producing enough insulin to accommodate the one slice of bread or the one apple that you might eat, the insulin resistant person produces enough insulin for an entire loaf of bread or an entire bushel of apples. This excess insulin then stimulates one or all of the following:
Weight Gain – Insulin directly stimulates weight gain by activating lipoprotein lipase to take up triglycerides into the fat cells. This causes direct storage of fat and increases your waistline. (3)
Elevated Triglycerides – Insulin directly stimulates production of free fatty acids and triglycerides through hepatic gluconeogenesis and is even more notably amplified by the broken signaling mechanism of the FOX-01 phosphorylation mechanism in patients with insulin resistance. (4)
Increased number of Small Dense LDL (sdLDL) particles – Low density lipoprotein (LDL, or “bad cholesterol”) is actually comprised of various sized lipoproteins including small, medium and large. As triglycerides increase, the small dense LDL particle numbers increase. Research points to the fact that it is the small dense particle that is highly atherogenic (leading to the formation of vascular plaques within the arteries). (5, 8)
Elevated Uric Acid – Leptin resistance and insulin resistance syndromes are often found together and are suspected to have significant influence on each other. High insulin loads lead to “sick adipose cells” causing leptin resistance. This has a dramatic effect on hepatic fructose metabolism increasing the production of uric acid. Excess insulin suppresses urinary excretion of uric acid and dramatically increases serum content of uric acid and the risk of kidney stones and gout. (6, 7)
Increased Inflammation – Increased levels of circulating insulin have a direct correlation on raising many of the inflammatory markers and hormones including TNF-alpha and IL-6 in the body (9). Any disease process that is caused by chronic inflammation can be amplified by increased circulating levels of insulin including asthma, acne, eczema, psoriasis, arthritis, inflammatory bowel and celiac disease, etc.
Elevated Blood Pressure – Increased uric acid production from insulin resistance as noted above directly suppresses production of nitric oxide within the vasculature and increases blood pressure (7). This completes the triad of metabolic syndrome (elevated triglycerides & cholesterol, weight gain, and elevated blood pressure) found in patients with insulin resistance.
Water Retention – We have known for many years that insulin affects the way the kidney uses sodium in the distal nephron. Insulin has a direct effect on sodium retention in the kidney. As insulin levels rise, the kidney retains increased levels of sodium (10). Water follows sodium and thereby causes fluid retention. This is the reason that many of my insulin resistant patients who have struggled with leg swelling and edema suddenly improve when they correct their diet and their high circulating insulin levels fall. It is also the reason that many of my patients show up in my office after the holidays with swollen legs and amplified swelling in their varicose veins after cheating on their ketogenic diets.
If you are plagued by any or all of these, my first suggestion is to see your doctor and get screened for insulin resistance. I treat patients with these every day and have reversed these effects in thousands of patients with the correct diet and/or medications. Having seen these signs and patterns over the last 20 years of medical practice, I am still astonished every day by the dramatic effect our diet plays on the hormonal changes within the body. Remember that the food you eat is actually the most powerful form of medicine . . . and the slowest form of pernicious poison.
