I’ve been told that many of you have nominated me. Thank you!!!
Every year Ketogenic.com hosts the Keto Awards with Metabolic Health Summit to highlight some of the best and brightest in our community.
There are five unique categories in which you can nominate and it would be an honor to me for you to add your vote: Top Keto Educator Top Keto Book Top Keto Podcast Top Keto Researcher Making Positivity Louder
I’ll be sure to let you know who is selected. Please take a minute to cast your vote for me. Vote Here:
A few years ago, my son and I were scuba diving the “Fish Bowl” just off the coast of the beautiful island of St Thomas in the Virgin Islands. This dive was 60-80 feet below the surface and was some of the most beautiful coral reef and aquatic life I have ever seen. The water was crystal clear with unlimited visibility and there were hundreds of schools of fish in this area.
As we dove into this amazingly beautiful depressed bowl-shaped area of coral that was about the size of a football field, more and more aquatic wildlife came into view.
We saw thousands of fish – the most colorful fish I’ve ever seen, hundreds of different species. We saw sting rays, barracuda, lobster, and some of the most beautiful coral I have ever witnessed. It was exhilarating, breathtaking and peaceful all at the same time.
However, as we swam over and around the ocean floor and through the coral caverns that lined it’s walls, I noticed something very unique. All of these species of aquatic life would swim, then rest. Many of them would rest for a period on the ocean floor or in a cove or cavern of the beautiful walls of coral reef.
Then, every few minutes, I’d catch the view of a group of reef sharks as they swam by. As they swam, they would watch us, and swim over or under our diving group. Yet, the sharks never stopped. They never rested or waited quietly on the ocean floor like the other aquatic predators we saw that day.
Majestic and fearsome creatures with the beautiful waving motion of their tails, sliding smoothly through the saltwater along the edges of the reef. These reef sharks and the other nurse and hammer head sharks we saw never stopped.
I learned a fascinating lesson that day. If a shark stops swimming, it dies.
The ocean may be its home . . .
And, the shark may be one of the most fearsome creatures under the deep blue . . .
But, without forward movement, the shark will drown. Sharks rely upon obligate ram ventilation of water passing through their mouths filtering oxygen as it is rammed against the gills.
If they stop swimming, they stop receiving oxygen. If they stop moving, they die.
It was a powerful life lesson.
You and I are much like the shark, we survive on a diet of protein, fat and movement.
You are a fearsome collection of appetites, powers, and instincts made for constant forward movement.
If you do not grow . . .
If you do not evolve, risk, or expand . . . Slowly but surely, you will die a spiritual or emotional death.
You may wish and pray it were otherwise. You can try to will yourself content with stagnation and starch . . .
You can try to force yourself to be satisfied. Believe me, I’ve tried.
Yet, as you know by now . . . it doesn’t take. It doesn’t work. Your hunger increases, and you start gasping for air.
You are the shark.
To whatever extent you have failed to move forward, that lack of momentum is drowning you in a deep blue sea of “what if’s,” “could have’s,” and “if only’s.”
You and I are not overwhelmed.
You are not suffering from too much. You and I suffer from TOO LITTLE.
Underwhelm frequently masquerades as overwhelm, and it stifles the life-giving apparatus.
You’re not over stretched. You’re not tapped out. You are profoundly under-utilized . . . bored, rotting & stymied.
The narrow walls of your life begin crushing your heart when you’re not moving. You know it’s true.
Even when everything within you wants to retreat . . .
Fin your tail, flair your vents and MOVE FORWARD.
Do not be afraid to play the bigger game, take the wild risk, make the bold move.
I gained four life lessons from this experience. These make more sense when viewed with this perspective:
Happiness is not the absence of problems; it is the ability to deal with them, swim at them head on.
Feeling sad after making a decision doesn’t mean you made the wrong decision. You decide and you keep moving.
You’re not stressed out because you are doing too much. You are stressed because you are doing too little of the things that make you feel most alive, the thing that keeps the oxygen moving across your gills.
The lesson you struggle with will repeat itself until you face it and learn from it.
Be the shark you were meant to be, and, at last, watch your life begin.
Many people are looking for natural sources of collagen.Every day in my clinic, I get asked about which collagen supplement I recommend using.People have been convinced over the years by great sales and marketing that they must have some form of supplemental collagen.
This is an important question, because there are many benefits to collagen. As the most abundant protein in our body, collagen is essential for:
·Fighting signs of aging like wrinkles
·Improving joint health and osteoarthritis
·Healing Irritable Bowel & Leaky Gut Syndrome
·Boosting metabolism
·Improving mental health
·Reducing the appearance of cellulite
·Strengthening hair & nails
·Great looking skin
WHAT IS COLLAGEN?
In the body, collagen is mostly found in the skin, bones, and joints. It also is found in the lining of the gut. We’ve known for years that gut health is incredibly important for overall health!
Collagen in the body is made up of amino acids which wrap together to make a triple-helix structure. The helix structure is why collagen is so strong.
The amino acids which make up collagen are:
·Glycine: Makes up about 33% of collagen
·Proline: Makes up about 10% of collagen
·Hydroxyproline: Makes up about 10% of collagen
·Hydroxylysine: Makes up about 1% of collagen
The 5 most common types are Type I, II, III, IV and V.
·Type I Collagen is the most abundant in our body (over 90%) and stronger than steel by weight. It is found in skin, hair, nails, muscle, joints and organs.
·Type II Collagen makes up movable joints.
·Type III (the so-called ‘baby collagen’) is the second most abundant collagen in human tissue.
·Type IV forms basal lamina, the epithelium-secreted layer of the basement membrane.
·Type V is present in cell surfaces, hair and placenta.
WHY YOU NEED COLLAGEN
Our bodies make collagen out of amino acids we consume through food. However, as we age, our bodies ability to make collagen declines. Thus, around the age of 30, collagen production begins to diminish by about 1% to 2% yearly. By the age of 40, you and I lose 10% to 20% of our collagen!
UV rays, cigarette smoke, pollution, poor diet lacking in the necessary amino acids causes our skin’s structural integrity to be compromised.
Our dermis is made up of more than 80% Type I Collagen and 15% Type III Collagen, along with Elastin and Hyaluronic Acid, and specialized cells called ‘Fibroblasts’ (the essential ‘collagen factories’ that synthesize new collagen).
Together they are the key components for the extracellular matrix which gives our skin its structure, elasticity and firmness.
Collagen is the key foundational protein for healthy, youthful-looking skin.
To produce collagen, our bodies first need to have amino acids as the building blocks for collagen. Millions of people around the world were indoctrinated in the low-fat diet dogma taught in grade school since the 1970’s. If you’ve been eating a low fat, vegetarian or vegan diet, which is lacking in those crucial amino acids, your body won’t be able to produce enough collagen!
Why? Because those amino acids above are found in animal proteins and animal fats, specifically from the connective tissues of cows and pigs (amazing how bacon is necessary for everything, right?!)
To make things worse, naturally-occurring enzymes in our bodies also break down collagen. Environmental factors like pollution, free radicals, and excessive sun exposure can also break down collagen.
THE #1 SOURCE OF COLLAGEN: Natrual GELATIN
When it comes to sources of collagen, you won’t find anything better than gelatin. Why? Because gelatin IS collagen.As mentioned above, gelatin comes from the connective tissue of cows, pigs and is found in whites and yolks of eggs. You can also get some types of collagen from fish.
Slow cooking or smoking beef and pork liquifies the connective tissues in these meats and creates the moistness that is so very delicious.
The great thing about gelatin is that it is easy for the body to digest and absorb. But, don’t expect your wrinkles or joint pain to disappear overnight.
Yes, you can buy expensive collagen powders or gelatins and help pay for supplement company CEO’s boat. And, some of these have been shown to be effective in helping the skin.However, most of the stuff you find in the supermarket is so highly processed that it isn’t likely to deliver any benefits.
Many collagen supplements found in powders can also cause diarrhea, bloating, a sensation of heaviness in the gut and stomachache.
Instead, save your money. Consume slow cooked beef & pork, eggs, fish and/or cook with bone broth.It will do wonders for your hair, skin and nails and it tastes great.
Sadly, I’ve had patients over age 70 tell me “pneumonia is an old man’s best friend.” It is very true that pneumonia, the common cold, influenza and COVID-19 can all cause death in the older frail adult. This is not something new, though if you listen to CNN you may think death should never occur.
But, thousands of physicians and over 200 different journal articles within the last 11 months demonstrate that if you are treated with azithromycin and either hydroxychloroquine or ivermectin plus Zinc, Vitamin D, Niacin, Vitamin C and Melatonin, you improve your risk of survival of a COVID-19 infection by an additional 10-40%. 75% of those studies demonstrated significant improvement even when hydroxychloroquine was started late. Africa has a mortality rate (1.3 per 100,000) that is 100 percent lower than the US (120 per 100,000) because they have hydroxychloroquine available over-the-counter and many people take it “every Sunday” as preventative medication for malaria.
Mind you, these medications were never FDA approved for treatment with COVID-19. But, we as licensed physicians have the autonomy to use medication “off-label” as long as we have discussed the risks, side-effects and expectations of these medications and you are aware that they were never FDA approved.
I have treated hundreds of patients with these combinations with great success in my clinic over the last 11 months.
Yet, in the last two weeks Fry’s Pharmacies (Kroger Pharmacies) are now refusing to dispense hydroxychloroquine or ivermectin for any COVID related virus. Why? Because they can make a huge profit on the Experimental COVID-19 vaccine. Why dispense a generic medication when you can make twice the profit from a vaccine? However, this experimental vaccine’s effectiveness is still yet to be confirmed, and probably less effective on newer strains as stated by the Surgeon General this last week (https://news.yahoo.com/us-surgeon-general-covid-19-184157789.html).
In my opinion, this is malpractice on the part of Fry’s Pharmacy and malfeasance on the part of the pharmacist.
Until they issue a public apology to you and me, I recommending you and I stop using Fry’s Pharmacy all together. Any company that mandates the use of an Experimental Vaccine with a side effect profile experienced by up to 20% of those who receive it, and at the same time refuses to provide access to proven treatments overseen by a physician should not receive the business or the trust of the public. If your pharmacist refused to dispense these medications with a valid prescription from your doctor, please let me know.
The pharmacists claim they won’t dispense hydroxychloroquine or ivermectin “because the FDA has not approved their use for viral infections.” Yet, these drugs are safe enough to be over the counter in many other countries and because of the vaccine, this is all political. Both of these drugs have been use very safely for decades with millions of people around the world for multiple disease processes.
The FDA issued it’s updated statement on the use of ivermectin. “Ivermectin is an antiparasitic drug that is approved by the Food and Drug Administration (FDA) for the treatment of onchocerciasis and strongyloidiasis. Ivermectin is not FDA-approved for the treatment of any viral infection. In general, the drug is well tolerated. It is currently being evaluated as a potential treatment for COVID-19.” These drugs are considered “generally safe” for multiple disease processes used over long periods of time, and yet, the politics and finances of this issue have now become more important than your health. Neither the FDA or the NIH has stated that these drugs are contrindicated, they just have not been approved, and because of that “they are not recommended.”
