

There is no better measure of a person than what he does when he is absolutely free to choose. #thoughtofday #deepthoughts #choices
The Obesity Paradox: The Intersection Where Agricultural Policy Contradicts Health Policy
Intent
The intent of this brief is to analyze the burden of obesity in the United States and to recommend policy changes to reduce the medical costs of obesity imposed upon the individual and country as a whole.
Introduction
Conventional fat reduction/caloric restriction guidelines for the treatment of obesity and associated cardiovascular disease, diabetes, cancer, and hypertension have been recommended since the early 1970’s. Because these guidelines are based on questionable evidence, the cost of obesity has dramatically risen to almost 21% of overall health care costs in the United States (1). This brief will analyze the current medical cost of obesity and will explain why the current obesity reduction guidelines perpetuate the problem. In addition, the brief will examine the impact of government agricultural policy on dietary habits, and will recommend changes to farm subsidy legislation in order to reduce the incidence of obesity and decrease costs to the healthcare system.
History & Background
The Cost of Obesity on the Nation
 As of 2012, obesity accounts for nearly 21% of overall health care costs in the United States. An obese person incurs $2741 more in medical expenses per year than his or her non-obese counterpart (1). Medicare spending has increased per person per year by $600 for each obese beneficiary (includes out-patient and prescription drugs) and Medicaid beneficiary prescription drug spending increased by $230 per year per obese person. Private insurance has increased by $248 for prescription drugs and $443 for in-patient services for each obese beneficiary per year (2). That adds up to $190.2 billion spent annually on obesity-related medical problems (3). This is a drastic change. Health care costs related to obesity were $85.7 billion (9.1% of overall health care costs) in 2006 and $61.2 billion (6.5% of overall health care costs) in 1998 (4).
As of 2012, obesity accounts for nearly 21% of overall health care costs in the United States. An obese person incurs $2741 more in medical expenses per year than his or her non-obese counterpart (1). Medicare spending has increased per person per year by $600 for each obese beneficiary (includes out-patient and prescription drugs) and Medicaid beneficiary prescription drug spending increased by $230 per year per obese person. Private insurance has increased by $248 for prescription drugs and $443 for in-patient services for each obese beneficiary per year (2). That adds up to $190.2 billion spent annually on obesity-related medical problems (3). This is a drastic change. Health care costs related to obesity were $85.7 billion (9.1% of overall health care costs) in 2006 and $61.2 billion (6.5% of overall health care costs) in 1998 (4).
 The most recent Center for Disease Control statistics reveal that 35.7% of the U.S. adult population is currently obese and another 33% is overweight. Over 78 million adults and 12.5 million children are obese (5). The addition of 30 million people to the health care roles (current estimation of the Affordable Care Act including Medicaid expansion) means that an estimated $27 billion (in 2012 dollars) more will be spent per year on obesity-related health care costs.
The most recent Center for Disease Control statistics reveal that 35.7% of the U.S. adult population is currently obese and another 33% is overweight. Over 78 million adults and 12.5 million children are obese (5). The addition of 30 million people to the health care roles (current estimation of the Affordable Care Act including Medicaid expansion) means that an estimated $27 billion (in 2012 dollars) more will be spent per year on obesity-related health care costs.
Impact of Government Policy on Consumption
The ‘Farm Bill’ was originally enacted as part of President Franklin D. Roosevelt’s Agricultural Adjustment Act of 1933, which provided subsidies to American farmers in the midst of the Great Depression. Since that time the federal government has paid farmers not to grow seven specific crops – known as commodities – with the intent of decreasing the supply, increasing the demand, and thereby raising the price (7). Dr. Susan Blumenthal, former Assistant Surgeon General and current SNAP to Health project director, writes, “The Farm Bill has since expanded to include many different categories or ‘titles.’ The last bill to be authorized, in 2008, had 15 titles, including nutrition (food stamps), crop subsidies, conservation, livestock, crop insurance and disaster assistance. The 2008 Farm Bill approved $300 billion in spending: 67% was spent on food stamps; 15% on agricultural subsidies; 9% on conservation; and 8% on crop insurance” (8).
The U.S. Department of Agriculture (USDA) Subsidy Programs tend to favor, either directly or indirectly, foods that increase obesity and other diseases. These subsidies support commodity crops, specialty crops, dairy products, livestock, and federal purchase programs. Their justification is that they help to stabilize prices in agricultural commodity markets by balancing supply and demand (9). Between 1995 and 2011, $277.3 billion were given in farm subsidies to almost 40% of U.S. farmers. Arizona received $1.1 billion (mainly for cotton); however, only 7% of Arizona farms received subsides during this period (10). These subsidies are incentives to grow and produce specific commodities that have a higher monetary return. Subsidies also act as a disincentive for farmers to grow fruits and vegetables which fall under the “specialty crops” category. This restricts both small and large farmers from diversifying their crops, and limits fruit and vegetable production (11).
Arizona farms received $25.3 million in dairy subsidies from 1995-2011 and $29.5 million in livestock subsidies during that same period (9). Arizona ranks 2nd nationally in its production of cantaloupe & honeydew melons, head & leaf lettuce, spinach, broccoli, cauliflower and lemons, all of which are “specialty crops” and do not receive subsidies (12). The most recent statistics show that the top five states receiving subsidies are Iowa, Texas, Illinois, Nebraska and Minnesota, with Kansas coming in at a close sixth. The majority of these subsidies are for corn ($81.7 billion), soybeans ($26.4 billion), rice ($13.3 billion) and wheat ($34.4 billion) from 1995-2011 (10). It is important to note that the Renewable Fuel Standard of 2012 (legislation protecting the corn-ethanol lobby) mandates that 37% of the corn harvest be used in ethanol production (13).
The food subsidies above have been in place since the Food, Conservation & Energy Act of 2002 and renewed in 2008. They were only to be available for a period of five additional years and were set to expire September 30, 2012. However, the American Taxpayer Relief Act of 2012 (H.R. 8), enacted by Congress and signed into law by President Barack Obama, included provisions that extended these subsidies until September 30, 2013 (20).
For many low-income Americans and especially children, federal programs have a direct and significant influence on food choices.  Over 30 million children receive government subsidized school lunch through National School Lunch Program (NSLP) administered by the USDA Food and Nutrition Service (14). USDA-purchased meats, dairy products, grains, fruits, and vegetables are supplied to schools for use in meal programs. Current school lunch recommendations on calorie intake set by the USDA and The Healthy, Hunger-Free Kids Act of 2010mandate school lunches provide 650-850 calories per meal to the 30 million children currently enrolled in this program (15). Interestingly, that is the same caloric count of a Big Mac®, small fry and Diet Coke® from McDonalds® (16). The rational for these purchase decisions are based upon agricultural support goals and adherence to national dietary guidelines (14). A study published in the journal Economics and Human Biology reveals that a person’s body mass index (BMI) increased faster if that personwere on food stamps, and the BMI increased at a faster rate while on the Supplemental Nutrition Assistance Program (SNAP). “We can’t prove that the Food Stamp Program causes weight gain, but this study suggests a strong linkage,” said Jay Zagorsky, co-author of the study and a research scientist at Ohio State University’s Center for Human Resource Research (17). However, much of the food available through the SNAP programs are refined, subsidized high-carbohydrate containing foods.
Over 30 million children receive government subsidized school lunch through National School Lunch Program (NSLP) administered by the USDA Food and Nutrition Service (14). USDA-purchased meats, dairy products, grains, fruits, and vegetables are supplied to schools for use in meal programs. Current school lunch recommendations on calorie intake set by the USDA and The Healthy, Hunger-Free Kids Act of 2010mandate school lunches provide 650-850 calories per meal to the 30 million children currently enrolled in this program (15). Interestingly, that is the same caloric count of a Big Mac®, small fry and Diet Coke® from McDonalds® (16). The rational for these purchase decisions are based upon agricultural support goals and adherence to national dietary guidelines (14). A study published in the journal Economics and Human Biology reveals that a person’s body mass index (BMI) increased faster if that personwere on food stamps, and the BMI increased at a faster rate while on the Supplemental Nutrition Assistance Program (SNAP). “We can’t prove that the Food Stamp Program causes weight gain, but this study suggests a strong linkage,” said Jay Zagorsky, co-author of the study and a research scientist at Ohio State University’s Center for Human Resource Research (17). However, much of the food available through the SNAP programs are refined, subsidized high-carbohydrate containing foods.
The price of food influences an individual’s consumption choices (6). Foods that are refined contain increased amounts of sugar or high-fructose corn syrup. These foods contain more caloric density and are often cheaper and more easily accessible. These are foods that are usually found in the center of the grocery store and frequently on sale at the end-caps of each isle. Nutrient-dense, higher fiber foods are frequently associated with higher prices and are consumed less often. These are the foods you usually find around the peripheral areas of the grocery store (fruits, vegetables, etc.) Current food subsidy policy found in the Food, Conservation and Energy Act of 2008 extension mandated by the American Taxpayer Relief Act of 2012 drives up the price of fruits, vegetables, and meats. This policy also turns people toward lower cost foods that are higher in simple carbohydrates and caloric density. Thus, current policy is actually making obesity worse and making America fatter. Research completed at the University of Illinois at Chicago reveals that small taxes or price changes do not produce a change in a person’s BMI; however, more significant price change has a measurable and significant effect on weight in both adults and children. Price increases of 100-150% have been shown to change purchasing behavior and thereby affect health (18). An example of this is the tax levied on cigarette smoking.
The USDA disagrees with the amount of influence they have over the individual American’s food choices. They state openly on their website that “Some public health advocates have argued that falling real, or inflation-adjusted, prices for many high-calorie foods encourage people to buy and consume more of these foods, leading to poor diet quality and rising rates of obesity. A closer look at how consumers respond to food price variation–over time, across geographic markets, in different types of stores, and in response to taxes and subsidies–reveals how food prices affect people’s food choices, and their waistlines. In short, price matters, but not very much, and it is not the only factor” (19).
Why Current Dietary Guidelines Have Not Been Effective
Why do we get fat? Why have we not been successful in losing weight via diet and exercise? The obesity paradox was described by Jules Hirsch of Rockefeller University, who proposed two opposing hypotheses:
- “Obesity is the result of a willful descent into self-gratification” implying that we gain weight because we over-eat (caloric excess) leading to caloric imbalance.
- “Alternative hypothesis is that there is something ‘biologic’ about obesity, some alteration of hormones, enzymes or other biochemical control systems which leads to obesity” (22).
The 1977 Dietary Goals for the United States – the first comprehensive statement by any branch of the federal government about the American diet – supported the first theory. The Guidelines were heavily influenced by the American Heart Association’s position that fat intake alone would cause heart disease. The USDA 2011 Dietary Guidelines imply that the “people who are the most successful at achieving and maintaining a healthy weight do so through continued attention to consuming only enough calories from foods and beverages to meet their needs and by being physically active.” (15)
Current research contradicts the caloric restriction or “calorie in – calorie out” theory. Scientific evidence clearly demonstrates the domino effect of carbohydrate or starch intake increasing insulin levels which thereby stimulates obesity by raising cholesterol and triglyceride levels. Time Magazine recently published evidence that the longstanding recommendations to “eat less high-fat red meat, eggs and dairy and replace them with more calories from fruits, vegetables and especially carbohydrates” is now seen as incorrect (45). Even our medical textbooks from 1965, like the introductory chapter of the Handbook of Physiology, make it clear that carbohydrate intake cause weight gain and raise triglyceride and cholesterol levels (22), (23), (24).
Current Policy
The current version of the Farm Bill was set to expire September 30th, 2013. If it had been allowed to expire, the results would have returned us to the 1949 Farm Bill legislation and theoretically double the price of milk. However, this would have had the effect of freeing up over $5 billion dollars of federal spending per year and would also lead to decreased consumption of a major source of carbohydrates in the standard American diet like wheat and corn. Senator Debbie Stabenow (D-MI), and chairwoman of the Senate Agriculture Committee, had repeatedly said she was opposed to an extension; however, she agreed to a compromise extending the bill for another year to help the farmers experiencing serious drought conditions in 2012 (7). Two additional extensions were passed in the House and Senate, but because these differed so significantly, it was referred to a House-Senate Conference Committee to work out the compromise details. With only $23 billion in spending reductions, The Agricultural Act of 2014 was passed on January 29, 2014 (46).
Outcomes and Stakeholders
 If the United States continues its current course, up to 58% of the population will be obese by 2030 (26). Many believe that the USDA Dietary Guidelines are to blame. Richard David Feinman, President of the Nutrition and Metabolism Society and Professor of Cell Biology at SUNY Downstate Medical Center said, “The previous Guidelines have not worked well. It is unreasonable to ask the Dietary Guidelines Advisory Committee (DGAC) to audit its own work. An external panel of scientists with no direct ties to nutritional policy would be able to do a more impartial evaluation of the data. This would be far better for everyone.” (27) A recent Gallup Poll reveals that 63% of Americans believe the USDA Guidelines that a low fat, calorie restricted diet will help in reduction of obesity, and the same study showed that 48% of Americans worry about their weight “all of the time or some of the time” (28). Recent evidence from the Women’s Health Initiative Dietary Modification Trial studying 49,000 women supports Dr. Feinman’s conclusion above. It did not show any statistically significant evidence that following a low-fat or caloric restricted diet had any effect upon obesity (29). Other nutritional experts from the Salt Institute and the National Health Coalition have expressed their support for significant changes to the USDA Dietary Guidelines (30). The Weston A. Price Foundation, which according to its website is “dedicated to restoring nutrient-dense foods to the human diet through education, research and activism,” also supports the view that the current USDA Dietary Guidelines have been a significant cause of obesity and have been an active voice promoting legislative change (31).
