Over fifty years of data have demonstrated that creating energy deficit through the reduction in caloric intake is effective in reducing weight. . . However, it is only for the short term (1, 2). The biggest challenge physicians face in the treatment of obesity is that calorie restriction fails when it comes to long-term weight loss.
Isn’t Fasting Effective in Long-Term Weight Loss?
With the craze and popularity of intermittent fasting, some have claimed that intermittent fasting is more effective in weight reduction. Recent results demonstrate that this may also be incorrect. In the short term evaluation of caloric restriction and intermittent fasting, reduction in 15-20 lbs of weight is effectively seen and the highly publicized Biggest Loser’s losing ~ 120 lbs. Intermittent fasting and alternate day fasting have been shown to be more effective in lowering insulin levels and other inflammatory markers in the short term.
There is, however, controversy over maintaining weight loss beyond 12 months in the calorie restriction, intermittent and alternate day fasting groups. Forty different studies in a recent literature review, thirty-one of those studies looking at forms of intermittent fasting, demonstrate that the majority of people regain the weight within the first 12 months of attempting to maintain weight loss(3, 5). This is, also, what I have seen for over 18 years of medical practice.
Is Calorie Restriction the Only Way to Lose Fat?
Numerous “experts” claim that the only way to reduce fat is “caloric deficit.” Variations through the use of intermittent, long-term or alternate day fasts can be found all over the internet. In regards to calorie restriction, these “experts” with nothing more than a personal experience and a blog to back their claims preach this louder than the “televangelists” preach religion. Based on the faith that many place in this dogma, it could be a religion. What causes belief in this dogma is that weight and fat loss actually does occur with caloric restriction to a point. The average person will lose 20-25 lbs, however, within 12 months of achieving this goal, most people regain all the weight. (No one ever mentions the almost universal problem with long-term weight loss, especially those “experts.”)
Prolonged calorie restricted fasts, intermittent fasts, and alternate day fasts are often grouped together into the fasting approach, causing significant confusion among those that I speak to and counsel in my office. There is great data that alternate day fasts do not have the reduction in resting energy expenditure that prolonged fasting, intermittent fasting and calorie restriction cause. However, none of these approaches appears to solve the problem of weight re-gain after long-term (12-24 months into maintenance) weight loss (3). And, a recent study of 100 men participating in alternate day fasting showed that there was a 38% dropout rate, implying that without close supervision and direction, maintenance of this lifestyle is not feasible for over 1/3rd of those attempting it.
Long-Term Weight Loss Failure Brings Tears
Failure on calorie restricted diets, low fat diets, and intermittent fasting diets with weight regain at twelve to twenty-four months is the most common reason people end up in my office in tears. They’ve fasted, starved themselves, calorie restricted, tried every form of exercise, and still regained the weight. Trainers, coaches and “experts” have belittled them for “cheating” or just not keeping to the diet. Yet, we know that calorie restriction and intermittent fasting cause a rebound in leptin, amilyn, peptid YY, cholecystikinin, insulin, ghrelin, gastric inhibitory peptide and pancreatic poly peptide by twelve months causing ineffective long-term weight loss (6). The dramatic rise in these hormones stimulates tremendous hunger, especially from ghrelin and leptin.

Although less problematic in alternate day fasting, these calorie restricted approaches also cause dramatic slowing of the metabolism at the twelve month mark. In many cases, the metabolic rate never actually returns to baseline, creating even more difficulty in losing further weight or even maintaining weight (6).

Is Gastric Bypass or Gastric Sleeve the Solution?
Gastric bypass and the gastric sleeve procedures have been touted as the solution to this problem, as they decrease ghrelin, however, 5-10 years later, these patients are also back in my office. They find that 5-10 years after these procedures the weight returns, cholesterol and blood pressure rise, and diabetes returns. These hormones kick into high gear, stimulating hunger in the face of a slowed metabolism, that to date, has been the driver for weight regain in the majority of people. People find it nearly impossible to overcome the hunger. You may have experienced this, I know I have.
It’s the Hormones, Baby!
So, what is the answer? It’s the hormones. (WARNING – You’ll hear that when your wife is pregnant, too, gentlemen). We are hormonal beings, both in weight gain, and in pregnancy. Trying to preach calorie control to a hormonal being is like showing up at the brothel to baptize the staff. You might get them into the water, but you’re probably not getting them returning weekly to church or pay a tithe.