As of January 14, 2021, the NIH has stated that ” currently there are insufficient data to recommend either for or against the use of ivermectin for the treatment of COVID-19. Results from adequately powered, well-designed, and well-conducted clinical trials are needed to provide more specific, evidence-based guidance on the role of ivermectin for the treatment of COVID-19.” Similar statements have been issued on hydroxychloroquine. However, “well conducted clinical trials” will not occur for some time, as these types of studies take years to be designed, funded and put into place. Because ivermectin and hydroxychloroquine are generic drugs, there is no incentive for any pharmaceutical company to run these types of studies. The FDA will never change it’s position for this same reason.
Any physician, organization or pharmacy that places politics and finances over your health and wellbeing and tries to get between the doctor and patient should experience you and I protesting with our wallets and our feet.
Two essential things come out of this. First, the CDC, FDA and NIH have shown us as a nation how untrustworthy they are. Second, if you and I are not vigilant, mandates for the use of an experimental and potentially dangerous vaccine will be come the “new normal.”
I recommend you go to https://stopmedicaldiscrimination.org/ and sign the petition to prevent travel companies, airlines and other businesses from mandating this and any other experimental vaccine. And, then tell Fry’s Pharmacy and any other pharmacist that plays politics with your health where they can put the rest of their medications.
Sources:
Kory P, et al., Review of the Emerging Evidence Demonstrating the Efficacy of Ivermectin in the Prophylaxis and Treatment of COVID-19. FLCCC Alliance; Version 5; Nov 28, 2020.
Rajter JC, et al. Use of Ivermectin is associated with lower mortality in hospitalized patients with corona-virus disease 2019. Chest Journal Open Access Jan 2021; 159(1): 85-92
Guilherme Dias de Melo, Françoise Lazarini, Florence Larrous, Lena Feige, Lauriane Kergoat, Agnes Marchio, Pascal Pineau, Marc Lecuit, Pierre-Marie Lledo, Jean-Pierre Changeux, Herve Bourhy, Anti-COVID-19 efficacy of ivermectin in the golden hamster. bioRxiv 2020.11.21.392639
Vora, Agam, et al. “White paper on Ivermectin as a potential therapy for COVID-19.” Indian Journal of Tuberculosis 67.3 (2020): 448-451.
Gorial, Faiq I., et al. “Effectiveness of Ivermectin as add-on Therapy in COVID-19 Management (Pilot Trial).” medRxiv (2020).
Scheim, David. “Ivermectin for COVID-19 Treatment: Clinical Response at Quasi-Threshold Doses Via Hypothesized Alleviation of CD147-Mediated Vascular Occlusion.” Available at SSRN 3636557 (2020)
Rajter, Juliana Cepelowicz, et al. “ICON (Ivermectin in COvid Nineteen) study: Use of Ivermectin is Associated with Lower Mortality in Hospitalized Patients with COVID19.” medRxiv (2020). medRxiv.org
Chowdhury, Abu Taiub Mohammed Mohiuddin, et al. “A comparative observational study on Ivermectin-Doxycycline and Hydroxychloroquine-Azithromycin therapy on COVID19 patients.” ResearchGate.net
NIH Statement on Ivermectin: https://www.covid19treatmentguidelines.nih.gov/statement-on-ivermectin/
FDA Statement on Ivermectin: https://www.fda.gov/animal-veterinary/product-safety-information/faq-covid-19-and-ivermectin-intended-animals
The following general measures are recommended to reduce transmission of infection:
Diligent hand washing, particularly after touching surfaces in public. Use of hand sanitizer that contains at least 60 percent alcohol is a reasonable alternative if the hands are not visibly dirty.
Respiratory hygiene (for example – covering the cough or sneeze).
Avoiding touching the face (in particular eyes, nose, and mouth).
Avoiding crowds (particularly in poorly ventilated spaces) if possible and avoiding close contact with ill individuals.
Cleaning and disinfecting objects and surfaces that are frequently touched. The CDC has issued guidance on disinfection in the home setting; a list of EPA-registered products can be found here.
Dr. Nally talks about each of these in his latest YouTube video below:
“Keep the carbs low and the fat high.”
—————————————————————-
For more information about any of the things mention above and in other videos, you can find the links below:
The keto misconceptions abound and this week is no different. A popular health website recently published an article warning people about the “dangers” of a ketogenic diet, including the keto-flu, kidney disease, gut bacteria, nutritional deficiency, bone health and low blood sugar. They claimed these dangers are “evidence based.” Dr. Nally very quickly debunks these dangers, explains how the naysayers “spin” the science and talks about why these misconceptions are false.
One of the common complaints that I see in my office is chronic numbness and tingling of the hands, fingers, feet & toes. There are multiple causes of these symptoms, but by far the most common cause in my practice is polyneuropathy caused by insulin resistance (hyperinsulinemia).
Before we dive into this particular type of nephropathy, it is important that we define a few terms. The terms “polyneuropathy,” “peripheral neuropathy,” and “neuropathy” are frequently used interchangeably, and although they can be easily confused, they are distinctly different.
Definitions
Polyneuropathy is a specific term that refers to a generalized sensation of tingling or numbness that uniformly affects many nerves at the peripheral sites (ends of the extremities like hands, fingers, lower legs, feet and toes).
Peripheral neuropathy is a less precise term. It is frequently used synonymously with polyneuropathy, but can also refer to any disorder of the peripheral nervous system. However, this term includes pain or numbness that radiates from nerve roots like “sciatica” of the leg and “brachial plexopathy” causing symptoms in one hand and/or arm (mononeuropathies).
Neuropathy, which again is frequently used interchangeably with peripheral neuropathy and/or polyneuropathy, can refer even more generally to disorders of the central (brain & spinal cord) and peripheral nervous system (nerves of the arms and legs) and their connections to sensory organs, such as the eye and ear, and to other organs of the body, muscles, blood vessels, and glands.
Why spend time defining all this? Because, neuropathy can be very confusing, even for the experienced physician. And, because I am seeing, more and more frequently, cases of insulin resistance induced polyneuropathy. The polyneuropathies must be distinguished from other diseases of the peripheral nervous system, including the mononeuropathies and mononeuropathy multiplex (multifocal neuropathy), and from disorders of the central nervous system.
Mononeuropathy refers to focused involvement of a single nerve, usually due to a localized trauma, compression, or nerve entrapment. Carpal tunnel syndrome is a common example of a mononeuropathy. Sciatica due to a lumbar disc bulge is another form of mononeuropathy.
Mononeuropathy multiplex refers to simultaneous involvement of non-adjoining sections of nerve trunks. Used loosely, this term can refer to multiple compressive mononeuropathies. However, in its more specific meaning, it identifies trauma, infection, auto-immunity or damage to multiple nerves outside the central nervous system. This is often due to lack of blood supply due to disease based inflammation of blood vessels supplying blood to these peripheral nerves.
Diseases of the central nervous system such as a brain tumor, stroke, or spinal cord lesion occasionally present with symptoms that are difficult to distinguish from polyneuropathy.
Insulin Resistance and Neuropathy
Insulin resistance, or better defined hyperinsulinemia, begins 10-15 years before a person is considered “pre-diabetic” and 20 years before the onset of type II diabetes. This “over production of insulin” in response to carbohydrates, starches and sugars causes a subtle and progressive form of inflammation. This excessive production of insulin will damage the smallest arteries (capillaries) carrying oxygen and fuel to the back of the eyes, the kidneys and the peripheral nerves of the hands, fingers, lower legs, feet and toes.
Often not identified until a person is actually diabetic, the mechanism underlying the development of this type of neuropathy is extremely complex. It is driven by years of subtle and progressive damage to the blood vessels, and inability of the nerves to use essential B vitamins damaging the genetics of the cell. This leads to inflammatory, metabolic, and ischemic effects causing the nerves to function poorly over time.
What Causes Polyneuropathy?
The mechanism of polyneuropathy damage in the patient with hyperinsulinemia three-fold.
The presence of high insulin stimulates increased fat storage. As fat cells begin to get filled, they begin to over-produce a number of inflammatory hormones including TNF-alpha, IL-6, IL-1, Adiponectin, Leptin and Resistin. These inflammatory hormones turn on auto-immunities and abnormal immune system function.
At the same time, the high insulin levels suppress appropriate testosterone and estrogen production causing microscopic damage to the lining of the smallest arteries and capillaries of the body (found predominantly at the extremities, kidneys and back of the eyes).
65% of patients with insulin resistance (hyperinsulinemia) have a malformation of one or both genes that encode the MTHFR enzyme (methylenetetrahydrofolate reductase) that uses folic acid (Vitamin B9) inside the cells of the body. Because this is genetic and is a process occurring inside the cell, it has been difficult to identify until recent advances in measuring genetic SNPs. Single nucleotide polymorphisms, frequently called SNPs (pronounced “snips”), are the most common type of genetic variation among people.
Interestingly, MTHFR deficiencies are also strongly correlated with depression, anxiety and other forms of mental illness. MTHFR is a SNP that can easily be tested through a simple blood sample at your local lab or doctors office. And, nerve testing can be done through a simple sudomotor function test in the doctors office. In fact, Medicare encourages this testing yearly through part of the Annual Wellness Exam.
The polyneuropathy that I see most commonly in my office can and will improve. In fact, polyneuropathy will completely resolve if you catch it early enough. We treat it in two ways.
What Can I Do To Treat Polyneuropathy?
First, restrict carbohydrate intake. A ketogenic or carnivore diet is the perfect approach to this. If you don’t have a copy of my book, The KetoCure, please pick one up on my website or on Amazon. if you are just looking to fine tune the nuts and bolts of your diet, you can get a copy of my diet recommendations here. Carbohydrate restriction corrects the high insulin levels. Within a few weeks, people start seeing improvement in inflammation, testosterone, estrogen and leptin resistance.
Second, get your MTHFR SNPs tested. This can be ordered through a simple blood test through your doctor or nearby lab. If you have one or both MTHFR mutations, treatment is simple. A mutation of the MTHFR SNP directly causes polyneuropathy, anxiety, depression and in severe cases, schizophrenia. It can also cause significant problems with homocysteine metabolism and is a significant risk factor in heart disease.
Third, use the correct form of folic acid. If you have the MTHFR mutation, regular folic acid is ineffective. Instead of using regular folic acid (Vitamin B9), 1000-5000mcg per day of L-methyl folate (premethylated Vitamin B9) solves the problem. Within 90 days, over 50% of my patients feel dramatic improvement in their neuropathy and many have compete resolution of the numbness and tingling. I see this so frequently, that a few years ago I had my multivitamins designed to include L-methyl folate instead of regular folic acid. You can find them here at Ketoliving. com. If you want more information on why I designed my own vitamin supplement a few years ago, you can read about them here.
So, restrict your carbs, use the appropriate form of folic acid for you, and pass the bacon!
If you are interested in getting more help on this issue, schedule an appointment with me in my office. Or, consider one of my membership options if seeing me in my office isn’t convenient for you. Sign up today!
References:
Yigit, Serbulent et al. “Association of MTHFR gene C677T mutation with diabetic peripheral neuropathy and diabetic retinopathy.” Molecular vision 19 1626-30. 25 Jul. 2013.