If the United States continues its current course, up to 58% of the population will be obese by 2030 (26). Many believe that the USDA Dietary Guidelines are to blame. Richard David Feinman, President of the Nutrition and Metabolism Society and Professor of Cell Biology at SUNY Downstate Medical Center said, “The previous Guidelines have not worked well. It is unreasonable to ask the Dietary Guidelines Advisory Committee (DGAC) to audit its own work. An external panel of scientists with no direct ties to nutritional policy would be able to do a more impartial evaluation of the data. This would be far better for everyone.” (27) A recent Gallup Poll reveals that 63% of Americans believe the USDA Guidelines that a low fat, calorie restricted diet will help in reduction of obesity, and the same study showed that 48% of Americans worry about their weight “all of the time or some of the time” (28). Recent evidence from the Women’s Health Initiative Dietary Modification Trial studying 49,000 women supports Dr. Feinman’s conclusion above. It did not show any statistically significant evidence that following a low-fat or caloric restricted diet had any effect upon obesity (29). Other nutritional experts from the Salt Institute and the National Health Coalition have expressed their support for significant changes to the USDA Dietary Guidelines (30). The Weston A. Price Foundation, which according to its website is “dedicated to restoring nutrient-dense foods to the human diet through education, research and activism,” also supports the view that the current USDA Dietary Guidelines have been a significant cause of obesity and have been an active voice promoting legislative change (31).
On the other hand, the Sugar Association has issued statements that sugar is not the cause of obesity and “continually eating too much food and sedentary lifestyles are the major contributing factors to increasing rates of obesity – not sugar intake” (32). In addition, the American Beverage Association has stated that sugars are not the problem with obesity, but instead, “overweight and obesity are a result of an imbalance between calories consumed and calories burned” (33).
Attempts at modifying the Farm Bill with legislation like the 2012 DeMint Amendment (SA 2276 ) were supported by both Arizona Senators McCain (R-AZ) and Kyl (R-AZ) with a “Yes” vote, as well as Senators Ayotte (R-NH), Brown (R-MA), Burr (R-NC), Coats (R-IN), Coburn (ROK), Cornyn (R-TX), DeMint (R-SC), Graham (R-SC), Hatch (R-UT), Heller (R-NV), Johnson (R-WI), Lee (R-UT), McConnell (R-KY), Murkowski (R-AK), Paul (R-KY), Rubio (R-FL), Sessions (R-AL), and Toomey (R-PA). However, because of a large lobbying agricultural coalition, it was voted down (34). Changing farm subsidies will be a great challenge as 40% of the farmers in the U.S. now have some degree of dependence upon these subsidies. The following agricultural groups have historically had significant monetary interest in the farm subsidies that these amendments would affect:
- American Beekeeping Federation
- American Farm Bureau Federation American Mushroom Institute
- American Sheep Industry Association American Soybean Association
- National Cattlemen’s Beef Association National Corn Growers Association National Cotton Council
- National Council of Farmer Cooperatives National Farmers Union
- National Milk Producers Federation National Pork Producers Council
- National Potato Council
- National Sorghum Producers
- National Watermelon Association
- Produce Marketing Association
- United Dairymen of Arizona
- United Egg Producers
- United Fresh Produce Association
- Western Peanut Growers Association
The following groups have formed coalitions in support of the Farm Bill: Health/Food Justice/Farm Group partnerships, Specialty Crop Farm Bill Alliance, Community Food Security Coalition, Center for a Livable Future at Johns Hopkins University, Collaboration for a Healthy Sustainable Food System, and the Healthy Farms, Healthy People: A Farm & Food Policy Summit for a Strong America.
The American Heart Association’s position is that the Farm Bill needs to be modified to include increased access to fruits and vegetables (35). The American Medical Association’s position in 2008 and 2011 has been for cutting the size and budget of the current Farm Bill (36). The American Osteopathic Association does not currently have a formal position on the Farm Bill.
If certain crops like corn or wheat were no longer subsidized,drastic changes will be likely in the food manufacturing industry, which would likely be the largest proponent against change. Unintended consequences of modifying the Farm Bill and not extending its subsidies could have the short term effect of escalating the price of a number of commodities to two to three times their current price. For example, the price of milk would increase to $6-$8 dollars a gallon without federal subsidies (37). This would likely deter the use of carbohydrates containing dairy products, but may also increase the price of meats and cheeses as well.
The USDA’s Rural Development Progress Report claims that the subsidies it distributed “saved more than 75,000 jobs” in 2006 and over 400,000 jobs in 2011 (38), (39). They claim that without federal farm subsidiesthere would be significant loss of jobs; however, studies from the Cato Institute actually show the opposite.
“Job gains are weak and population growth is actually negative in most of the counties where farm payments are the biggest share of income. Job growth is decidedly weak in the counties most dependent on farm payments. The vast majority of such counties (483) had job gains below the 19 percent national average from 1992 to 2002. A considerable number (167) had outright job losses over the period. In short, farm payments are not yielding robust economic and population gains in the counties where they should have the greatest impact. If anything, the payments appear to be linked with sub-par economic and population growth. To be sure, this quick comparison cannot answer whether growth would have been even weaker in the absence of the payments. Still, farm payments appear to create dependency on even more payments, not new engines of growth” (40).
As of 2010, obesity costs about $73.1 billion per year in lost productivity in the United States (43). The worsening obesity epidemic poses further workforce productivity losses up to 20% more by 2030. Even small improvements in obesity will improve workforce productivity and has substantial potential for savings. Currently, the Affordable Care Act allows employers to charge obese employees 30-50% more for health insurance. Without correcting this epidemic, it may be impossible for many to afford health care, opting out to pay the less expensive tax penalty. This would have the effect of increasing commercial premiums across the country, feasibly pushing private insurance companies out of business and forcing a single payer governmental system.
Recommendations
This brief points out that the overall U.S. healthcare costs associated with obesity have increased by 68% in the last fourteen years. It provides evidence that using current dietary low-fat caloric restriction guidelines show poor statistically significant improvements in obesity. And it provides evidence that obesity is not caused by excessive caloric intake and fat, but by insulin response to carbohydrate intake. Lastly, this analysis provides evidence that the Farm Bill propagates continued worsening obesity rates in the US by providing access to cheap, fattening food.
The USDA 2011 Dietary Guidelines need to be revised to reflect current evidence-based obesity prevention and weight reduction research. The guidelines should include information about limiting the intake of foods high in carbohydrates.
The food subsidy extension provided in the American Taxpayer Relief Act of 2012 was extended five years by the Agricultural Act of 2014. Had it been allowed to expire, it would have saved the country over $200 billion over the next ten years. However, because of so many entitlements involved in this bill, the House and Senate convened in Conference that resulted in a compromise of only $23 billion dollars in spending reductions, the first SNAP reforms since 1996 reducing waste, but did nothing in eliminating subsidies that drive or influence eating behavior (46).
When significant price changes occur, eating behavior will change. As the price of fattening carbohydrates increases, people will eat less of them, leading to a national decrease in obesity and overweight. The current reforms did nothing that will change our dietary behavior.
References
1. Cornell University. Obesity accounts for 21 percent of U.S. health care costs, study finds. Science Daily. [Online] April 9, 2012. [Cited: January 5, 2013.] http://www.sciencedaily.com/releases/2012/04/120409103247.htm.
2. Annual Medical Spending Attributable To Obesity: Payer-And Service-Specific Estimates. Eric A Finkelstein, Justin G Trogdon, Joel W Cohen and William Dietz. Health Affairs, 28, Bethesda, MD : Project HOPE, 2009, Vol. 5. 10.1377/hlthaff.28.5.w822.
3. Begley, Sharon. As America’s Waistline Expands, Costs Soar. Reuters. [Online] Thompson Reuters, April 30, 2012. [Cited: January 5, 2013.] http://www.reuters.com/article/2012/04/30/us-obesity-idUSBRE83T0C820120430.
4. Ungar, Rick. Obesity Now Cost Americans More In Healthcare Spending Than Smoking. Forbes. [Online] 4 30, 2012. [Cited: January 5, 2013.] http://www.forbes.com/sites/rickungar/2012/04/30/obesity-now-costs-americans-more-in-healthcare-costs-than-smoking/.
5. Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesity in the United States, 2009–2010. NCHS data brief, no 82. Hyattsville, MD : National Center for Health Statistics, 2012, 2012.
6. Poverty and Obesity: The Role of Energy Density and Energy Costs. A Drewnowski, SE Specter. s.l. : American Journal of Clinical Nutrition, 2004, Vols. 79:6-16.
7. Laprete, Jay. U.S. Farm Bill. Times Topics. [Online] The New York Times, December 31, 2012. [Cited: February 11, 2013.] http://topics.nytimes.com/top/reference/timestopics/subjects/f/farm_bill_us/index.html?offset=0&s=newest.
8. SNAP to Health. U.S. Farm Bill: Frequently Asked Questions. SNAP to Health. [Online] CSPC / Snap to Health, 2013. [Cited: February 11, 2013.] http://www.snaptohealth.org/farm-bill-usda/u-s-farm-bill-faq/.
9. USDA. Agricultural Marketing Service. Commodity Purchasing. [Online] January 22, 2013. [Cited: February 10, 2013.] http://www.ams.usda.gov/AMSv1.0/ams.fetchTemplateData.do?template=TemplateQ&navID=Commodity%20Purchasing%20Main%20Page&rightNav1=Commodity%20Purchasing%20Main%20Page&topNav=&leftNav=CommodityPurchasing&page=CommodityPurchasing&resultType=&acct=cmdtyprchs.
10. Environmental Working Group. United States Summary Information. EWG Farm Subsidies. [Online] 2012. [Cited: February 10, 2013.] http://farm.ewg.org/region.php?fips=00000.
11. Monke, Jim. Farm Commodity Programs: Base Acreage and Planting Flexibility. Washington, DC : Congressional Research Services, 2003.
12. Arizona Farm Bureau Federation. AG Facts. Arizona Farm Bureau. [Online] 2013. [Cited: February 15, 2013.] http://www.azfb.com/ag-facts.html.
13. Children of the Corn: The Renewable Fuels Disaster. The American. [Online] American Enterprise Institute, January 4, 2012. [Cited: February 15, 2013.] http://www.american.com/archive/2012/january/children-of-the-corn-the-renewable-fuels-disaster.
14. USDA Food & Nutrition Service. National School Lunch Program. USDA Food & Nutrition Serivce. [Online] June 21, 2012. [Cited: February 15, 2013.] http://www.fns.usda.gov/cnd/lunch/.
15. U.S. Department of Agriculture (USDA). USDA 2010 Dietary Guidelines. USDA Center for Nutrition Policy and Promotion: Dietary Guidelines for Americans. [Online] U.S. Government Printing Office, January 31, 2011. [Cited: January 5, 2013.] http://www.cnpp.usda.gov/Publications/DietaryGuidelines/2010/PolicyDoc/Chapter2.pdf.
16. ABC News. ABC News. Medical Unit. [Online] ABC News Internet Ventures, September 30, 2012. [Cited: April 14, 2013.] http://abcnews.go.com/blogs/health/2012/09/30/school-lunch-showdown-850-calorie-meals-compared/.
17. Ohio State University. Food Stamp Use Linked To Weight Gain, Study Finds. Science Daily. [Online] August 12, 2009. [Cited: April 13, 2013.] http://www.sciencedaily.com /releases/2009/08/090810122139.htm.
18. Food Prices and Obesity: Evidence and Policy Implications for Taxes and Subsidies. L Powell, F Chalupka. 1, Illinois : The Milbank Quarterly by Wiley Periodicals Inc, 2009, Vol. 87.
19. Jessica Todd, Biing-Hwan Lin. Amber Waves Online Magazine. U. S. Department of Agriculture Economic Research Service. [Online] September 2012. [Cited: February 10, 2013.] http://www.ers.usda.gov/amber-waves/2012-september/what-role-do-food-and-beverage-prices.aspx.
20. American Taxpayer Relief Act of 2012. U.S. Government Printing Office. [Online] Jan 12, 2012. [Cited: February 10, 2013.] http://www.gpo.gov/fdsys/pkg/BILLS-112hr8enr/pdf/BILLS-112hr8enr.pdf.
21. Bruch, Hilde. The Importance of Overweight. Michigan : Norton, University of Michigan, 1957.
22. Taubs, Gary. Good Calories, Bad Calories: Fats, Carbs, and the Controversial Science of Diet and Health. New York : Anchor Books, 2007. 978-1-40000-3346-1.
23. Role of Insulin in Endgenous Hypertriglyceridemia. GM Reave, RL Lerner, MP Stern, JW Farquhar. s.l. : Journal of Clinical Investigation, 1967, Vols. 46(II):1756-67.
24. High-Carb Diets Questioned. Kolata, G. 235(4785):164, s.l. : Science, 1987, Vol. 9.
25. U.S. Department of Health and Human Services. The Surgeon General’s Call to Action to Prevent and Decrease Overweight and Obesity. Washington, D.C. : U.S. Government Printing Office, 2001.
26. Global Burden of Obesity in 2005 and Projections to 2030. T Kelly, W Yang, C-S Chen, K Reynolds and J He. 8 July 2008, New Orleans : International Journal of Obesity, 2008, Vols. 32, 1431–1437. doi:10.1038/ijo.2008.102.
27. In The Face Of Contradictory Evidence: Report Of The Dietary Guidelines For Americans Committee. Adele H Hite, Richard D Feinman, Gabriel E Guzman, Morton Satin, Pamela Schoenfeld, Richard J Wood. 10, s.l. : Nutrition, 2010, Vol. 26. DOI: 10.1016/j.nut.2010.08.012.
28. A Dugan, F Newport. Gallup Wellbeing. Gallup. [Online] August 17, 2012. [Cited: April 13, 2013.] http://www.gallup.com/poll/156710/americans-say-low-fat-diet-better-low-car.aspx.
29. Low-fat dietary pattern and weight change over 7 years: the Women’s Health Initiative Dietary Modification Trial. . Howard BV, Manson JE, Stefanick ML, et al. s.l. : JAMA, 2006, Vols. 295:39-49. doi:10.1001/jama.295.1.39.
30. Healthy Nation Coalition. Healthy Nation Coalition. Healthy Nation Coalition. [Online] Adrienne Larocque, PhD, 2012. [Cited: March 8, 2013.] http://www.forahealthynation.org/.
31. Judith McGeary, Esq. Legislative Updates. The Weston A. Price Foundation. [Online] December 11, 2012. [Cited: March 9, 2013.] http://www.westonaprice.org/legislative-updates/policy-update-farm-bill-and-gmos.
32. The Sugar Association. Sugar and Your Diet. Sugar.org. [Online] 2012. [Cited: March 9, 2013.] http://www.sugar.org/sugar-and-your-diet/caloric-intake.html.
33. American Beverage Association. Obesity. American Beverage Association. [Online] 2013. [Cited: March 9, 2013.] http://www.ameribev.org/nutrition–science/obesity/.
34. Library of Congress. S.Amdt.2276 to S.3240. Congress.Gov. [Online] March 8, 2013. [Cited: March 9, 2013.] http://beta.congress.gov/amendment/112th-congress/senate-amendment/2276.
35. The American Heart Association. Policy Brief – The Farm Bill. The American Heart Association. [Online] 2012. [Cited: April 14, 2013.] http://www.heart.org/idc/groups/heart-public/@wcm/@adv/documents/downloadable/ucm_429110.pdf.
36. AMA: Report of Reference Committee . Malechek, Lindsay. 2011.
37. Wolf, Jim. Senate, House agriculture committees in deal to avert milk price spike. Reuters. Sun, Dec 30, 2012, 2012.
38. USDA. USDA Rural Progress Report. USDA. [Online] December 2006. [Cited: April 14, 2013.] http://www.rurdev.usda.gov/rd/pubs/2005_06_Prog_Report.pdf.
39. —. USDA Rural Developement 2011 Progress Report. USDA Rural Developement. [Online] December 2011. [Cited: April 14, 2013.] http://www.rurdev.usda.gov/Reports/RD%20Progress%20Report%202011–Smallest(2).pdf.
40. Slivinski, Stephen. Rural Subsidies. Cato Institute. [Online] July 2009. [Cited: March 9, 2013.] http://www.downsizinggovernment.org/agriculture/rural-subsidies.
41. Obesity prevention: the role of policies, laws and regulations. Swinburn, Boyd A. New Zeland : BioMed Central Ltd., 208, Vol. 5:12. 10.1186/1743-8462-5-12.
42. Begley, Sharon. As America’ss Waistline Expands, Costs Soar. Reuters. [Online] Thompson Reuters, April 30, 2012. [Cited: January 5, 2013.] http://www.reuters.com/article/2012/04/30/us-obesity-idUSBRE83T0C820120430.
43. The Costs of Obesity in the Workplace. E Finkelstein, M DiBonaventura, S Burgess, B Hale. 10, Illinois : Lippincott Williams & Wilkins, 2010, Vol. 52. doi: 10.1097/JOM.0b013e3181f274d2.
44. Rudd Center For Food Policy & Obesity. Search Legislation Database. Yale Rudd Center. [Online] Rudd Center, 2013. [Cited: January 5, 2013.] http://www.yaleruddcenter.org/legislation/search.aspx.
45. Walsh, Bryan. “Ending The War on Fat.” TIME Magazine. June 12, 2014.
46. Lucas, Frank D. “Agricultural Act Summary.” House Agricultural Committee. [Online] Jan 29, 2014. [Cited June 28, 2014.] http:// http://agriculture.house.gov/farmbill
The Fat Storage Control Mechanism
The only way to successfully loose weight is to modify or turn off the mechanisms that stimulate fat storage. For years we have been told that this was just a problem of thermodynamics, meaning the more calories you eat, the more calories you store. The solution was, thereby, eat less calories or exercise more, or both. We are taught in school that a 1 gram of carbohydrate contains 4 kcal, 1 gram of protein contains 4 kcal, and 1 gram of fat contains 9 kcal.
It’s easy to see that if I’m going to limit my calories, cutting out fat is the first step. For the last 65 years, we as a society have been doing just that, cutting out fat, exercising more and eating fewer calories. What has it done for us? It’s made us fatter! (1)