 So, how do you manipulate the hormones in a way to control the rebounding hunger and suppression of metabolism? This is where we put a bit of twist on the knowledge we’ve gained from alternate day fasting. Recent research shows that “mild” energy deficit in a pulsatile manner, that has the ability to mimicking the body’s normal bio-rhythm’s is dramatically effective in reducing weight and maintaining normal hormonal function without cause of rebound metabolic slowing (4).
So, how do you manipulate the hormones in a way to control the rebounding hunger and suppression of metabolism? This is where we put a bit of twist on the knowledge we’ve gained from alternate day fasting. Recent research shows that “mild” energy deficit in a pulsatile manner, that has the ability to mimicking the body’s normal bio-rhythm’s is dramatically effective in reducing weight and maintaining normal hormonal function without cause of rebound metabolic slowing (4).
Pulsed Mild Energy Restriction
What does this mean in layman’s terms? It means that if we provide a diet that maintains satiety hormones while providing a period of baseline total energy expenditure needs and a period of mildly reduce caloric intake in a pulsed or cyclic manner, greater weight loss occurs and there is no rebound of weight 1-2 years later.
The main reason I’ve not jumped on the intermittent fasting band wagon is the shift in leptin, amylin, ghrelin and GLP-1 signaling that regularly occurs at the 6-12 month mark. The rebound of these hormones causes weight re-gain and is what prevents successful long-term weight loss. A number of people come to my office and tell me they couldn’t follow a ketogenic diet, so they’re doing intermittent fasting and it works . . . for a while. Then, they end up in my office having hit a plateau or fallen off the wagon and regained all the weight. They are completely confused and don’t understand what happned. Most of them are convinced it’s their thyroid or cortisol and they’ve seen every naturopath and functional medicine doctor in town.
What people really need is a simple approach to long-term weight loss without having to spend the night in the physiology lab every two weeks sleeping under a ventilated hood system.
The Ketogenic Lifestyle is a Pulsed Energy Lifestyle
- First, it is essential to turn off the insulin load. Insulin is the master hormone. This is done by a ketogenic lifestyle that restricts carbohydrates.
- Second, providing adequate protein to supply maintenance of muscle and testosterone is key.
- Third, providing adequate fat is the simple way to maintain leptin, ghrelin, amylin, GLP-1 (among the others) and long-term weight loss. Can you eat too much fat? Of course you can. But, because each of us have differing levels of stress and activity each day, this fat intake becomes the lever for hunger control.
- Fourth, the use of exogenous ketones ensures easily accessible ketone (short chain fatty acids) to modulate adipose (white fat) signaling of the liver without large caloric intake through the portal vein by first pass of liver metabolism. The ketones also help stabilize the gut bacteria. The combination of hormone balance between the liver and fat cells and improvement of gut bacteria suppresses key hunger hormones and aids glucose regulation between the fatty tissues and the liver. Ketones, both endogenous and exogenous, suppress production of TNF-alpha, IL-6, resistin, and stabilize production of adiponectin and leptin from the adipose cells (7, 8, 9).
In my office, once we calculate the basic protein needs daily, we start with a 1:1 ratio of protein to fat. Then, the fat is adjusted up or down based on hunger. Remember, hunger occurs, because your body produces hormones. The addition of fat to a diet that is not stimulating large amounts of insulin resets the hormone patterns back to normal without causing weight gain.
Give Obese People Fat Ad Libitum?
“Sure, Dr. Nally, but what about those people who don’t know if they are hungry, bored, stressed or just have a bacon fixation? You can’t just give them all the fat they want?!”
Why not? Implying that people aren’t smart enough to know when they are full is a bit of a fascist philosophy, don’t you think?
Do people over eat? Sure they do. But, I’ve found that when you give people an antidote to hunger (using fat intake in the presence of stabilized insulin levels) over a few months, people begin to recognize true hunger from other forms of cravings. This is especially true when they keep a diet journal. This gives people the ability to begin listening to their own bodies, responding accordingly and governing their stress, eating, exercise and activity. Keeping a diet journal is key to long-term weight loss. And, isn’t helping people use their own agency to improve their health really what we’re trying to do?
Interestingly, doing this over the years seems to line up with the findings of this year’s MATADOR study in the International Journal of Obesity. They found that mild intermittent energy restriction of about 30-33% for two weeks, then interrupting this with two weeks of a diet that was energy balanced for needs improved both short and long-term weight loss efficiency (4). In looking at my, and my patient’s diet journals, this energy restriction of about 1/3 of needed calories cyclically seems to happens naturally with a ketogenic lifestyle, without even counting calories. (Calories are a swear-word in my office).