Wan, Lin et al. “Methylenetetrahydrofolate reductase and psychiatric diseases.” Translational psychiatry 8,1 242. 5 Nov. 2018, doi:10.1038/s41398-018-0276-6.
Shelton, Richard C et al. “Assessing Effects of l-Methylfolate in Depression Management: Results of a Real-World Patient Experience Trial.” The primary care companion for CNS disorders 15,4 (2013): PCC.13m01520. doi:10.4088/PCC.13m01520.
Hughes R. Investigation of peripheral neuropathy. BMJ 2010; 341:c6100.
Morrison B, Chaudhry V. Medication, toxic, and vitamin-related neuropathies. Continuum (Minneap Minn) 2012; 18:139.
Pareyson D, Piscosquito G, Moroni I, et al. Peripheral neuropathy in mitochondrial disorders. Lancet Neurol 2013; 12:1011.
Rutkove SB, et al., Overview of Polyneuropathy. UpToDate.com. Online Jan 2020, https://www.uptodate.com/contents/overview-of-polyneuropathy?search=neuropathy&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1
I’ve had many of my patients and followers on social media ask about my continued use of the hashtag #JustKeepEsterifying. Well, here is the answer. Check out the short 4 minute video below to get the answer:
What do you do when you hit a weight loss stall while living a ketogenic lifestyle? Find out below. Dr. Nally goes into detail on the multiple causes of stalling while following a low-carbohydrate or ketogenic lifestyle. He dispels the myths around counting calories and macros. And, he discussed the basics of overcoming a stall.
Rice is rice. Potato is a carbohydrate that will halt your weight loss and please do not bring me a bagle.
And, NO, I did not just give you permission to go eat a jelly donut!!
You’d be amazed at how many people don’t realized the carbohydrate content (sugar equivalents) of various foods that we’ve been told are “good for us.” Check out my youtube.com video here on eight steps to getting started with a ketogenic lifestyle.
The most common complaint that I get in my office when someone has started a ketogenic diet is, “Doc, I feel fatigued. Will this ever go away?”
That feeling of fatigue, some refer to as the “keto-flu,” is usually due to a couple of things. First, you may not be eating enough fat (I recommend a 1 gram to 1 gram ratio of protein to fat when getting started). Second, you’re not taking in enough salt (specifically sodium, potassium, magnesium and/or zinc). These four salts are essential electrolytes our body requires for proper function.
If salt is the problem, the you will be experiencing leg cramps. Cramps during daytime activity are usually due to low sodium or potassium levels. Cramps that wake you up at night are usually due to low magnesium or zinc. Leg cramps can also be due to hypothyroidism or significant blood sugar swings. Dr. Nally will usually check for this during your visit with him.
“But isn’t too much salt bad for you?” I am frequently asked.
Too much salt is only bad for you if you’re eating a “low-fat” diet.
What if increasing salt intake actually lowered your blood pressure?
Did you know that increasing your salt intake can actually improve your diabetic blood sugar if you are following a correct diet? Could it be that easy?
Almost every patient that I see in the office has a significant worry about salt intake, some greater than others. In fact, some people are so fearful about salt that when I initially began encouraging its use, they told me that I was crazy, and they left my practice.
Has restricting salt over the last 50 years really worked, or is it doing more damage than we think?
That was the question that was asked by Dr. Ames in the American Journal of Hypertension 17 years ago. However, his answer never got a mention. In fact, I’ve been in practice for almost 20 years, and incidentally stumbled upon this article when it was mentioned by a colleague of mine. Granted, the study is a small sample size of people, only twenty-one. However, the results are profound.
Twenty-one patients with hypertension were randomized to periods of no salt (placebo) and periods of 2 grams (2000 mg) of sodium chloride four times a day (a total of 8 grams of salt per day). Glucose tolerance tests were completed with insulin levels at the end of each intervention period.
Insulin Resistance and Hypertension Improve by Adding Salt
Three very noteworthy results happened. First, those patients with insulin resistance and diabetes had improvement in their glucose levels while on 2 grams of sodium supplementation.
Second, those with hypertension also, shockingly, showed improvement in their blood pressure while on the 2 grams of sodium supplementation.
Third, those with insulin resistance had a lowering of their insulin levels during the period of increased sodium intake. These findings fly in the face of the dogma that’s been drilled into our heads that “salt is bad!”
“But, Dr. Nally, you can’t base your findings on a small group of 21 people,” the experts say.
Yes, it is a small study group. However, these findings are identical to what I, also, see clinically every day in my practice for over 20 years.
We know that the average human needs at a minimum 3 grams of sodium per day and 3 grams of potassium per day. The standard American diet (SAD diet) including processed foods contains 2-3 grams per day of sodium and potassium. In fact, the CDC claims the worst salt containing meals for you are:
Bread
Processed chicken dinners
Pizza
Pasta
Insulin also stimulates additional retention of sodium at the kidney level. If you are insulin resistant, producing excess insulin in response to starches or sugars, you retain notably larger amounts of salt when eating the standard American diet (SAD diet) or a “low-fat” diet. However, if your following a low-carbohydrate or ketogenic lifestyle, you won’t be eating the meals above and you’re probably not getting near enough salt.
Salts, or electrolytes, are essential in normal cellular function. Low salt in the body is like running your car without oil. It will run, but not very efficiently and over the long term will cause problems. This is the cause of the keto-flu I wrote about previously. And, according to the study above, it is a potential driver of our persisting insulin resistance, diabetes and hypertension.
How Much Salt Should I Use?
In my office, I encourage use of 3-4 grams of sodium and 3-4 grams of potassium daily when using a ketogenic lifestyle. That’s approximately 1 ½ – 2 teaspoons of salt per day. I like the Redmond’s RealSalt or pink Himalayan salt because these products contains all four types of salt (sodium, potassium, magnesium and zinc).
It is probably that your salt restrictions is making your insulin resistance and blood pressure worse. That’s what the clinical evidences are pointing toward, and it is what I see every day in my office.
Want to know more about a ketogenic life-style? Click the KetoLife link to get some basics.
If you’re already following a ketogenic lifestyle, then let me help you navigate the bumps and turns by going to the KetoKart and checking out the products I recommend to jump-start ketosis DocMuscles-style!
Until then, I’ll have another piece of bacon, please . . . and, oh, pass the salt!
Will a ketogenic diet or very low carbohydrate diet kill you? Will it increase your likelyhood of death? That’s what the media and the dietary world is saying this week. Is it really true? How do you know? That’s the question that I ponder as I smoke my brisket while reading the headlines this week.
My inbox has exploded with patients and acquaintances suddenly worried that my very low-carb lifestyle is bad. This all revolves around the publishing of a study in the Lancet this week, and the interpretative spin that has been placed on it by “those in the know.” To quote one of the NHS dietitians, Catherine Collins, RD FBDA, “In summary, this paper will disappoint those who, from professional experience, will continue to defend their low-carb cult, but contributes to the overwhelming body of evidence that supports a balanced approach to calorie intake recommended globally by public health bodies.” Either she didn’t actually read the paper, or she clearly doesn’t understand the low-carbohydrate/ketogenic dietary world. Before you go throwing out your bacon, turning off my smoker and buying bags of rice, let’s talk about some principles that seem to be completely misunderstood by the “low-fat, calorie restricting” nutritional aristocracy.
Ketogenic Diets are Powerfully Effective
First, ketogenic diets are powerfully effective. They are effective in weight loss, reduction of blood sugar, reversal of diabetes, decreasing cardiovascular risk and reduction in blood pressure. These are just a few of the powerful effects of a ketogenic lifestyle. (I wrote a whole book on the 16 different diseases dramatically improved by carbohydrate restriction.) It’s why I’ve been using carbohydrate restriction for over 14 years both personally and in my clinical practice. 85% of the people in my practice don’t respond effectively to anything other than carbohydrate restriction. This is because their insulin levels are 2-20 times normal. The question the Lancet should be asking is “why do 85% of people fail calorie restriction?” But, that is for another article.
Few Diets Keep the Weight Off Long-Term
Does the ketogenic diet keep weight off in the long term? All diets seem to fail in this regard, even the ketogenic diet will show rebounding of weight after 1-2 years. Yes, I hate to be the bearer of sour news, but as an obesity specialist, this is what I do for a living. The Lancet article implies that the low-carb diet is singular in the issue of weight rebound, but that is not the case. The only diet I have found to effectively keep the weight off long-term is a ketogenic diet, combined with pulsed eating and the correct type of physical activity.
Definition of a Very Low-Carbohydrate Diet
Third, commentary, and the researchers themselves, extrapolate that based on the results, very low carbohydrate diets increase the risk of mortality. However, this study wasn’t even “low-carb.” It was Paleolithic at best. The lowest calorie intake group was just under 1600 kcal per day and the carbohydrate restriction was only 120 grams per day. A low-carb diet is defined as less than 100 grams per day. A very low-carbohydrate diet is defined as less than 50 grams per day, and a ketogenic diet is defined as less than 20 grams per day. This study and the cohort studies involved in it weren’t even low-carb!!!
Only Two Data Gathering Points in 25 Years?
Fourth, although people were followed for 25 years, there were only two data gathering points consisting of 66 questions spaced 5-7 years apart asking the 15,428 participants to “remember what they ate” over previous 3-5-year intervals. Seriously?! I can barely remember what I ate last week and I take pictures of my food and journal my meals frequently. How can you publish an article with only two data collection points over 25 years? And, how can extrapolated data over 25 years be accepted as valid in a premier medical journal? It is beyond my understanding.
You Gotta Lower Insulin to Reduce Mortality
Fifth, insulin must be lowered to a “baseline level.” Increasing fat intake in the presence of abnormally elevated insulin will actually increase risk of cardiovascular disease, peripheral vascular disease, diabetes, hypertension, gout, kidney stones, and death by multiple causes. This cohort of people only partially lowered carbohydrate intake, and raised fat and or protein intake. Those of us who’ve been treating obesity and practicing in the trenches are well aware that if you don’t bring the insulin levels under control, raising fat and protein is just a ticking time bomb. Of course, the all-cause mortality went up in this group. I’d expect nothing less. This is what I saw with a large portion of my Paleolithic dietary patients.
This is also why caloric restriction doesn’t work. These participants had average calorie restriction of 1600-1800 kcal per day. Yet their risk for all-cause mortality (death by all causes) increased.
Weight Gain Continued
Sixth, all of the groups continued to gain weight. Body mass index increased by almost a full point ever 6 years. Carbohydrates were NOT restricted enough to be effective. It also, demonstrates another example of calorie restriction failure in 15,000 plus people.
That’s what I’d call successful – not really!
Smokers Not Excluded
To make matters worse, 60-70% of the population were smokers or former smokers and this study did not specifically eliminate this as a risk factor for all-cause mortality. We know that smoking dramatically increases risk of heart disease, peripheral vascular disease, hypertension, stroke, lung cancer, chronic obstructive pulmonary disease, etc. The contribution of tobacco in this cohort was not adequately isolated.