Some may argue that we really aren’t eating fewer calories and exercising more. But most people I have seen in my office have tried and tried and tried and failed and failed and failed to loose weight with this methodology. The definition of insanity is “doing the same thing over and over and expecting a different result.”
Most of my patients are not insane, they recognize this and stop exercising and stop restricting calories . . . ’cause they realized, like I have, that it just doesn’t work! If you’re one that is still preaching caloric restriction and cutting out fat, I refer you to the figure above and the definition of insanity . . .
So, if reducing the calories in our diet and exercising more is not the mechanism for turning on and off the storage of fat, then what is?
Before I can explain this, it is very important that you appreciate the difference between triglycerides and free fatty acids. These are the two forms of fat found in the human body, but they have dramatically different functions. They are tied to how fat is oxidized and stored, and how carbohydrates are regulated.
Fat stored in the adipose cells (fat cells) 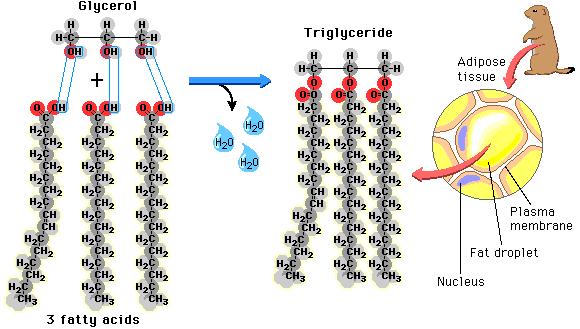 as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
as well as the fat that is found in our food is found in the form of triglycerides. Each triglyceride molecule is made of a “glyceride” (glycerol backbone) and three fatty acids (hence the “tri”) that look like tails. Some of the fat in our adipose cells come from the food we eat, but interestingly, the rest comes from carbohydrates
(“What! Fat comes from sugar?! How can this be?!!“)