Cholesterol Elevation Impairs Glucose-Stimulated Ca2+Signaling in Mouse Pancreatic β-Cells, Endocrinology, June 2011, Andy K. Lee, Valerie Yeung-Yam-Wah, Frederick W. Tse, and Amy Tse; DOI: http://dx.doi.org/10.1210/en.2011-0124
Glucose-Stimulated Upregulation of GLUT2 Gene Is Mediated by Sterol Response Element–Binding Protein-1c in the Hepatocytes, DIABETES, VOL. 54, JUNE 2005; Seung-Soon Im, Seung-Youn Kang, So-Youn Kim, Ha-il Kim, Jae-Woo Kim, Kyung-Sup Kim and Yong-Ho Ahn
Selective versus Total Insulin Resistance: A Pathogenic Paradox, Cell Metabolism, Volume 7, Issue 2, 6 February 2008, Pages 95–96, Michael S. Brown, Joseph L. Goldstein
Association between small dense LDL and early atherosclerosis in a sample of menopausal women, Department of Clinical Medicine and Surgery, University “Federico II” Medical School, Naples, Italy Division of Cardiology, Moscati Hospital, Aversa, Italy A. Cardarelli Hospital, Naples, Italy, Gentile M, Panico S, et al., Clinica Chimica Acta, 2013
Sugar, Uric Acid and the Etiology of Diabetes and Obesity. Diabetes. 2013;62(10):3307-3315, Richard J. Johnson; Takahiko Nakagawa; L. Gabriela Sanchez-Lozada; Mohamed Shafiu; Shikha Sundaram; Myphuong Le; Takuji Ishimoto; Yuri Y. Sautin; Miguel A. Lanaspa
Fructose: metabolic, hedonic, and societal parallels with ethanol. J Am Diet Assoc. 2010 Sep;110(9):1307-21. doi: 10.1016/j.jada.2010.06.008. Lustig RH
Cardiovascular Risk in Patients Achieving Low-Density Lipoprotein Cholesterol and Particle Targets. Atherosclerosis. Vol 235; 585-591, May 2014, Peter P. Toth, Michael Grabner, Rajeshwari S. Punekar, Ralph A. QuimboMark J. Cziraky c, Terry A. Jacobson
Chronic Subclinical Inflammation as Part of the Insulin Resistance Syndrome The Insulin Resistance Atherosclerosis Study (IRAS), Circulation, July 2000, 102:42-47; Andreas Festa, MD; Ralph D’Agostino, Jr, PhD; George Howard, DrPH; Leena Mykka¨nen, MD, PhD; Russell P. Tracy, PhD; Steven M. Haffner, MD
The Effect of Insulin on Renal Sodium Metabolism. Diabetologia. September 1981, Volume 21, Issue 3, pp 165-171. R. A. DeFronzo




 So, how do you manipulate the hormones in a way to control the rebounding hunger and suppression of metabolism? This is where we put a bit of twist on the knowledge we’ve gained from alternate day fasting. Recent research shows that “mild” energy deficit in a pulsatile manner, that has the ability to mimicking the body’s normal bio-rhythm’s is dramatically effective in reducing weight and maintaining normal hormonal function without cause of rebound metabolic slowing (4).
So, how do you manipulate the hormones in a way to control the rebounding hunger and suppression of metabolism? This is where we put a bit of twist on the knowledge we’ve gained from alternate day fasting. Recent research shows that “mild” energy deficit in a pulsatile manner, that has the ability to mimicking the body’s normal bio-rhythm’s is dramatically effective in reducing weight and maintaining normal hormonal function without cause of rebound metabolic slowing (4).

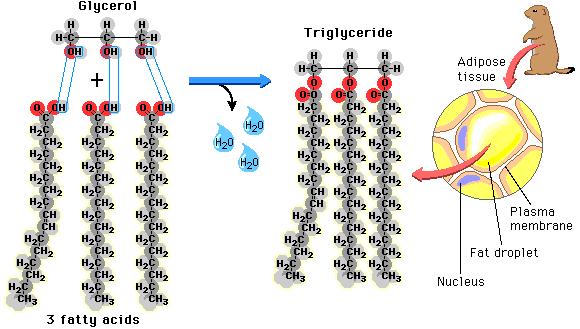 as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
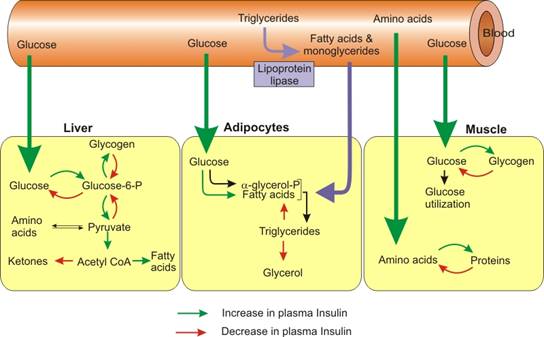 before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).
before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).