The World Health Organization has developed sixteen goals as their “Call to Arms.” Goals 12 and 13 specifically discuss “ensuring sustainable food consumption patterns throughout the world.” These goals specifically outline a transformational vision of the world. This will occur by “doubling agricultural growth” and restricting food production that worsens the “carbon footprint.”
Really?!
Over the last ten years, multiple progressive groups and sites have made the claim that the greatest threat to Climate Change is the cattle industry. They link cattle, livestock and our consumption of red meats to global warming and have been preaching the politics of nutrition. They claim that the only real way to stop climate change and global warming is to “eat less red meat and dairy products.”
Low-carbohydrate and ketogenic diets are a threat to this transformational vision. Because of this, we will likely see more and more scientific research used as propaganda, let’s call it what it is, to sway the general populous in their buying and eating patterns.
So, if you’ll excuse me, my smoked brisket is ready to pull off the smoker. . .
Over fifty years of data have demonstrated that creating energy deficit through the reduction in caloric intake is effective in reducing weight. . . However, it is only for the short term (1, 2). The biggest challenge physicians face in the treatment of obesity is that calorie restriction fails when it comes to long-term weight loss.
Isn’t Fasting Effective in Long-Term Weight Loss?
With the craze and popularity of intermittent fasting, some have claimed that intermittent fasting is more effective in weight reduction. Recent results demonstrate that this may also be incorrect. In the short term evaluation of caloric restriction and intermittent fasting, reduction in 15-20 lbs of weight is effectively seen and the highly publicized Biggest Loser’s losing ~ 120 lbs. Intermittent fasting and alternate day fasting have been shown to be more effective in lowering insulin levels and other inflammatory markers in the short term.
There is, however, controversy over maintaining weight loss beyond 12 months in the calorie restriction, intermittent and alternate day fasting groups. Forty different studies in a recent literature review, thirty-one of those studies looking at forms of intermittent fasting, demonstrate that the majority of people regain the weight within the first 12 months of attempting to maintain weight loss(3, 5). This is, also, what I have seen for over 18 years of medical practice.
Is Calorie Restriction the Only Way to Lose Fat?
Numerous “experts” claim that the only way to reduce fat is “caloric deficit.” Variations through the use of intermittent, long-term or alternate day fasts can be found all over the internet. In regards to calorie restriction, these “experts” with nothing more than a personal experience and a blog to back their claims preach this louder than the “televangelists” preach religion. Based on the faith that many place in this dogma, it could be a religion. What causes belief in this dogma is that weight and fat loss actually does occur with caloric restriction to a point. The average person will lose 20-25 lbs, however, within 12 months of achieving this goal, most people regain all the weight. (No one ever mentions the almost universal problem with long-term weight loss, especially those “experts.”)
Prolonged calorie restricted fasts, intermittent fasts, and alternate day fasts are often grouped together into the fasting approach, causing significant confusion among those that I speak to and counsel in my office. There is great data that alternate day fasts do not have the reduction in resting energy expenditure that prolonged fasting, intermittent fasting and calorie restriction cause. However, none of these approaches appears to solve the problem of weight re-gain after long-term (12-24 months into maintenance) weight loss (3). And, a recent study of 100 men participating in alternate day fasting showed that there was a 38% dropout rate, implying that without close supervision and direction, maintenance of this lifestyle is not feasible for over 1/3rd of those attempting it.
Long-Term Weight Loss Failure Brings Tears
Failure on calorie restricted diets, low fat diets, and intermittent fasting diets with weight regain at twelve to twenty-four months is the most common reason people end up in my office in tears. They’ve fasted, starved themselves, calorie restricted, tried every form of exercise, and still regained the weight. Trainers, coaches and “experts” have belittled them for “cheating” or just not keeping to the diet. Yet, we know that calorie restriction and intermittent fasting cause a rebound in leptin, amilyn, peptid YY, cholecystikinin, insulin, ghrelin, gastric inhibitory peptide and pancreatic poly peptide by twelve months causing ineffective long-term weight loss (6). The dramatic rise in these hormones stimulates tremendous hunger, especially from ghrelin and leptin.
N Eng J Med 27 Oct 2011. Mean (±SE) Fasting and Postprandial Levels of Ghrelin, Peptide YY, Amylin, and Cholecystokinin (CCK) at Baseline, 10 Weeks, and 62 Weeks.
Although less problematic in alternate day fasting, these calorie restricted approaches also cause dramatic slowing of the metabolism at the twelve month mark. In many cases, the metabolic rate never actually returns to baseline, creating even more difficulty in losing further weight or even maintaining weight (6).
N Engl J Med 27 Oct 2011. Mean changes is weight from 0 – 62 weeks.
Is Gastric Bypass or Gastric Sleeve the Solution?
Gastric bypass and the gastric sleeve procedures have been touted as the solution to this problem, as they decrease ghrelin, however, 5-10 years later, these patients are also back in my office. They find that 5-10 years after these procedures the weight returns, cholesterol and blood pressure rise, and diabetes returns. These hormones kick into high gear, stimulating hunger in the face of a slowed metabolism, that to date, has been the driver for weight regain in the majority of people. People find it nearly impossible to overcome the hunger. You may have experienced this, I know I have.
It’s the Hormones, Baby!
So, what is the answer? It’s the hormones. (WARNING – You’ll hear that when your wife is pregnant, too, gentlemen). We are hormonal beings, both in weight gain, and in pregnancy. Trying to preach calorie control to a hormonal being is like showing up at the brothel to baptize the staff. You might get them into the water, but you’re probably not getting them returning weekly to church or pay a tithe.
So, how do you manipulate the hormones in a way to control the rebounding hunger and suppression of metabolism? This is where we put a bit of twist on the knowledge we’ve gained from alternate day fasting. Recent research shows that “mild” energy deficit in a pulsatile manner, that has the ability to mimicking the body’s normal bio-rhythm’s is dramatically effective in reducing weight and maintaining normal hormonal function without cause of rebound metabolic slowing (4).
Pulsed Mild Energy Restriction
What does this mean in layman’s terms? It means that if we provide a diet that maintains satiety hormones while providing a period of baseline total energy expenditure needs and a period of mildly reduce caloric intake in a pulsed or cyclic manner, greater weight loss occurs and there is no rebound of weight 1-2 years later.
The main reason I’ve not jumped on the intermittent fasting band wagon is the shift in leptin, amylin, ghrelin and GLP-1 signaling that regularly occurs at the 6-12 month mark. The rebound of these hormones causes weight re-gain and is what prevents successful long-term weight loss. A number of people come to my office and tell me they couldn’t follow a ketogenic diet, so they’re doing intermittent fasting and it works . . . for a while. Then, they end up in my office having hit a plateau or fallen off the wagon and regained all the weight. They are completely confused and don’t understand what happned. Most of them are convinced it’s their thyroid or cortisol and they’ve seen every naturopath and functional medicine doctor in town.
What people really need is a simple approach to long-term weight loss without having to spend the night in the physiology lab every two weeks sleeping under a ventilated hood system.
The Ketogenic Lifestyle is a Pulsed Energy Lifestyle
Third, providing adequate fat is the simple way to maintain leptin, ghrelin, amylin, GLP-1 (among the others) and long-term weight loss. Can you eat too much fat? Of course you can. But, because each of us have differing levels of stress and activity each day, this fat intake becomes the lever for hunger control.
Fourth, the use of exogenous ketones ensures easily accessible ketone (short chain fatty acids) to modulate adipose (white fat) signaling of the liver without large caloric intake through the portal vein by first pass of liver metabolism. The ketones also help stabilize the gut bacteria. The combination of hormone balance between the liver and fat cells and improvement of gut bacteria suppresses key hunger hormones and aids glucose regulation between the fatty tissues and the liver. Ketones, both endogenous and exogenous, suppress production of TNF-alpha, IL-6, resistin, and stabilize production of adiponectin and leptin from the adipose cells (7, 8, 9).
In my office, once we calculate the basic protein needs daily, we start with a 1:1 ratio of protein to fat. Then, the fat is adjusted up or down based on hunger. Remember, hunger occurs, because your body produces hormones. The addition of fat to a diet that is not stimulating large amounts of insulin resets the hormone patterns back to normal without causing weight gain.
Give Obese People Fat Ad Libitum?
“Sure, Dr. Nally, but what about those people who don’t know if they are hungry, bored, stressed or just have a bacon fixation? You can’t just give them all the fat they want?!”
Why not? Implying that people aren’t smart enough to know when they are full is a bit of a fascist philosophy, don’t you think?
Do people over eat? Sure they do. But, I’ve found that when you give people an antidote to hunger (using fat intake in the presence of stabilized insulin levels) over a few months, people begin to recognize true hunger from other forms of cravings. This is especially true when they keep a diet journal. This gives people the ability to begin listening to their own bodies, responding accordingly and governing their stress, eating, exercise and activity. Keeping a diet journal is key to long-term weight loss. And, isn’t helping people use their own agency to improve their health really what we’re trying to do?
Interestingly, doing this over the years seems to line up with the findings of this year’s MATADOR study in the International Journal of Obesity. They found that mild intermittent energy restriction of about 30-33% for two weeks, then interrupting this with two weeks of a diet that was energy balanced for needs improved both short and long-term weight loss efficiency (4). In looking at my, and my patient’s diet journals, this energy restriction of about 1/3 of needed calories cyclically seems to happens naturally with a ketogenic lifestyle, without even counting calories. (Calories are a swear-word in my office).
What does the correct long-term wight loss program look like in a diet or meal plan? Well, you’ll have to join the Ketogenic Lifestyle 101 Course to see what that really means to you individually. I look forward to seeing you there.
Want to find out more about the Ketogenic Lifestyle 101 course? CLICK HERE.
Have you read my book The Keto Cure? Get a signed copy from me by clicking HERE.
References:
Bronson FH, Marsteller FA. “Effect of short-term food deprivation on reproduction in female mice.” Biol Reprod. Oct 1985; 33(3): 660-7. https://www.ncbi.nlm.nih.gov/pubmed/4052528?dopt=Abstract&holding=npg
Connors JM, DeVito WJ, Hedge GA. “Effects of food deprivation on the feedback regulation of the hypothalamic-pituitary-thyroid axis of the rat.” Endocrinology. Sep 1985. 117(3): 900-6. https://www.ncbi.nlm.nih.gov/pubmed/3926471?dopt=Abstract&holding=npg
Seimon RV, Roekenes JA, Zibellini J, Zhu B, Gibson AA, Hills AP, Wood RE, King NA, Byrne NM, Sainsbury A. “Do intermittent diets provide physiological beneftis over continuous diets for weight loss? A systematic review of clinical trials.” Mol Cell Endo. 15 Dec 2015. 418(2): 153-172. https://www.sciencedirect.com/science/article/pii/S0303720715300800
Byrne NM, Sainsbury A, King NA, Hills AP, Wood RE. “Intermittent energy restriction improves weight loss efficiency in obese men: the MATADOR study.” Int J Obes. 2018. 42:129-138. https://www.nature.com/articles/ijo2017206
Trepanowski JF, Kroeger CM, Barnosky A. “Effect of Alternate-Day Fasting on Weight Loss, Weight Maintenance, and Cardioprotection Among Metabolically Healthy Obese Adults.” JAMA Intern Med. Jul 2017. 177(7): 930-938. https://jamanetwork.com/journals/jamainternalmedicine/article-abstract/2623528?redirect=true
Sumithran P, Prendergast LA, Delbridge E, Purcell K, Shulkes A, Kriketos A, Proietto J. “Long-term persistence of hormonal adaptations to weight loss.” N Engl J Med. 27 Oct 2011. 365: 1597-1604. http://www.nejm.org/doi/full/10.1056/NEJMoa1105816
Asrih M et al., “Ketogenic diet impairs FGF21 signaling and promotes differential inflammatory responses in the liver and white adipose tissue.” PlosOne. 14 May 2015. Open Access. https://doi.org/10.1371/journal.pone.0126364
Veniant MM et al. “FGF21 promotes metabolic homeostasis via white adipose and leptin in mice.” PlosOne. Jul 2012. Open access. https://doi.org/10.1371/journal.pone.0040164
Whittle AJ, “FGF21 conducts a metabolic orchestra and fat is a key player.” Endocrinology. 1 May2016. 157(5): 1722-1724.