We all know that glucose derived from sugar is taken up by the cells from the blood stream and used for fuel, however, when too much glucose is in the blood stream or the blood sugar increases above the body’s comfort zone (60-100 ng/dl), the body stores the excess. The process is called de novo lipogenesis, occurring in the liver and in the fat cells themselves, fancy Latin words for “new fat.” It occurs with up to 30% (possibly more if you just came from Krispy Kream) of the of the carbohydrates that we eat with each meal. De novo lipogenesis speeds up as we increased the carbohydrate in our meal and slows down as we decrease the carbohydrate in our meal. We’ve known this for over 50 years, since it was published by Dr. Werthemier in the 1965 edition of the Handbook of Physiology (2).
While we know that fat from our diet and fat from our food is stored as triglyceride, it has to enter and exit the fat cell in the form of fatty acids. They are called “free fatty acids” when they aren’t stuck together in a triglyceride. In their unbound state, they can be burned as fuel for the body within the cells. I like to think of the free fatty acids as the body’s “diesel fuel” and of glucose as the body’s version of “unleaded fuel.” The free fatty acids can easily slip in and out of the fat cell, but within the adipose cell, they are locked up as triglycerides and are too big to pass through the cell membranes. Lipolysis is essentially unlocking the glycerol from the free fatty acids and allowing the free fatty acids to pass out of the fat cell. Triglycerides in the blood stream must also be broken down into fatty acids 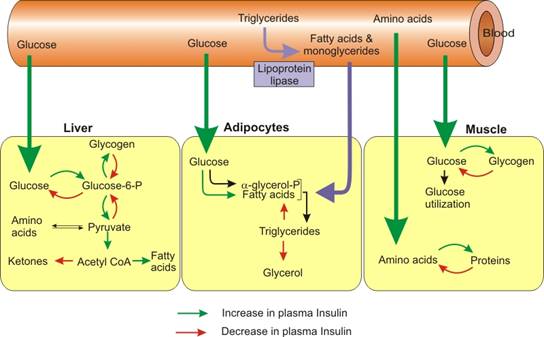 before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).
before they can be taken up into the fat cells. The reconstitution of the fatty acids with glycerol is called esterification. Interestingly, the process of lipolysis and esterification is going on continuously, and a ceaseless stream of free fatty acids are flowing in and out of the fat cells. However, the flow of fatty acids in and out of the fat cells depends upon the level of glucose and insulin available. As glucose is burned for fuel (oxidized) in the liver or the fat cell, it produces glycerol phosphate. Glycerol phosphate provides the molecule necessary to bind the glycerol back to the free fatty acids. As carbohydrates are being used as fuel, it stimulates increased triglyceride formation both in the fat cell and in the liver, and the insulin produced by the pancreas stimulates the lipoprotein lipase molecule to increased uptake of the fatty acids into the fat cells (3).
So when carbohydrates increase in the diet, the flow of fat into the fat cell increases, and when carbohydrates are limited in the diet, the flow of fat out of the fat cells increases.
Summarizing the control mechanism for fat entering the fat cell:
- The Triglyceride/Fatty Acid cycle is controlled by the amount of glucose present in the fat cells (conversion to glycerol phosphate) and the amount of insulin in the blood stream regulating the flow of fatty acid into the fat cell
- Glucose/Fatty Acid cycle or “Randle Cycle” regulates the blood sugar at a healthy level. If the blood glucose goes down, free fatty acids increase in the blood stream, insulin decreases, and glycogen is converted to glucose in the muscle and liver.
These two mechanisms ensure that there is always unleaded (glucose) or diesel fuel (free fatty acids) available for every one of the cells in the body. This provides the flexibility to use glucose in times of plenty, like summer time, and free fatty acids in times of famine or winter when external sources of glucose are unavailable.
The regulation of fat storage, then, is hormonal, not thermodynamic. Unfortunately, we’ve know this for over 65 years and ignored it.
We’ve ignored it for political reasons, but that’s for another blog post . . .
References:
1. James, W. J Intern Med, 2008, 263(4): 336-352
2. Wertheimer, E. “Introduction: A Perspective.” Handbook of Physiology. Renold & Cahill. 1965.
3. Taubs, G. “The Carbohydrate Hypothesis, II” Good Calorie, Bad Calorie. Random House, Inc. 2007, p 376-403.
Senior Texting Guide
About half of those who see me in my practice, here in Surprise, Arizona, are over the age of 60. It is a pleasure working with them, but I have found that there is a different acronym code for texting that is necessary. Maybe this will help. . .