What does the correct long-term wight loss program look like in a diet or meal plan? Well, you’ll have to join the Ketogenic Lifestyle 101 Course to see what that really means to you individually. I look forward to seeing you there.
Want to find out more about the Ketogenic Lifestyle 101 course? CLICK HERE.
Have you read my book The Keto Cure? Get a signed copy from me by clicking HERE.
References:
- Bronson FH, Marsteller FA. “Effect of short-term food deprivation on reproduction in female mice.” Biol Reprod. Oct 1985; 33(3): 660-7. https://www.ncbi.nlm.nih.gov/pubmed/4052528?dopt=Abstract&holding=npg
- Connors JM, DeVito WJ, Hedge GA. “Effects of food deprivation on the feedback regulation of the hypothalamic-pituitary-thyroid axis of the rat.” Endocrinology. Sep 1985. 117(3): 900-6. https://www.ncbi.nlm.nih.gov/pubmed/3926471?dopt=Abstract&holding=npg
- Seimon RV, Roekenes JA, Zibellini J, Zhu B, Gibson AA, Hills AP, Wood RE, King NA, Byrne NM, Sainsbury A. “Do intermittent diets provide physiological beneftis over continuous diets for weight loss? A systematic review of clinical trials.” Mol Cell Endo. 15 Dec 2015. 418(2): 153-172. https://www.sciencedirect.com/science/article/pii/S0303720715300800
- Byrne NM, Sainsbury A, King NA, Hills AP, Wood RE. “Intermittent energy restriction improves weight loss efficiency in obese men: the MATADOR study.” Int J Obes. 2018. 42:129-138. https://www.nature.com/articles/ijo2017206
- Trepanowski JF, Kroeger CM, Barnosky A. “Effect of Alternate-Day Fasting on Weight Loss, Weight Maintenance, and Cardioprotection Among Metabolically Healthy Obese Adults.” JAMA Intern Med. Jul 2017. 177(7): 930-938. https://jamanetwork.com/journals/jamainternalmedicine/article-abstract/2623528?redirect=true
- Sumithran P, Prendergast LA, Delbridge E, Purcell K, Shulkes A, Kriketos A, Proietto J. “Long-term persistence of hormonal adaptations to weight loss.” N Engl J Med. 27 Oct 2011. 365: 1597-1604. http://www.nejm.org/doi/full/10.1056/NEJMoa1105816
- Asrih M et al., “Ketogenic diet impairs FGF21 signaling and promotes differential inflammatory responses in the liver and white adipose tissue.” PlosOne. 14 May 2015. Open Access. https://doi.org/10.1371/journal.pone.0126364
- Veniant MM et al. “FGF21 promotes metabolic homeostasis via white adipose and leptin in mice.” PlosOne. Jul 2012. Open access. https://doi.org/10.1371/journal.pone.0040164
- Whittle AJ, “FGF21 conducts a metabolic orchestra and fat is a key player.” Endocrinology. 1 May 2016. 157(5): 1722-1724.



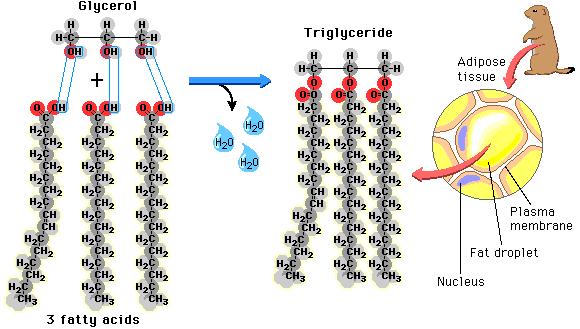 as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
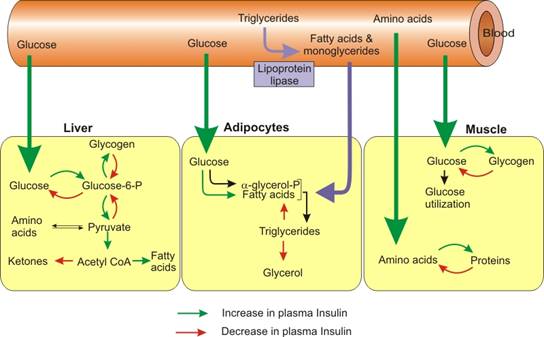 before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).
before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).