In my last blog post about willpower, I described habits being neural impulse channels in our brain stimulated by a cue following a path leading to the same outcome each and every time – without exerting much effort. Researchers call the formation of these impulse channels habit-loop cycles. Much of the original obesity research of the 19th century was conducted by psychiatrists and psychologists recognizing that people had habitual eating patterns. Because of this, gluttony became the perceived influence of obesity. This underlying philosophy still permeates the obesity research, treatment and low-carb dietary world today. Yet, over the last 15 years, I’ve found that the habit-loop cycle is tied to powerful hormone responses. These responses to very subtle and often unknown triggers or cues powerfully drive weight gain, obesity and struggles with willpower. How does the habit-loop cycle effect you? Before we can change these habit-loop cycles, we have to understand what they are, and how they were created.
It’s All About That Basal Ganglia
Meghan Trainor tells us that “It’s all about that bass . . .” However, it’s really all about that basal ganglia. Deep inside our brains, close to the brain stem, at the location where the brain meets the spinal cord, is a little “nub” of neurological tissue called the basal ganglia. This little nubbin of tissues was identified by the really smart scientists at MIT in the 1990’s as the location where habits are formed and executed. The brain is – to take a quote from my favorite ogre, Shrek – “like an onion – it has layers!”
The Brain Is Like an Onion
If you picture the outer layers of the brain tissue, those closest to the hair and scalp, you can create a mental image of where our most complex thoughts occur. When you think up a new invention, create a new way to cook with bacon, laugh at a friend’s joke, or link two complex thoughts about how habits form, you are using these outer layers of the brain.
Like an Onion – It Has Layers! (DreamWork’s Shrek, 2001)
However, our interest today is deeper . . . much, much deeper. Deep within the center of the brain at the basal ganglia is the location where our automatic behavior originates. Swallowing, breathing and the startle responses are housed in this little nubbin of brain tissue. It is this area of the brain that learns to recall and record patterns of neurological thought and stimulating action. This part of the brain has the ability, like the water drops on the mound we discussed last week, to record neural pathways and tracks leading to reduced mental effort and habit. The basal ganglia even has the ability to store habits while the rest of the brain is asleep. It is in this location, the basal ganglia, where the habit-loop cycle occurs.
Habits Created by Chunking
The habit-loop cycle is the process where the brain converts a sequence of actions into an automatic routine. The really smart guys at MIT call this “chunking,” and it is the root of habit formation. There are hundreds of behavioral chunking activities that you and I rely upon every day. Some of these are as simple as the process you use to squirt toothpaste on your toothbrush before brushing your teeth. Others are more complex like getting dressed or making a lunch box for the kids.
The Habit-Loop Cycle in Your Car
A habit-loop cycle is performed by this little nubbin of tissue by millions of people every morning. Take, for example, backing your car out of the garage. When you first learned to do this, it required huge amounts of concentration – and for very good reason. You’re steering 3000-5000 lbs of steel between a 16 foot garage-door opening into oncoming traffic.
Safely backing your car requires you to open the garage door, unlock the car, adjust the seat, insert the key into the ignition, turn it clockwise, move the rear-view mirror and the side mirrors to visualize any obstacles, put your foot on the brake, put the car into reverse, gently remove your foot from the brake, mentally estimate the distance between the garage and the street while keeping the wheels straight and looking over your shoulder, applying a slight pressure between the gas pedal and the brake, and in some cases, slapping your teenagers hand while they fiddle with the radio dial.
But think about it . . . did you actually put any thought into these actions this morning? You and I probably did this once or twice today without any additional thought. It happened because the basal ganglia took over and created a habit-loop out of it. This routine, repeated hundreds of times, became a habit, requiring very little mental effort.
Your Basal Ganglia Makes You Fat
The habit-loop cycle occurs hundreds and maybe thousands of times throughout our day. It is the cycle that drives hundreds of our activities. In fact, it is this same cycle, in combination with 30 different hormones, that drives our weight gain or weight loss. Yes, I said it,your basal ganglia can make you fat.
Habits Make for a Smaller Brain
Your brain will try to turn any regular routine into a habit, because habits allow our minds to slow down and conserve effort, energy and fuel. The efficient brain allows us to stop thinking about basic behaviors like walking, breathing and eating. This effort-saving effect of the brain is a major advantage, otherwise our brains would be huge, requiring heads the size of watermelons, or even the size of a water tower, causing their own weather systems. Your wife will thank you for an efficient brain that is smaller and requires less room. Can you imaging giving birth to a watermelon or a small Chevy? (Did you notice the size of Shrek and the Donkey’s head? Just say’n . . . )
Habits Are The Root of Behavior
What all this leads to is this – habits, as much as memory and reason, are the root of our behavior. We often don’t remember the experiences that create our habits. However, once they are created, they influence our action without our own realization. Charles Duhigg’s book, The Power of Habit is a great resource for further information on how habits drive our behavior.
The Habit-Loop of Obesity
So, how does all this affect obesity and weight gain? Let’s, first, look at the habit-loop cycle. Researcher, Larry Squire, documented the habit-loop through three decades of research. He and others published numerous articles showing that habits have a cue or trigger that stimulates a routine. The routine leads to an outcome or reward. The reward usually satisfies a craving. Cue-> Routine -> Reward. What we learn through our studies in obesity is that the reward often stimulates a hormonal response of 1-30 different hormones in brain and body leading to repeat cues or triggers. The cravings are hormonally driven. I call it the Habit-Loop of Obesity.
The Craving is the Key
Human psychology and emotion is the key behind habit creation. First, there must be a trigger or cue. Second, the trigger is attached to a previously experienced emotion or craving tied to the cue. The key to habit formation is the craving. The craving is what stimulates the physical routine to occur. It is an emotion or craving that drives the brain to create the habit. Third, there must be a clearly defined outcome or reward that satisfy the emotion or the craving. The emotion or craving doesn’t have to be associated with hormones, however, in the relm of obesity, it is usually tied together.
I am all about making things easier. Your brain does it. We all do it. And, I’m all about trying to help you lose fat and get healthy more easily. Let food be your medicine, let medicine be your food. That’s my mantra and that is as easy and natural as it gets. But, in our day and age, we don’t always have access to growing and raising our own food. That’s why my second mantra is – better living through chemistry. So, I created the KetoKart. Over the last 15 years of medical practice, I’ve found products and supplements that aid in letting food be your medicine, changing triggers, modifying hormones, and help to satisfy cravings in a healthy way to make your decisions easier. Go to the KetoKart, see which package works for you and order it. You’ll thank me.
How do we change our obesity habits? Stay tuned for the third part in this series: Fixing the Habit-Loop of Obesity.
So, I want to know . . . which package did you choose?
Pre-order your copy of my new book that will be available on September 26, 2017.
The ketogenic diet isn’t just a great tool for helping people lose weight and feel their best; it’s also an extremely effective method for treating the common “diseases of civilization.” The Keto Cure will give readers the prescription they need to heal their bodies by eating plenty of fat and moderating protein and carbs.
I’ve been advocating a low-carb, high-fat diet in my clinical practice for over fifteen years, helping people address their health problems by making better food choices. I teamed up with bestselling low-carb author and podcaster Jimmy Moore to create a top-50 health podcast espousing the benefits of eating keto. Now, for the first time, I’ve taken my years of clinical experience, put everything down on paper, and create a how-to guide that details all the ways in which the ketogenic diet can help remedy common ailments.
The Keto Cure details the science behind the keto diet’s effectiveness at treating a wide range of diseases, including:
Alzheimer’s
Epilepsy
Fatty liver disease
Hypercholesterolemia
Hypertension
Parkinson’s disease
Thyroiditis
Type 2 diabetes
and many more
The Keto Cure also outlines practical tips gleaned from Dr. Nally’s fifteen-plus years in medical practice, as well as Moore’s ten-plus years as a health and wellness podcaster, on overcoming the common pitfalls that people experience when adapting to a high-fat way of eating, including fatigue and keto flu. This helpful information, combined with a wide variety of delicious keto recipes from international bestselling cookbook author Maria Emmerich, makes The Keto Cure a complete resource for healing oneself with the ketogenic diet.
How does ketosis help the diseases of civilization? Find out as Dr. Nally answers these and many other pertinent dietary questions this evening.
You can learn more about his multi-vitamin supplement he designed for insulin resistance/diabetic/weight management patients that he mentions in the video here at KetoLiving.com.
You can learn about exogenous ketones that he mentions helps to augment ketosis here at DymaicKetones.com.
Watch as we talk about how insulin stimulates the Na-K-ATPase pump leading to increased leg edema, varicose veins, bloating, hypertension and swelling. I see it all the time. Watch the video to find out why.
Watch further as I, Dr. Nally, answer some of the very common misconceptions and confusing factors about the ketogenic lifestyle, ketosis, supplements and exogenous ketones. Enjoy!!
I am frequently asked about the sweeteners that can be used with a low carbohydrate diet. There are a number of sweeteners available that are used in “LowCarb” pre-processed foods like shakes or bars, or in cooking as alternatives to sugar. However, most of them raise insulin levels without raising blood sugar and are not appropriate for use with a true low-carbohydrate/ketogenic diet. You can see and print the article I published clarifying which sweeteners you can use and which ones to avoid here:
Of recent note, I’ve been asked about the insulin response that occurs in the study found here quoted by Dr. Jason Fung in his wonderful book, The Obesity Code.
First, it is essential to note that both the crystalline form of Stevia and the aspartame used in the form of Equal, also a crystal, contain either dextrose or malto-dextrin as the crystallizing agent. Both dextrose and malto-dextrin have a known insulin spike equal to table sugar. You can see that in my article link above. Watch the video and we’ll discuss which forms of Stevia and aspartame don’t raise insulin in myself or my patients.
Aspartame has been effective in appetite suppression in many obesity patients clinically. However, recent studies have demonstrated that aspartame does have a negative effect on gut flora, has potential to cause insulin resistance to persist when used long term (seen in animal studies) and has been shown to damage the mitochondria of brain cells (also animal studies). I now caution my patients with its use. We will keep a very close eye on all these sweeteners.