Coconut Flour Conversion Chart
For those on a ketogenic or low-carbohydrate diet, whole wheat flour or almond flour is often substituted for with coconut flour. Found this cool chart at “Maria Mind Body Health.” Maria Emmerich has given me permission to post it here for you, my wonderful patients and followers.
We use many of Maria’s recipes in my home, but occasionally you may want to convert your own recipe and this chart will help. My wife is the cook in our family, and probably already knows how to do this, but for those just beginning your ketogenic journey, this will be a big help in recipe conversion.
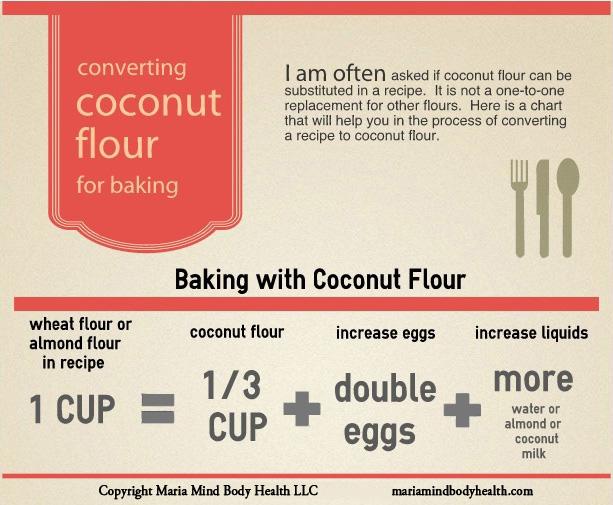
I’ve had patient’s ask me in the room how to substitute for flour. Here’s the answer. Remember, you have to double the eggs per cup. Thanks Maria!!
Insulin Resistance and The Horse

As a family practice physician and bariatrician, my job is to examine and treat the “Diseases of Civilization.” The Diseases of Civilization are those diseases arising out of the changes induced by industrializing and modernizing a society of people. These include diseases like diabetes, dyslipidemia (abnormal cholesterol), heart disease, hypertension, gout, vascular disease, & stroke. It is interesting that the so called Diseases of Civilization didn’t really appear on the scene until the early 1900’s. Yes, we have now identified some of these diseases in the early Egyptians, but to my point, as a society modernizes or industrializes, certain types of disease begin to arise. The Canadian cardiologist William Osler, one of the founding professors of John’s Hopkins Hospital, documented the first “syndrome” associated with narrowing of the arteries causing heart disease at the turn of the 19th century, and in 1912, the American Cardiologist James Herrick is credited with the discovery that narrowed arteries cause angina, a form of chest pain with exertion.
Today we know that underlying each of these diseases is the phenomenon of insulin over production, which seems to arise between five and twenty years prior to the onset of the Diseases of Civilization. Metabolic Syndrome, Dysmetabolic Syndrome or Syndrome X is the name we’ve given to the presentation of three or more of these diseases at once in one person. There is still argument as to whether insulin over production is the chicken or the egg, but what I see clinically has convinced me that insulin is culprit.
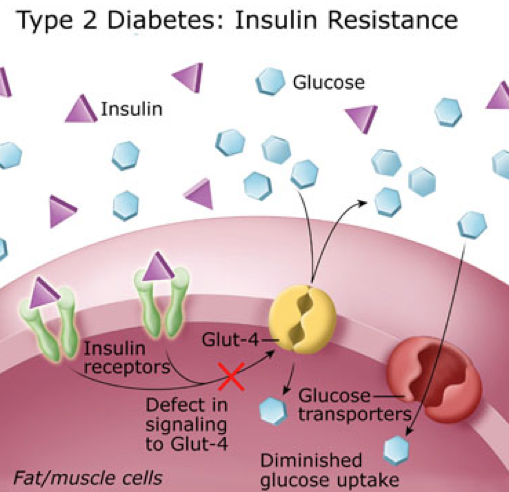
Insulin is a very powerful hormone that acts as a key, opening a door in just about every cell in the body, letting glucose (the primary form of fuel derived from carbohydrate) into the cell. For reasons that appear to be genetic, this key becomes “dull” in a portion of the population and does not unlock the door fast enough to lower the blood sugar. So, the body panics, and stimulates production of additional insulin, 2-10 times more in many people. However, the insulin that was produced initially, eventually kicks in. This extra insulin, acting at a slower rate, is the underlying culprit to the Diseases of Civilization.
How, you ask? Let me explain.
Insulin does more than just open the door for glucose.
1. Insulin causes weight gain. It turns on the storage of fat by activating an enzyme called lipoprotein lipase, pulling the triglycerides out of the cholesterol molecules and depositing them in the adipose tissue (fat cells).
2. Insulin raises cholesterol. It drives increased triglyceride production in the liver, especially in the presence of fructose.
3. Insulin triggers atherosclerosis. Triglycerides are essentially the passenger in the LDL (bad cholesterol) molecule. Higher triglycerides cause increased LDL production leading to increased atherosclerosis (narrowing of the arteries).
4. Insulin causes gout & kidney stones. Insulin increases uric acid production and in a round about way can increase calcium oxylate as well, increasing the risk of kidney stones and gout.
5. Insulin raises blood pressure. Insulin stimulates the retention of sodium, causing and increase in blood pressure.

6. Insulin makes inflammation worse. Insulin drives the inflammatory cascade and increases free radicals, and stimulates the inflammatory hormones causes arthritis, allergic rhinitis, psoriasis, dermatitis, and inflammatory bowel problems to be amplified.
My intent is not to demonize insulin. It is an essential hormone, however, when five to ten times the normal amount of insulin is being produced, you’re going to amplify the problems above by five to ten times normal. Type II Diabetes is really just a consequence of 15-20 years of over production of insulin.
This isn’t just something that affects humans. either. We have been seeing this in other species of the animal kingdom as well. Take for example my wife’s horse, Jazz. She’s a beautiful grey Arab/Saddle-Bred who kept having problems with laminitis, or more colloquially known as “founder.” Her diet consisted predominantly of alfalfa at the time, considered a moderate starch containing form of feed.
Laminitis is a progressively increasing tenderness to the hoof of horses or cattle that can be disabling and if not treated appropriately can cause permanent lameness in the animal. Recent literature in the veterinary world have identified that animal diets high in starch have a propensity to cause laminitis as well as colic. First identified in the equine community in the 1980’s with glucose tolerance tests, insulin resistance has been identified as a significant factor in hoof disease. The use of Corn, Oats, Barley or even Alfalfa as a primary form of feed for a horse with insulin resistance greatly increases the risk of laminitis.
Like Jazz, many horses in the arid Arizona climate are fed primarily with oats and alfalfa. Jazz was tested and found to have insulin resistance. Since Jazz has been placed on a much lower starch containing feed, she has had no further problems with laminitis. We converted all our horses to Bermuda grass.

Our family and our horses are all now on Low-Carb diets to some degree and have been for the last seven years. No further hoof problems with the horses, and 55 lbs of weight loss with normalization of cholesterol in their owner, me.