Be warned, a ketogenic diet may cause pregnancy . . . !
Infertility and poly-cystic ovarian syndrome (PCOS) is a common occurrence in women with insulin resistance, pre-diabetes and diabetes. When treated with a ketogenic lifestyle, these symptoms often improve dramatically, and in fact, I’ve had a number of women in my medical practice, previously unable to conceive due to PCOS, get pregnant after changing to a ketogenic diet.
As I reviewed my website recently, I realized that I have posted lots of science but I’ve never posted any success stories. So, as patient’s are comfortable & willing to share, I will begin posting these experiences here on the blogosphere for the world to witness their successes and the power of the KetoDynamic Antidote.
The first success story is my own. This picture of me and my wife, were taken after I had been following a ketogenic lifestyle for about 4 years. I dropped 60 lbs, normalized my cholesterol and blood sugar also normalized. I couldn’t and wouldn’t recommend these lifestyle changes unless I was willing to follow them for the long haul myself. I call people following a ketogenic lifestyle for longer than a year “Ketonians.”
Not only mine, but hundreds of patient’s having similar successes have become the greatest reward to my career as a physician over the last 15 years. They are truly the “KetoDynamic Moments” that etch themselves into my memory and have made me such an advocate of a ketogenic lifestyle. Therefore, it is with great honor and excitement that I have been allowed to share Michelle’s story below.
Michelle started seeing me in October 2015. She has struggled with weight all her life and, now in her late 40’s, weighed 201 lbs with a waist circumference of almost 36 inches and a body mass index of 32. Her “before” picture was taken just before a Halloween activity in 2015. Her “after” picture was taken in late March 2016.
A simple ketogenic lifestyle change ( <20g of carbohydrates, moderate protein for her ideal body weight & increasing fat to > 60% of total calories) has produced almost 50 lbs of weight loss and 6 inches off her waist in just 5 months. This was with dietary change only (Michelle doesn’t exercise) and she’s still losing weight. What is dramatic, and I see it every day, is that Michelle looks younger by at least 10 years (she actually added 20 years to her life span with this weight loss already). She feels fantastic. Blood sugar and cholesterol are now under control and she has tremendous amounts of energy. Her picture in March is at a body mass index of 29.
Michelle doesn’t calorie restrict. She just eats until she is full. Congratulations, Michelle!!! And, keep up the great work.
If you’d like to share your KetoDynamic successes with me and my audience, please let me know.
Ketogenic Lifestyle Rule #2: Life Begins at the Edge of Your Comfort Zone
We have been taught for over 50 years that the minimum carbohydrate intake necessary to maintain health is 130 grams per day, with the average diet of 2000 calories per day containing around 300 grams per day based on 1977 recommendations that 55-60% of are dietary intake should come from carbohydrates. This value was initially established during World War II by a committee of scientists tasked with determining dietary changes that might effect national defense (1). These “guidelines,” originally called the Recommended Daily Allowances (RDA) and accepted by many as the gospel truth, have been modified every ten years and in 1997 changed to the Dietary Reference Intake (DRI). However, the recommended carbohydrate values have not changed other than “avoiding added sugars” in the most recent 2015 recommendations.
In light of the fact that there are NO actual diseases caused by lack of carbohydrate intake, most dietitians and physicians still preach the carbohydrate dogma originally outlined by the RDA. I say dogma, because these recommendations are based on a diet that vilifies fat, particularly animal fat like red meat. Say the words “red meat” around a dietician these days you’d think Voldemort (“He Who Shall Not Be Named”) had returned.
I bring up the carbohydrate quandary because it is a question that I am asked every single day. The question that seems to be asked of me, more and more, is what exactly is a carbohydrate?
Let’s make it simple. There are really only three types of carbohydrates:
Sugar
Starch (known as complex carbohydrates)
Fiber
Let’s start with Sugar. The simple form of carbohydrates, and the form that spikes your blood sugar and insulin rapidly, are called mono-saccharides (glucose, galactose, fructose & xylose). When two of these mono-saccharides are bound together they form disaccharides like sucrose, also known as “table sugar” (glucose + fructose), lactose found in milk (glucose + galactose), and maltose found in cereals and sweet potatoes (glucose + glucose).
Milk Sugar or Lactose (glucose + glucose)
The simple monosaccharides or disaccharides are easy broken into their mono-saccharide form in the blood stream and require the body to produce insulin to be used. The person with insulin resistance, impaired fasting glucose or type II diabetes often produces 2-10 times the normal amount of insulin to correctly use these mono-saccharides (see why this is a problem in: The Dreaded Seven: Seven Detrimental Things Caused By High Insulin Levels). Remember, fruit is also simple sugar containing the mono-saccharide fructose . . . which we call “natures candy” in my office.
“Yea, I know sugar is bad for me, but Dr. Nally, I just eat the good starches.”
If I had a nickel for every time I’ve herd that phrase . . .
We’ve become comfortable with shunning fat and “simple sugar,” but in the process we’ve been eating more “good starch.” But the “good starches” are also saccharides – just in longer chains of more than three glucose molecules bound together. Our gut easily breaks the bonds between the glucose links and turns these starches into mono-saccharides to be used as fuel. It takes a bit longer than the simple sugars above, so the release of insulin is slower (which is why it has a better glycemic index score), but whether you produce the insulin in the first hour or the second hour after eating it, insulin is still insulin. In the case of insulin resistance, the damage is still done.
These good starches make up “comfort food” like bread, rice, pasta, potatoes, corn, grains & oats. To the patient with insulin resistance, impaired fasting glucose or type II diabetes, the higher insulin response stimulates increased weight gain, rise in cholesterol, shift in hormone function and progression of atherosclerosis (vascular and heart disease). See the recent article on Why Your Oatmeal is Killing Your Libedo.
What about “resistance starches?” These are still starches and I am finding clinically that they still cause a rise in insulin and push people out of ketosis (See Common Ketosis Killers).
Finally, Fiber. Fiber is a carbohydrate, however, it is the indigestible part of the plant. Fiber has double bonds between the saccharides that human gastrointestinal tracts cannot digest. In most cases, fiber passes right through the intestines without being digested. It actually acts like a broom for your colon, helping the intestines to move nutrients through the system. This is why I recommend 1-2 leafy green salads a day for most patient’s following ketogenic diet. Fiber does help to promote bowel function.
The Leafy Greens
Fruit, non-green vegetables, pasta, grains and breads do contain good sources of fiber, however, these foods also have absorbable starches making them problematic as noted above.
The take home message is this, the use of starch or simple carbohydrate will be problematic for weight loss, cholesterol control, blood sugar control or blood pressure control in a patient with insulin resistance.
Therefore, the ketogenic lifestyle truly begins at the end of your comfort zone.
I am frequently asked about the sweeteners that can be used with a low carbohydrate diet. There are a number of sweeteners available that are used in “LowCarb” pre-processed foods like shakes or bars, or in cooking as alternatives to sugar; however, many of them raise insulin levels without raising blood sugar and are not appropriate for use with a true low-carbohydrate/ketogenic diet. You can see and print the article I published clarifying which sweeteners you can use and which ones to avoid in the menu bar above “Sour Truth About Sweeteners” and you can watch last night’s periscope below:
Multiple Sclerosis (MS) is a neurological disease caused by demyelination or breakdown of the myelin coating around the nerve cells (1). This is referred to as a neurodegeneration where the physical structure of the nerve is compromised, much like the coating around an electrical wire being chipped or stripped away. Common symptoms of MS are sensory symptoms in the extremities or face, unilateral visual loss, acute or subacute motor weakness of the muslces, diplopia (double vision), gait disturbance and balance problems, Lhermitte sign (electric shock-like sensations that run down the back and/or limbs upon flexion of the neck), vertigo, bladder problems, loss of control of a limb, and pain.
Initially, and for many years, the degeneration seen in multiple sclerosis (MS) was thought to occur because of an acute inflammatory attack on the cells by dis-regulated immune cells crossing the blood brain barrier. However, treatments focused on modulating the inflammatory attack seem to have no effect on the degeneration and demyelination. Thus, the actual definitive cause of this demyelination and neuro-degeneration has eluded us since 1868, when Jean-Martin Charcot first described it.
Recent studies point to evidence that this demyelation may be due to degeneration or breakdown of the nerve cell’s ability to use glucose as a primary fuel (2, 3). It is now theorized that MS may be due to a combination of degeneration and localized inflammation related to poor glucose uptake causing the demyelination which is seen in a number of MS cases (4, 5, 6).
A. Normal nerve cell with intact myelin sheath around the axon. B. Demyelinated axion nerve losing its ionic charge due to escape of potassium. C. Radio-labled tracer allowing visualization of demyelination on PET Scan
With this dual concept in mind, ketogenic diets have demonstrated some promising results when used with neurological diseases including MS. Ketogenic diets have been used in the treatment of epilepsy since 500 B.C. and in the treatment of obesity since 1860. It is now becoming apparent that ketogenic diets may play a very significant role in the treatment of neurological disease because of two-fold effects that arise when ketones become the primary fuel for the body.
First, when a person becomes keto-adapted and ketones are used as the primary fuel, instead of glucose, the body up-regulates mitochondria to use the ketones for fuel. As the ketone level rises, the need for glucose diminishes. This provides the nerve cell an alternative fuel source if glucose metabolism is impaired. It also decreases the need and production of insulin, a known hormone heavily involved in stimulating inflammation and inflammatory responses.
The second effect of a ketogenic diet is this favorable effect on inflammation. It has been demonstrated that a ketogenic diet decreases reactive oxygen species, increased production of superoxide dismutase and catalayse, all of which notably decrease the inflammatory effects of oxidative stress (9,10, 11). A ketogenic diet also is well known to raise glutithione levels, another anti-oxidant that decreases inflammation and oxidative stress (12-16). This same anti-inflammatory and keto-adaptation effect can be obtained from intermittent fasting.
To date, studies in patients with neurologic diseases like MS, Alzheimer’s disease using ketogenic diets have had positive results in memory, cognition and diminished inflammation with evidence of halting or reversing the chronic demyelination (17,18, 19). Still somewhat theoretical, the evidence points to effective dietary treatment and prevention for multiple sclerosis and other degenerative neurological diseases like Alzheimer’s Disease.
References:
J. M. Pearce, “Historical descriptions of multiple sclerosis,” European Neurology, vol. 1, no. 1, pp. 49–53, 2005.
C.-A. Castellano, S. Nugent, N. Paquet et al., “Lower brain 18F-fluorodeoxyglucose uptake but normal 11C-acetoacetate metabolism in mild Alzheimer’s disease dementia,” Journal of Alzheimer’s Disease, vol. 43, no. 4, pp. 1343–1353, 2014.
S. Nugent, S. Tremblay, K. W. Chen et al., “Brain glucose and acetoacetate metabolism: a comparison of young and older adults,” Neurobiology of Aging, vol. 35, no. 6, pp. 1386–1395, 2014.
H. Lassmann, W. Brück, and C. F. Lucchinetti, “The immunopathology of multiple sclerosis: an overview,” Brain Pathology, vol. 17, no. 2, pp. 210–218, 2007.