For those with interest, studies reveal feeds in order of the highest to lowest starch (carbohydrate) content to be: Sweet Feed, Corn, Oats, Barley, Wheat Bran, Beat Pulp, Alfalfa, Rice Bran, Soybean hulls, Bermuda Grass. Take a look the Low Carbohydrate help section in the menu above to see the carbohydrate content of many of the foods for human consumption.
It’s time we recognize that our diet and lifestyles have lead us to the Diseases of Civilization, and those diets and lifestyles have even effected our animals.
The Terminator is Obese?
 When you visit your doctor, he or she will probably measure your height and your weight. Then a Body Mass Index (BMI) will be calculated and placed on your chart. The BMI has actually become one of the standard “vital signs” required at a doctor visit over the last five years. This was not something that physicians started measuring on their own, it is a required measurement most health insurance plans insist upon before they will pay for the visit. BMI is an interesting and arguably worthless measurement. It was developed by a Belgian physicist by the name of Adolphe Quetelet some time between 1830-1850. Quetelet was a “Social Physicist,” trying to combine probability and statistics with the study of sociology (1). BMI was originally called the “Quetelet Index” and was designed specifically to measure averages among large populations in sociology or epidemiological studies (2).
When you visit your doctor, he or she will probably measure your height and your weight. Then a Body Mass Index (BMI) will be calculated and placed on your chart. The BMI has actually become one of the standard “vital signs” required at a doctor visit over the last five years. This was not something that physicians started measuring on their own, it is a required measurement most health insurance plans insist upon before they will pay for the visit. BMI is an interesting and arguably worthless measurement. It was developed by a Belgian physicist by the name of Adolphe Quetelet some time between 1830-1850. Quetelet was a “Social Physicist,” trying to combine probability and statistics with the study of sociology (1). BMI was originally called the “Quetelet Index” and was designed specifically to measure averages among large populations in sociology or epidemiological studies (2).
BMI = mass (kg) / [height (m)]²
However, it wasn’t Quetelet that got BMI placed on the medical chart. BMI was made popular by the infamous Ancel Keys (the same Ancel Keys responsible for the flawed Seven Countries Study) in his July 1972 article published in the Journal of Chronic Disease. Ancel Keys, himself, explicitly stated that BMI was designed specifically for population studies, and inappropriate for evaluation of individual health (2). But, because of the ease of measurement, and the fact that Life Insurance companies had been using BMI to set your insurance premiums since the 1970’s, Health Insurance companies adopted it as a measure of overall health. In 1985, because BMI found great favor in epidemiological research, the National Institutes of Health (NIH) adopted it as the method to identify and define obesity in patients. And, in 1998 the NIH identified the BMI cutoffs – 25 for overweight, 30 for obesity – as easy numbers that could be remembered and used to counsel patients on weight reduction and health.
 The problem with BMI is that it doesn’t actually identify a person with excessive fat accumulation. BMI is a height to weight ratio. It doesn’t account for fat at all. Using the NIH guidelines, the Terminator, with an estimated BMI of 31, would be considered obese. (You try telling the Terminator that he is obese, and see what happens.) Because, muscle weighs twice as much when compared to an identical volume of fat, Mr. Schwarzenegger (or anyone with increased muscle mass), will have a higher scale weight. This raises the BMI calculation, giving a false indication of increased health risk.
The problem with BMI is that it doesn’t actually identify a person with excessive fat accumulation. BMI is a height to weight ratio. It doesn’t account for fat at all. Using the NIH guidelines, the Terminator, with an estimated BMI of 31, would be considered obese. (You try telling the Terminator that he is obese, and see what happens.) Because, muscle weighs twice as much when compared to an identical volume of fat, Mr. Schwarzenegger (or anyone with increased muscle mass), will have a higher scale weight. This raises the BMI calculation, giving a false indication of increased health risk.
I was recently asked about a study published in The American Journal of Medicine that was recently commented on in Scientific American regarding BMI vs Muscle Mass as a predictor of longevity. The assumption is that just because your doctor measures BMI, it must be a great tool predicting health outcomes. The assumption is absolutely wrong. We know from multiple studies, including the article sited above, that increase muscle mass increases overall health, decreases the likelihood of insulin resistance and diabetes, reduces the risk of heart disease, and extends longevity. How can a measure of height to weight predict longevity? It can’t. The only reason BMI is on the medical chart, thanks to the NIH, is so that the physician gets paid. 
In actuality, the most effective way of measuring a persons health is to simply measure body fat. This can easily be done by measuring waist circumference with an inexpensive tape measure. It can also be done with a simple bioelectrical impedance measurement. The gold standard for measuring body fat is to strip you down naked and dip you in a tub of water, measuring the water displacement. (I have very few patient’s that will return to my office after doing that, so we don’t use it very often, but it is effective).
The answer to the question is “NO,” the Terminator is NOT obese. And, if he shows up in my office, I’m not going to comment about his BMI.
1. Eknoyan, Garabed (2007). “Adolphe Quetelet (1796–1874)—the average man and indices of obesity”. Nephrology Dialysis Transplantation 23 (1): 47–51.
2. Keys, Ancel; Fidanza, Flaminio; Karvonen, Martti J.; Kimura, Noboru; Taylor, Henry L. (1972). “Indices of relative weight and obesity”. Journal of Chronic Diseases 25 (6–7): 329–43
The Self-Discipline Muscle
Many patients come to my office desiring to loose weight, but complain of no self-control. They feel they cannot loose weight because they don’t have the willpower. Willpower, or self-control, is an elusive and mysterious thing. “If only I had more self-control,” I hear people say, “I could . . . ” exercise regularly, eat right, avoid drugs and alcohol, save for retirement, stop procrastinating, achieve a noble goal, or loose weight. A 2011 American Psychological Association study reveals that almost 30% of those interviewed felt that lack of willpower was the greatest barrier to making a change in any of these areas.
So what is “willpower” or “self-control?” It is the ability to resist short-term temptations in order to fulfill a long-term goal. 
I meet and work with people every day who feel they have no willpower. In actuality, will power and self-control are learned behaviors that develop over time. Anyone can have willpower, you just have to understand how willpower in certain areas can be strengthened and what makes it weak. In fact, a 2005 study showed that self-discipline or willpower was more important than IQ in academic successes. This study also found that increased self-discipline lead to less binge eating, higher self-esteem, higher grade point averages, better relationship skills and less alcoholism. Fascinating isn’t it!?
The answer can be found in a quote from Henry P Liddon, “What we do upon some great occasion will probably depend on what we already are; and what we are will be the result of previous years of self-discipline.” This means that willpower or self-control can be learned or improved. How, you ask?
First, you must establish and write down a reason or motivation for change. In addition, that change must fulfill a clear goal. Just wanting to loose weight isn’t good enough. You have to be motivated because of a consequence that arises from the obesity or overweight. And, you “loosing weight” isn’t a clear goal. You must set a weight reduction goal. It has to be clearly written down with your motivational reason. Willpower or self-control cannot begin to form until these two steps occur.
Second, you must begin to monitor your behavior toward that goal. When it comes to weight loss, I ask every one of my patient’s to keep a diet journal. In this journal they are asked to write down every thing they eat and drink. The night before, they are to write down their plan for tomorrow’s meals, then the next evening, they account for their success or failure by journaling on that same page what they actually ate and drank, then after comparing what they did, they plan for tomorrow and journal why they were successful or why they weren’t. It’s the last part that is so powerful, a short 3-5 minutes of self-introspection. Self-introspection is the key to behavioral change. It is the key that allows a person to see their habits and then make very small changes that break bad habits, solidify good habits and strengthens willpower.
Third, willpower is developed over time. It is developed by being accountable to ones-self on very little things every single day. But it MUST be written down. If I planned to eat bacon and eggs for breakfast and I didn’t, why? When I look at my day, I may realize that I went to bed too late to get up early and cook bacon and eggs. So, instead, I ate a yogurt that was in the fridge. I am accountable to myself. If I plan to eat bacon and eggs tomorrow, I must either go to bed earlier, prepare them the night before, or throw out the yogurt . . . so not to be a temptation again. This is written down and I make a very small change tomorrow.
 Over time, this self-introspection becomes easier and easier, to the point that you do it sub-consciously. It is this sub-conscious self-introspection and change will be seen by others as self-control or willpower. Just like a working or strengthening a muscle, recording short goals and and accounting for them makes your self-discipline stronger. The self-discipline muscle becomes more powerful. In time, a split second decision not to binge on that piece of cake will be seen as strong willpower by those around you. You’ll recognize that it’s just flexing your self-discipline muscle.
Over time, this self-introspection becomes easier and easier, to the point that you do it sub-consciously. It is this sub-conscious self-introspection and change will be seen by others as self-control or willpower. Just like a working or strengthening a muscle, recording short goals and and accounting for them makes your self-discipline stronger. The self-discipline muscle becomes more powerful. In time, a split second decision not to binge on that piece of cake will be seen as strong willpower by those around you. You’ll recognize that it’s just flexing your self-discipline muscle.
So, my next question to you is . . . where’s your diet journal?
Vitamin D's Effect on Weight and Obesity
Vitamin D plays an interesting role in may aspects of human health. It plays a role in disease prevention including osteoporosis, some cancers, autoimmune disorders, hypertension, diabetes and has recently been found to effect weight loss.
 What is Vitamin D? It is an oil-soluble (fat-soluble) vitamin that helps in the absorption of calcium and phosphorus in the intestine and suppresses parathyroid hormone (PTH), the hormone that stimulates bone resorption (breakdown). Vitamin D also plays a role in muscle function and in the immune system, but our understanding in these roles are still limited. (1)
What is Vitamin D? It is an oil-soluble (fat-soluble) vitamin that helps in the absorption of calcium and phosphorus in the intestine and suppresses parathyroid hormone (PTH), the hormone that stimulates bone resorption (breakdown). Vitamin D also plays a role in muscle function and in the immune system, but our understanding in these roles are still limited. (1)
Vitamin D can be found in fatty fish, cod-liver oil and eggs. In the United States, cow’s milk is supplemented with Vitamin D and this is often the source from which most people obtain it. Deficiency in Vitamin D often occurs from lack of sun exposure, inadequate intake, surgery to or damage of the intestines ability to absorb, or from kidney or liver damage resulting in problems processing Vitamin D. Recent studies reveal that obesity is a major factor in altering the way the body uses Vitamin D and stimulates PTH.
I find that about 30-40% of my patients are Vitamin D deficient. Many researches claim this is due to poor sun exposure or the use of sun screens, however, I live in Arizona. Sun “over exposure” is usually the problem here, yet I still find that 30-40% of my patients are deficient. My patients should be able to get enough sunlight walking from their cars to the grocery store entrance. I disagree that “lack of sun exposure is the cause.” Although our current labs claim vitamin D levels should be above 20 ng/dl, I find people do not get the needed effect until 25 Hydroxy-Vitamin D levels should are greater than 32-35 ng/dl.
Poor Vitamin D intake is usually the problem.
Our bodies convert 25 Hydroxy-Vitamin D into the active molecule 1,25 Dihydroxy-Vitamin D. Recent studies reveal that higher Body Mass Index (BMI) leads to lower conversion of 25 Hydroxy-Vitamin D to 1,25 Dihydroxy-Vitamin D. (2,3)
Simply adding 25 Hydroxy-Vitamin D as a supplement frequently helps with weight management in many of my patients. Supplementation with 1000-2000 IU is often adequate. Higher doses should be discussed with your doctor.
References:
1. C P Earthman, L M Beckman, K Masodkar and S D Sibley. The link between obesity and low circulating 25-hydroxyvitamin D concentrations: considerations and implications.International Journal of Obesity (2012) 36, 387–396; doi:10.1038/ijo.2011.119; published online 21 June 2011.
2. Frost M, Abrahamsen B, Nielsen TL, Hagen C, Andersen M, Brixen K. Vitamin D status and PTH in young men: a cross-sectional study on associations with bone mineral density, body composition and glucose metabolism. Clin Endocrinol (Oxf) 2010; 73: 573–580.
3. Konradsen S, Ag H, Lindberg F, Hexeberg S, Jorde R. Serum 1,25-dihydroxy vitamin D is inversely associated with body mass index. Eur J Nutr 2008;47: 87–91.
Low-Carb Diets . . . Bad For Health?

Interview with Howard Harkness of "N=1 Health"

While on the 2014 Low-Carb Cruise a few weeks ago, I had the wonderful pleasure of being interviewed by “N=1 Health‘s” Howard Harkness. We had very nice conversation and discussed a number of topics relating to obesity medicine, weight loss, carbohydrate restriction and some of the history of medicine. Take a look at the interview here on N=1 Health.
Thanks, Howard!

How Does Stress Cause Weight Gain?
How are your stress levels lately? Are you struggling with your finances? Struggling with your job? Do you have troubles in your personal relationships? Are you carrying a heavy load in school? Do you have a horse that just won’t behave?
Many of my patients will routinely experience weight loss plateaus due to stress. Most of them want to know how and why this occurs. The simple answer is this: our bodies are designed with a “fight or flight” response.

If you’re in the woods and you stumble upon a bear, the sudden recognition of significant danger will stimulate an immediate release of protective hormones into your blood stream including adrenaline and cortisol. (Your brain also know that those extra few donuts you ate will make you quite the tasty treat for the bear.)
Fight or Flight Causes Glucose in the Blood Stream
Adrenaline increased your heart rate, dilates the blood vessels to your muscles and increases your respiratory rate. Cortisol is the hormone that stimulates increased glycogen release from the liver. Glycogen is a form of sugar made available so that you can immediately fight the bear or run from the bear. The glycogen response raises your insulin level so that that fuel can be pulled right into the cells needing it. The adrenalin and cortisol, among other hormones, are released so that blood can be shunted from your stomach and intestines to your muscles and brain to more effectively enable you to finish fighting the bear, or out run that drooling growling bear hot on your heels.
Modern Bears
 Most of us will never “stumble across a bear.” However, your boss may confront you about how you handled a recent assignment or may drop an extra pile of work on your desk. You may run short on your finances this month, have a serious disagreement with your significant other, or someone may cut you off in traffic causing a near accident. Any or all of these stimulate the identical “fight or flight” response. Whether it is an actual bear or the stress from traffic, the same adrenalin and cortisol response occurs.
Most of us will never “stumble across a bear.” However, your boss may confront you about how you handled a recent assignment or may drop an extra pile of work on your desk. You may run short on your finances this month, have a serious disagreement with your significant other, or someone may cut you off in traffic causing a near accident. Any or all of these stimulate the identical “fight or flight” response. Whether it is an actual bear or the stress from traffic, the same adrenalin and cortisol response occurs.
Chronic Cortisol Release & Weight Gain
How does that keep you from loosing weight? The elevated cortisol causes a cascade effect raising your insulin levels. Insulin will remain effectively elevated in the blood stream for the next 2-12 hours. Insulin is the primary hormone driving and stimulating weight gain. If you’ve had 2 or 3 stressful events throughout the day, and you have not had the opportunity to physically burn off these stress response hormones, your body will store and/or continue to gain weight throughout the entire day. If you have been trying to loose weight, the spike in the insulin from this cortisol cascade halts the weight burning process and may actually bump you out of ketosis (the process by which we burn fat as the primary fuel source) for the next 4-12 hours.
Mitigating Daily Stress
How do you prevent this from happening? A simple 15-20 minute walk 3-5 times per week is enough to decrease the stress hormone surge that occurs from a “fight or flight” response. Any regular exercise program will decrease these stress hormones. Adequate sleep also decreases these hormones.
Berberine, the active ingredient in tumeric, is also helpful in controlling blood sugar spikes and helping those with insulin resistance to handle stress and inflammation. I’ve been using berberine daily for years personally and with many of my patients. I love it so much, I designed my own formulation. You can find it along with my other supplement line at ketoliving.com.

If your job, school or life is stressful, incorporating an exercise program as simple as a daily walk for 15-20 minutes per day will keep the proverbial “bear in the woods” from catching up to you because of your weight. Controlling your blood sugar is the other key. The correct diet and supplements play a huge role combined with exercise.
Check out my diet page if you’d like a copy of my ketogenic dietary program. Check out my YouTube page for hundreds of free videos and DocMuscles.Locals.com for additional information for my followers. And, look at my membership programs available here.
The Real . . .

Mom’s Cream Cheese Waffles
Mother’s Day is a great event in our home, and traditionally, it is a chance to make breakfast for Mom.
In our home, Mom has always loved waffles. But changing to a low carbohydrate diet put a damper on the waffles for a while, until my sweet wife found and perfected the following recipe. (She adapted this recipe fromJennifer Eloff’s Cream Cheese Bran Waffle recipe found in her book, Splendid Low Carbing for Life Vol 1.) These waffles are amazing! They are now lovingly referred to in our home as “Mom’s Cream Cheese Waffles.”
Because I’ve found that Splenda© spikes the insulin and slows weight loss in a significant percentage of my patient’s we’ve changed up the sweetener below.
Breakfast for Mother’s Day in our home consisted of Mom’s Cream Cheese Waffles, freshly grilled thick slice bacon and strawberry flavored homemade whipped cream to top off the waffles and was easily prepared by my 13 year old daughter. It’s a perfect Low Carb Mother’s Day meal that’ll satisfy the waffle craving and still give the gift of “ketosis”.
Enjoy!

Mom’s Cream Cheese Waffles:
16 oz regular cream cheese (softened)
6 eggs
1 cup Carbalose flour
1 cup wheat germ
1/4 cup heavy cream
1/4 cup water
1/2 cup erythritol
1-2 drops liquid Stevia (add to taste)
1 tsp baking soda
1 tsp baking powder
1/4 tsp salt
In a food processor or electric mixer, blend the cream cheese until smooth. Add the eggs and continue to blend. Add the Carbalose flour, wheat germ, cream, water , Splenda, baking soda, baking power and salt. Continue to blend.
Pour 1/4-1/2 cup onto hot greased waffle iron. Close and cook for approximately 3 minutes.
Yeild: 12-16 “plate sized” waffles
1 Waffle: approx. 7g protein, 9g fat, 1g carbs
Low Carb Cheese Cake
My amazing wife, among her many talents, makes a wonderful low carb cheese cake. She has taken the recipe found in Maria Emmerich’s “Secret Weight Loss Recipes” and modified it to our family’s taste. It has quickly become one of my family’s favorites.
 |
| Low Carb Cheesecake = 1 gram carb per serving Individual spring-form serving pans |
Crust:
2 cups almond flour
1/4 cup coconut flour
1/2 cup butter melted
Pinch of salt
1/2 cup erythritol
Mix and press into spring-form pan.
5 (8 oz) packages cream cheese, softened
1 cup erythritol and 1 tsp liquid Stevia
1 TBS vanilla
1/2 cup whey Protein
1 cup sour cream
3 eggs
Preheat oven to 350F. Mix cream cheese, sweetener, protein and vanilla with an electric mixer until blended. Add eggs one at a time, mixing on low after each until blended. Blend in sour cream and pour over crust. Place a pan of water on the lower rack place cheesecake on rack above. Bake for approximately 45 minutes until set. Watch carefully!
Refrigerate overnight.
Freezes well too!
My wife will often bake them in individual sized pans (as in the picture above) so that I can pull one out of the freezer, let it thaw and cover it in whip cream and a sprinkle of berries. Tastes fantastic!
One serving is = 1 gram of carbohydrate.
Low Carb Chocolate Chip Cookies
Low Carb Chocolate Chip Cookies
I love chocolate chip cookies! However, over the last seven years, as I have followed a low carbohydrate diet I have not been able to indulge my chocolate chip cookie craving — until recently.
My gorgeous and very ingeniousness wife has perfected her chocolate chip cookie recipe and – Oh, WOW . . .are they good.
Warm, tasty chocolate chip cookies that are actually good for you, served up by a beautiful blond in a very cute apron. . . I think this is what heaven is like.

Here is a snapshot of the remaining batch my wife made at our house the other day before they got eaten. Boy, are they good. Here is the recipe:
Low Carbohydrate Chocolate Chip Cookies
1 tsp vanilla
2 eggs
2 sticks (1 cup) of butter, softened
1/2 cup Sweet Perfection
1/4 cup erythritol
1/4 cup Just Like Sugar (chicory root sweetener)
1 tsp salt
1 tsp baking soda
1 tsp baking powder
1 1/2 cup almond flour
1 cup coconut flour
1/2 cup Carbalose flour
2 ChocoPerfection Milk Chocolate bars chopped
Mix the vanilla, eggs, butter and sweeteners until creamy or fluffy. Add in all dry ingredients and mix. Add chocolate and mix. Place dough on parchment paper covered cookie sheets in 2 tsp sized scoops.
Bake at 350 degrees for 8-10 minutes.
Makes 45-50 cookies
(~ 2 net carbohydrates per cookie)
Enjoy!!
What's Yours . . . ?


How To Start Your Weight Loss Journey
Weight loss, better put as “fat loss,” is a journey. A journey brought you to where you stand today, and it will be an even more exciting journey getting back to that size you’ve been daydreaming about. So, how do you most effectively start down the path of this journey?
That is the great question. It is the most important question I get asked every day. In the words of Napoleon Hill, “Desire is the starting point of all achievement, not a hope, not a wish, but a keen pulsating desire which transcends everything.”
First, Know Where You Are Coming From.
A journey requires knowing where you were, were you are today and where you want to go. Get a journal and weight yourself. Write it down and then check your weight every 3-5 days. DO NOT weigh yourself every day. I repeat DO NOT weight yourself every day. This can be discouraging because is is normal to fluctuate 2-5 lbs every day based on meals and water intake. Many people see this fluctuation and thing they are failing, then give up. The journal helps this. Recording your weight helps you see the progress.
The journal is also to help you record what you eat. Plan and record your meals IN YOUR JOURNAL. If you are being followed by a weight loss specialist, they will want to see your journal. If you are seeing me in my office, bring the journal with you to EVERY visit. Record every thing you eat.  And, record your water intake. I am amazed at how many of my patient’s are dehydrated and just putting water back into their systems help them loose weight.
And, record your water intake. I am amazed at how many of my patient’s are dehydrated and just putting water back into their systems help them loose weight.
Second, Plan Your Day.
Planning is the key to weight loss on any program.
You should plan your exercise and plan your meals the night before. Failing to plan is really just planning to fail. Your plan should include 1) keeping carbohydrate intake less than 20 grams per day and 2) getting adequate proteins to match your goals.
{kind=link}
Third, What’s the Underlying Cause of Your Weight Struggles?
You can’t effectively lose weight unless you understand why you are gaining weight. Two thirds of my patients are hyperinslinemic – they produce too much insulin in response to any sugar, starch or carbohydrate. This is also called “insulin resistance.” This is the primary cause of weight gain in 85% of the population. People produce between two to thirty times the normal amount of insulin in response to a piece of bread or a bowl of cereal. When they eat a single piece of bread, their bodies respond as if they ate the whole loaf. If they eat a bowl of cereal, their bodies respond as if they ate the whole box of Captain Crunch.
This variable over production of insulin is why some patient’s gain more weight than others eating and exercising the same way. Your doctor can easily identify this through blood work. For starters, if your waist circumference is larger than 40 inches as a male or larger than 35 inches as a female, you’re probably insulin resistant. Most men complain they don’t have a tape measure to measure their belly, so I tell them if they walk toward the wall and the first thing that touches the wall is their belly, “you’re insulin resistant.”