C. Confavreux and S. Vukusic, “Natural history of multiple sclerosis: a unifying concept,” Brain, vol. 129, no. 3, pp. 606–616, 2006.
P. K. Stys, G. W. Zamponi, J. van Minnen, and J. J. G. Geurts, “Will the real multiple sclerosis please stand up?” Nature Reviews Neuroscience, vol. 13, no. 7, pp. 507–514, 2012.
P. G. Nijland, I. Michailidou, M. E. Witte et al., “Cellular distribution of glucose and monocarboxylate transporters in human brain white matter and multiple sclerosis lesions,” Glia, vol. 62, no. 7, pp. 1125–1141, 2014.
L. C. Costantini, L. J. Barr, J. L. Vogel, and S. T. Henderson, “Hypometabolism as a therapeutic target in Alzheimer’s disease,” BMC Neuroscience, vol. 9, supplement 2, article S16, 2008.
P. G. Sullivan, J. E. Springer, E. D. Hall, and S. W. Scheff, “Mitochondrial uncoupling as a therapeutic target following neuronal injury,” Journal of Bioenergetics and Biomembranes, vol. 36, no. 4, pp. 353–356, 2004.
P. G. Sullivan, N. A. Rippy, K. Dorenbos, R. C. Concepcion, A. K. Agarwal, and J. M. Rho, “The ketogenic diet increases mitochondrial uncoupling protein levels and activity,” Annals of Neurology, vol. 55, no. 4, pp. 576–580, 2004.
T. Shimazu, M. D. Hirschey, J. Newman et al., “Suppression of oxidative stress by β-hydroxybutyrate, an endogenous histone deacetylase inhibitor,” Science, vol. 339, no. 6116, pp. 211–214, 2013.
S. G. Jarrett, J. B. Milder, L.-P. Liang, and M. Patel, “The ketogenic diet increases mitochondrial glutathione levels,” Journal of Neurochemistry, vol. 106, no. 3, pp. 1044–1051, 2008.
J. B. Milder, L.-P. Liang, and M. Patel, “Acute oxidative stress and systemic Nrf2 activation by the ketogenic diet,” Neurobiology of Disease, vol. 40, no. 1, pp. 238–244, 2010.
N. Dupuis, N. Curatolo, J. F. Benoist, and S. Auvin, “Ketogenic diet exhibits anti-inflammatory properties,” Epilepsia, vol. 56, no. 7, pp. e95–e98, 2015.
D. Y. Kim, J. Hao, R. Liu, G. Turner, F.-D. Shi, and J. M. Rho, “Inflammation-mediated memory dysfunction and effects of a ketogenic diet in a murine model of multiple sclerosis,” PLoS ONE, vol. 7, no. 5, Article ID e35476, 2012.
Y.-H. Youm, K. Y. Nguyen, R. W. Grant et al., “The ketone metabolite β-hydroxybutyrate blocks NLRP3 inflammasome—mediated inflammatory disease,” Nature Medicine, vol. 21, no. 3, pp. 263–269, 2015.
A. Ramm-Pettersen, K. O. Nakken, I. M. Skogseid et al., “Good outcome in patients with early dietary treatment of GLUT-1 deficiency syndrome: results from a retrospective Norwegian study,”Developmental Medicine and Child Neurology, vol. 55, no. 5, pp. 440–447, 2013.
Y. Ito, H. Oguni, S. Ito, M. Oguni, and M. Osawa, “A modified Atkins diet is promising as a treatment for glucose transporter type 1 deficiency syndrome,” Developmental Medicine and Child Neurology, vol. 53, no. 7, pp. 658–663, 2011.
M. Storoni and GT Plant, “The Therapeutic Potential of the Ketogenic Diet in Treating Progressive Multiple Sclerosis,” Multiple Sclerosis International, vol. 2015, Article ID 681289, 9 pages, 2015.
The image above has nine dots within a square. Your task, using only four lines is to connect ALL nine dots WITHOUT ever raising your pen, pencil or finger (Please don’t use a sharpie on your computer screen . . . it doesn’t come off).
You may have seen this puzzle previously . . . it’s made its rounds in corporate training circles. But the underlying principle remains true. The solution requires you to expand your thinking or to “think outside the box.”
Whenever you find yourself on the side of the majority, it is time to pause and reflect. (Mark Twain)
Why should we limit ourselves to thinking outside the box. Can’t we just get rid of the box?
True discovery consists in seeing what everyone has seen . . . then, thinking what no one has thought.
The answer can be found when those four lines are used beyond the box our mind creates:
What good has the box done us? People were burned at the stake because they refused to believe the Earth was not the center of the universe. People were beheaded because they had a sneaking suspicion that the world was not flat.
Why is it so very hard to accept that our weight gain and diabetes are driven by a hormonal signal, and not by gluttony or caloric intake of fat? The definition of insanity is doing the same thing repetitively and expecting a different outcome. How long have you been restricting calories and fat with only minimal or no improvement in your weight, blood sugar, cholesterol or general feeling of health?
The main problem with the current thought model, or dogma, on the obesity’s cause is that it does not account for metabolic syndrome. Metabolic syndrome is insulin resistance. It is an over production of insulin in the presence of ANY form of carbohydrate (sugar or starch).
In the practice of medicine over the last 15 years, I noticed that a very interesting pattern emerged. There was always a spike in fasting and postprandial insulin levels 5-10 years prior to the first abnormal fasting and postprandial blood sugars. These patients were exercising regularly and eating a diet low in fat. But they saw continued weight gain and progressed down the path of metabolic syndrome. 10-15 years later, they fall into the classification of type II diabetes. What I now lovingly refer to as stage IV insulin resistance.
The only thing that seems to halt this progressive process with any degree of success is carbohydrate restriction. Fasting insulin levels return to normal, weight falls off, and the diseases of civilizations seem to disappear as insidiously as they arose.
So you tell me, is the world flat? Is the Earth the center of the universe?
What is a low carbohydrate or ketogenic diet? 15 years of practical in the trenches experience have helped me develop a very simple program to help you lose and maintain your weight. Access to this program, video help and access to blog articles at your fingertips are offered through my online membership site.
You can also hear me each week a I discuss low carbohydrate, paleolithic and ketogenic diets with the Legendary Jimmy Moore on KetoTalk.com
Let me answer that question with the following questions:
Do you find yourself longing for the apocalypse?
Do you find yourself looking for a reason to live?
Are you feeling tired, irritable, stressed out?
Do you or you family find yourself to be overly cynical, jaded or emotionally numb?
If you can answer “yes” to any of the questions above, then I highly recommend prescription strength nature . . .
All parody and humor aside, full strength prescription nature is one of the very best treatments for stress.
I find that sitting outside with my animals, watching the birds, dogs, horses and ducks dramatically helps with lowering my stress levels and helps me re-focus. You can see my favorite place to sit on my farm and watch nature . . . here on Katch.me
You may find the following posts very insightful in explaining how stress wreaks havoc on your weight loss, mood & emotions and how to go about fixing it:
For someone like me, who spends 14-18 hours a day taking care of illness and sickness, I have found that spending time in nature is often more therapeutic than any pill available in the pharmacy. So, this afternoon, if your looking for me, I’ll be taking my own medicine, a prescription of Nature Rx on my horse.
Today in the office I had the calorie conversation again . . . three times. We have an entire society with a very influential health and fitness industry built around the almighty calorie. Has it helped? Looking at our 5 year obesity outcomes. It hasn’t helped a bit. In fact, it is worse. In 1985 only 19% of U.S. adults were obese.
U.S. Obesity Adult 2011U.S. Adult Obesity 2014
In 2014, 34.5% of U.S. adults were obese. The numbers this year are approaching 35.6% You can see the dramatic increase in obesity by 1-3% every year for the last 5 years in the CDC images above.
For over 50 years we have been told that caloric restriction and fat restriction is the solution. But by the numbers above, the 58 million people in the U.S. utilize a gym or health club to burn off those calories aren’t seeing the success that they should be expecting.
Why? Because the calorie is NOT king. What do I mean by that? We don’t gain weight because of the thermogenic dogma we’ve been taught for the last 50 years. Our weight gain is driven by a hormone response to food. Hear more about why the calorie is NOT king on tonight’s PeriScope. You can Katch it here with all the live stream comments and hearts at Katch.me/docmuscles.
Or you can watch the video without the comments here:
It is well know that one of the most profound complications of diabetes is damage to the kidney and the very small arteries within the kidney acting as your body’s filtration system. The kidney begins to lose the ability to adequately filter and retain microscopic protein progressively over time. As the blood sugar and insulin levels continually rise over time in the patient with diabetes or pre-diabetes, damage to the delicate filtering system of the kidneys occur. This very common and progressively damaging problem is called “nephropathy.”
Chronic elevated blood sugar and insulin cause the filtering system to become more and more “leaky” and ineffective.
We knew in 1972 that patients with diabetes had thickening of the basement membrane or endothelium of the small tubles within the kidneys. In fact, 98.6% of diabetics tested had thickening of this area of endothelium and tubules also called the renal glomeruli (1). This allows the glomerulus or filtration system of the kidney to become more “leaky” and microscopic protein loss begins to occur through the kidney. This loss of important proteins in the blood is called “albuminuria” or “micro-albuminuria.” It is a flag that further damage of the kidney can and will occur without making significant changes to lower the blood sugar and the insulin. As of today, it is not totally clear how the basement membrane is damaged at the microscopic level, however, there is some evidence that elevated insulin has both a physical and immune type effect that stimulates oxidative stress, atherogenesis, immunoglobulins, as well as the formation advanced glycation end products leading to endothelial wall damage (2).
Recent research reveals that a ketogenic diet effectively repairs and/or completely reverses the albuminuria (3).
Evidence in my office of the significant improvement in micro-albumin can be seen in the one of a number of case studies below:
72 year old male with history of diabetes, diabetic nephropathy already treated with full dose statins, ACE inhibtors, metformin, and Januvia. (Remember, microalbumin should be <30 mg/g)
Date Microalbumin HbA1c
8/12/2010 2264 mg/g 6.4% Started carb restriction <30 g per day.
10/01/2010 1274 mg/g 5.2%
1/08/2011 1198 5.8% Admits to cheating over holidays
12/26/2013 2434 mg/g 6.8% Returned from 2 yr travel-off diet
2/27/2014 399 mg/g 6.3% Restarted carb restriction <20g per day
6/20/2014 190 mg/g 7.0% Traveling – no carb restriction
The patient began following a ketogenic diet in 2010. After improvement he moved out of town for two years and “fell of the wagon.” Upon returning h restarted his carbohydrate diet and was only partially following it. As you can see, he also admitted to some cheating on the carbohydrate restriction over the holidays. In light of this, carbohydrate restriction decreased his albuminuria from 2400 to 97 mg/g within a period of 18 months.
References:
Siperstein MS, Unger RH, Madison LL. “Further Electron Microscopic Studies of Diabetic Microagniopathy.” Early Diabetes: Advances in Metabolic Disorders, sup 1. New York: Academic Press, 1972, p261-271.