Skin tags or the presence of thickened browning skin at areas of skin folds (acanthosis nigricans) are classic signs of insulin resistant.

Hypoglycemia or low blood sugar is another sign of hyperinsulinemia or insulin resistance. This is where a person gets light headed or dizzy 2-5 hours after eating a meal that contains mainly starch or sugar.
Insulin resistance requires a dramatically different dietary approach than the standard diets we’ve been taught all our lives. The “heart healthy” diet, DASH diet, vegetarian/vegan diet, low fat diet or calorie restricted diet just don’t work with hyperinsulinemia or insulin resistance. If you are insulin resistant, a low fat/calorie restricted diet will not be very effective, and you may even gain weight with this approach as many of my patients have experienced.
If you have any of these symptoms, you need to follow up with your doctor or weight management specialist. Find out where your insulin levels are in relationship to your diet. Losing weight is possible. You can get started here with my ketogenic dietary program.
As this is a journey, it will probably have a number of twists and turns that are often made easier with a road map. Getting checked out with your doctor, and evaluating your metabolic status is your road map. Check out the health programs I offer to my patients to get this road map. I’ve also produced hundreds of videos on YouTube and DocMuscles.Locals.com to help you down the road. Either way, enjoy the journey!!
Fat Thoughts . . .
As a bariatrician, I think about fat all the time. I guess you could say I have a lot of “fat thoughts.”
I frequently hear patient’s tell me, “Dr. Nally, I’m eating RIGHT, but I’m just NOT losing weight!”

If you’re not losing weight, your not eating correctly. 99% of your weight loss success is related to your diet. We have been poorly misinformed over last 40 years as to what a “correct” diet contains. We’ve been told to follow a low fat diet for the last 40-50 years. However, it is very apparent as patient’s follow a low fat diet that only a small percentage of them have success in weight loss, and the majority actually gains more weight and remains significantly hungry. When you look at the body’s physiology, fat restriction only stimulates increased hunger. The intake of any form of carbohydrate, whether that be simple or complex, stimulates an insulin response. Based on our genetics, that insulin response can be variable. some of us respond normally and others respond with between 2-10 times the normal insulin surge. Insulin is actually the hormone that drives weight loss or weight gain.
You and I will not be able to effectively lose weight until we control the response of insulin, and this can only be done through carbohydrate restriction.
Inflammation Killer – A Ketogenic Diet

A recent study published in the Annals of Internal Medicine demonstrate significant improvement in overall inflammation in type II diabetic patients following a carbohydrate restricted diet versus a low fat calorie restricted diet. Another bit of proof demonstrating what I’ve been seeing in my office over the last 8 years. The study reveals significant improvement in glycemic (blood sugar) control in those following a low carbohydrate diet as well as significant lowering of C-reactive protein, IL-1 and IL-6 over those following a low fat diet. You can see the study here.
Ketogenic Diet Reduces Diabetic Nephropathy
A common problem that arises in patients with diabetes is that of kidney disease or “nephropathy.” Nephropathy is defined as damage to or disease of the filtering system of the kidney. In diabetic patients, they commonly begin to loose the ability to adequately filter and retain microscopic protein needed in the body. As the blood sugar and insulin levels progressively rise over time, damage to the delicate filtering system of the kidneys occur.
they commonly begin to loose the ability to adequately filter and retain microscopic protein needed in the body. As the blood sugar and insulin levels progressively rise over time, damage to the delicate filtering system of the kidneys occur.
Very impressive results revealing improved kidney function were found in both Type I and Type II diabetic mice placed on a low carbohydrate, or ketogenic, diet in just and 8 week period of time. The nephropathy (reduced passage of protein through the kidneys) was completely reversed in all the mice. This is the first in what I suspect will be a series of articles showing that ketogenic diets have significant effect on reversal of age related and diabetic tissue damage. See the article here.
I Like My Green Eggs & Ham . . .

You know, Dr. Seuss was right, the whole egg is actually good for you.
A recent study from the University of Connecticut demonstrated that eating the whole egg actually decreases LDL (the bad cholesterol) sub-particles and insulin resistance in Metabolic Syndrome better than the egg white or the egg substitute.
I like green eggs and ham!
I do!! I like them, Sam-I-am!
And I would eat them in a boat!
And I would eat them with a goat…
And I will eat them in the rain.
And in the dark. And on a train.
And in a car. And in a tree.
They are so good so good you see!
Fat Thoughts on Cholesterol
As a medical bariatrician and family practitioner specializing in low-carbohydrate diets, I often see the panic stricken look on people’s faces when they look at their cholesterol profiles just after starting a carbohydrate restriction life-style.
First, it is very important to understand that if you check your cholesterol within the first 4-6 weeks of dietary changes, there will be a transient rise in the cholesterol profile as your adipose tissues (fat cells) release your new fuel source into the blood stream and the mitochondria in the one trillion cells in your body convert from the use of glucose to the use of ketones (derived from triglycerides) as the primary fuel source. This is not a problem as the body is designed to handle this increase in triglyceride and cholesterol. I explain to patient’s that we are essentially making the figurative change from “un-leaded fuel to diesel fuel.”
Second, the standard cholesterol profile does not give you a true picture of what is occurring at a cellular level. The standard cholesterol panel checks Total cholesterol (all the forms of cholesterol), HDL (the good stuff), LDL-C (the bad stuff) and triglycerides. It is important to recognize that the “-C” stands for a calculation usually completed by the lab.

Total cholesterol, HDL and triglycerides are usually measured and LDL-C is measured using the Friedewald equation [LDL = total cholesterol – HDL – (triglycerides/5)].
Third, it is also important to realize that HDL and LDL are actually transport molecules (the buses for the triglycerides (the passengers). HDL is taking triglycerides to the fat cells and LDL is taking triglycerides from the fat cells to the muscles and other organs for use as fuel.
When you being a low carbohydrate diet, your blood glucose availability as the primary fuel source drops and triglycerides become the primary source. It takes your body 4-6 weeks to increase the number of mitochondria necessary to effectively use triglycerides as the primary fuel. (This is why many athletes and patients who are active will feel slightly sluggish during their exercise for the first few weeks).
Once your body accommodation to the new fuel, there will be a notable drop in LDL-C and a rise in the HDL.
But this still doesn’t answer the question and relieve the panic seen above. A deep sigh and the look of relief occurs when I explain that LDL-C doesn’t give us the real story.
To make it simple and understandable, LDL is made up of three main sub-types big fluffy ones, medium sized ones, and small dense ones. It’s the small dense ones that contain lipoprotien A [Lp(a)] found in increased vascular risk. Recent studies reveal that heart disease and atherosclerosis is caused by the small dense LDL molecules.
A low carbohydrate diet causes the small dense cholesterol to drop and there is a rise in the two other sub-types This shift in sub-types can actually elevate the Total Cholesterol number and occasionally the LDL-C.
If you are following a low carbohydrate diet, get your cholesterol levels checked. It is more ideal to get an NMR Lipoprofile or VAP Cholesterol test that will give you an LDL particle number and this can be explained more fully by your doctor.
Now, off to the fridge . . . where did I put that package of bacon . . . ?
FDA Approves Avantame (New Artificial Sweetener)
 The FDA approved an intense new artificial sweetener, Advantame. Because of its chemical similarity, Aspartame now has a super sweet cousin. This sweetener, 20,000-37,000 times more sweet than table sugar (sucrose), is found in powder form and dissolves in water. However, it does partially break down when exposed to heat or used in heated drinks, so it may not be that great for cooking.
The FDA approved an intense new artificial sweetener, Advantame. Because of its chemical similarity, Aspartame now has a super sweet cousin. This sweetener, 20,000-37,000 times more sweet than table sugar (sucrose), is found in powder form and dissolves in water. However, it does partially break down when exposed to heat or used in heated drinks, so it may not be that great for cooking.
Similar to Aspartame, one of the breakdown metabolites is phenylalanine, implying that those with sensitivity to phenylalanine or PKU may need to avoid it, however, the amount of phenylalanine produced when ingested was felt to be fairly negligible.
My interest was peaked by the fact that Advantame does not raise blood sugar or insulin levels in the multiple animal and three humans studies reviewed here and here. This implies that it probably won’t cause weight gain and the studies in animals actually revealed some negligible weight loss.
The FDA claims this is a very safe artificial sweetener due to it’s intense sweetness and requirement for only small quantities to be effective. In fact, Josh Bloom from the American Council on Science and Health was quoted saying that, “About the only way this stuff could harm you is if you were run over by a truck that was delivering it.”
From the perspective of weight loss, this may be another sweetener that could be used effectively on a carbohydrate restricted diet.
What Would You Choose?