Nasr SH, D’Agati VD. “Nodular glomerulosclerosis in the nondiabetic smoker.” J Am Soc Nephrol. 2007;18(7):2032.
Poplawski MM, Mastaitis JW, Isoda F, Grosjean F, Zheng F, Mobbs CV (2011) Reversal of Diabetic Nephropathy by a Ketogenic Diet. PLoS ONE 6(4): e18604. doi:10.1371/journal.pone.0018604

































 So, how do you manipulate the hormones in a way to control the rebounding hunger and suppression of metabolism? This is where we put a bit of twist on the knowledge we’ve gained from alternate day fasting. Recent research shows that “mild” energy deficit in a pulsatile manner, that has the ability to mimicking the body’s normal bio-rhythm’s is dramatically effective in reducing weight and maintaining normal hormonal function without cause of rebound metabolic slowing (4).
So, how do you manipulate the hormones in a way to control the rebounding hunger and suppression of metabolism? This is where we put a bit of twist on the knowledge we’ve gained from alternate day fasting. Recent research shows that “mild” energy deficit in a pulsatile manner, that has the ability to mimicking the body’s normal bio-rhythm’s is dramatically effective in reducing weight and maintaining normal hormonal function without cause of rebound metabolic slowing (4).








 raise insulin levels without raising blood sugar and are not appropriate for use with a true low-carbohydrate/ketogenic diet. You can see and print the article I published clarifying which sweeteners you can use and which ones to avoid here:
raise insulin levels without raising blood sugar and are not appropriate for use with a true low-carbohydrate/ketogenic diet. You can see and print the article I published clarifying which sweeteners you can use and which ones to avoid here:











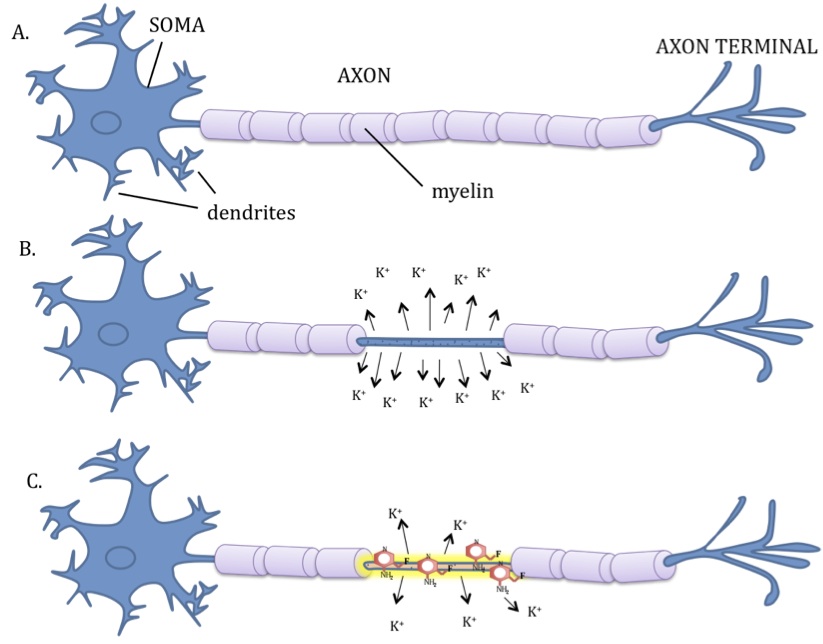






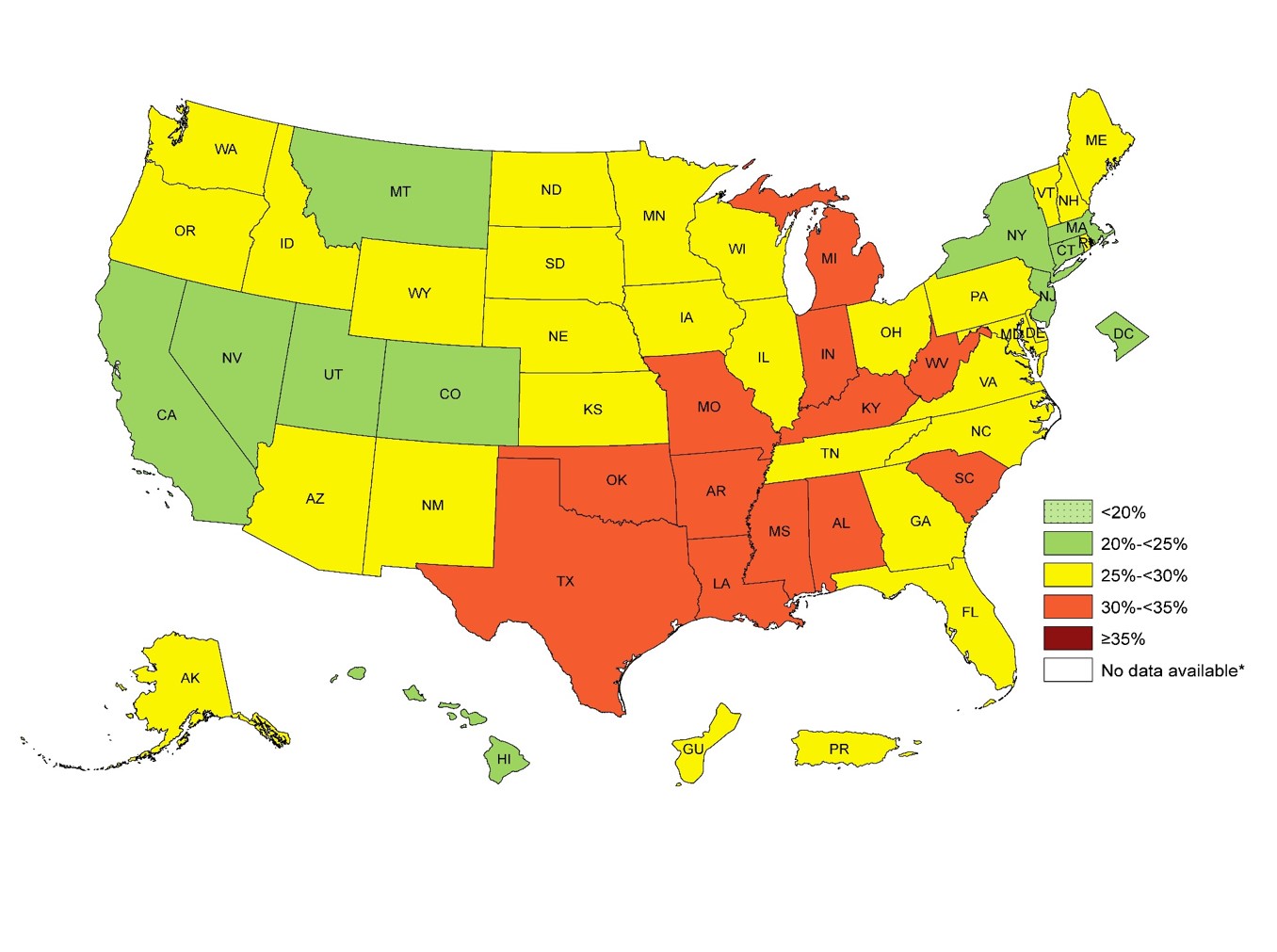
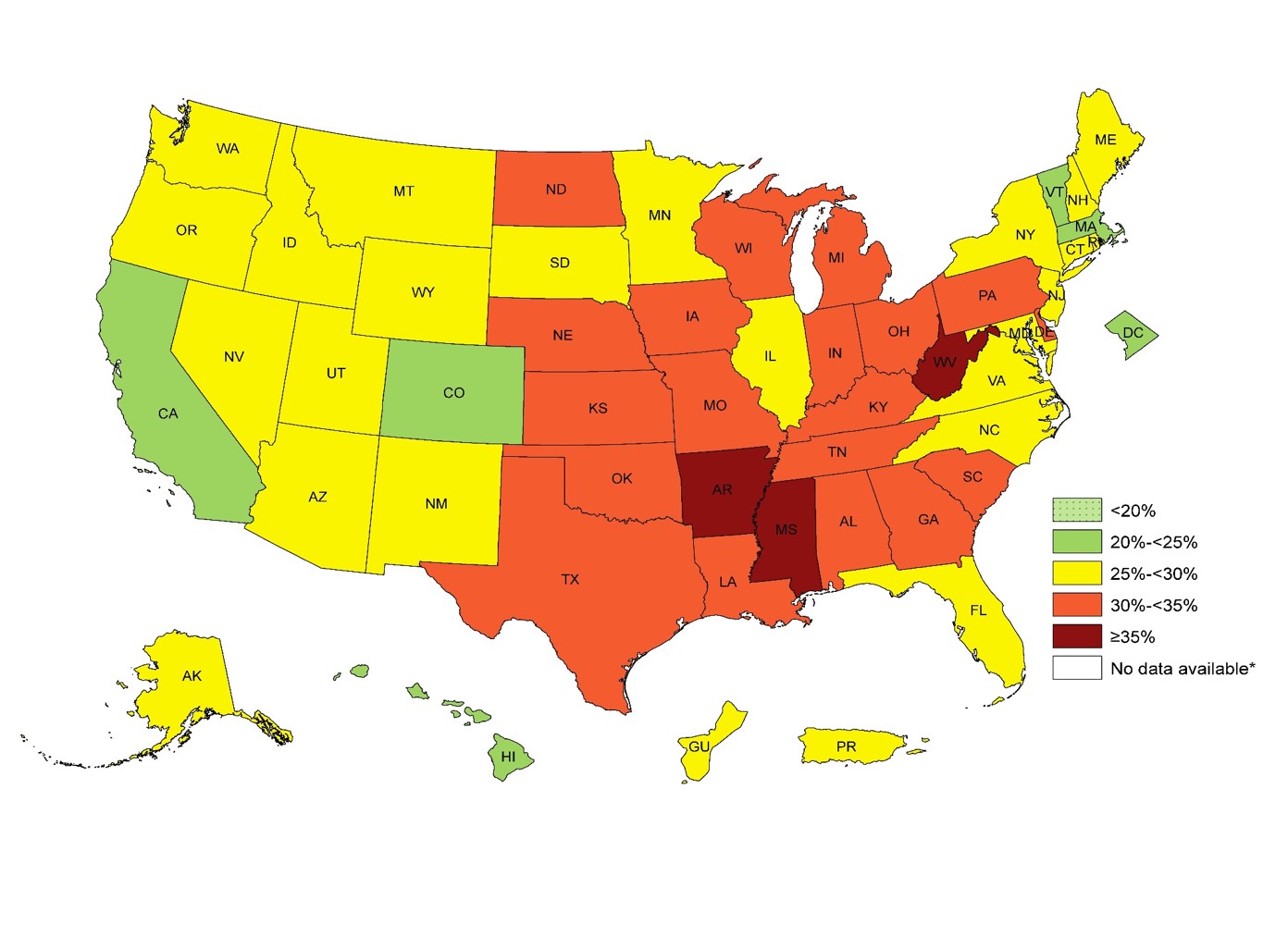

{kind=link}